
記住我




The study sample (n = 2755) consisted of 1305 men and 1450 women, with mean (SD) ages of 69.5 (9.2) years for men and 69.4 (9.2) years for women. Table 1 presents the characteristics of participants by MetS status. Approximately 39.2% of the participants were diagnosed with MetS. Among the components of MetS, high BP and high WC exhibited the highest prevalence, affecting 69.7% and 61.6% of participants, respectively. Participants diagnosed with MetS were more likely to be Black or Hispanic, have lower levels of education, engage in less physical activity, and have a lower proportion of current alcohol consumers, compared to those without MetS. Additionally, individuals with MetS exhibited higher BMI, WC, SBP, TG, FBG, NC, LC, and PC, but lower HDL-C than those without MetS.
Table 1 Demographic, clinical, and lifestyle characteristics of participants stratified by metabolic syndrome status: MESA cohort (2010–2012)Association between SII and MetSTable 2 displays the association between the LnSII and MetS. In the crude model, no significant association was found between the LnSII and MetS. However, in model 2 (adjusted for age, sex, and race), and model 3 (all variables were adjusted), LnSII showed positive correlations with MetS (OR: 1.19; 95% CI: 1.03–1.38, and 1.23; 1.05–1.46, respectively). When LnSII was analyzed as a categorical variable (quartile), after adjusting for all confounders in Model 3, participants in the quartile 3 had a 47% higher prevalence of MetS (1.47; 1.14–1.89), compared to those in the quartile 1 (P trend = 0.041). The RCS curve, based on the Model 3, confirmed a linear relationship between LnSII and MetS (P for nonlinearity = 0.123) (Fig. 2).
Table 2 Association between systemic immune-inflammation and metabolic syndrome in whole population; MESA cohort (2010–2012)Association between SII and components of MetSTable 3 illustrates the association between the LnSII and the five components of MetS across different models. We found that LnSII was positively associated with high FBG (1.23; 1.05–1.44) and high BP (1.37; 1.15–1.63), but not with the other components. On the categorical scale of LnSII, participants in the highest LnSII quartile (quartile 4) had 32% higher prevalence of elevated FBG compared to those in the lowest quartile (quartile 1) (P trend = 0.021). For high BP, participants in the quartile 4 of SII exhibited a 63% higher prevalence of high BP compared to those in the first quartile (1.63; 1.25–2.14) (P trend < 0.001). Furthermore, we identified 40% higher prevalence of low HDL-C in quartile 2 of the LnSII compared to quartile 1 (1.40; 1.07–1.83) (P trend = 0.454). All the aforementioned associations for each component of MetS were identified after further adjustment for the other components (Model 4). The RCS curve based on the multivariable models (Model 3) did not reveal any non-linear associations between the LnSII and the components of MetS (P for non-linearity > 0.05 for all components).
Table 3 Association between systemic immune-inflammation and components of metabolic syndrome in whole population: MESA cohort (2010–2012)Subgroup analysesThe results of the subgroup analysis revealed a significant positive correlation between LnSII and MetS (Fig. 3) in specific subgroups, including men, individuals aged ≥ 60 years, Black individuals, and those who were obese. Regarding MetS components (Supplementary Table 1), a positive relationship between LnSII and high BP was found in various subgroups, including both men and women, individuals under 60 and over 60 years, as well as White and Black individuals, and in both obese and non-obese groups (P < 0.05). However, the interaction test indicated that these subgroups did not significantly modify the association between LnSII and MetS, high FBG, and elevated BP (all P for interaction > 0.05). Regarding the other components of MetS, obesity status significantly influenced the association between LnSII and elevated WC. Specifically, in obese individuals, LnSII was positively associated with higher prevalence of elevated WC (1.72: 1.00-2.95), whereas a negative association was observed in non-obese individuals (0.80: 0.66–0.97) (P for interaction = 0.009) (Supplementary Table 1).
DiscussionIn this study, we identified a significant linear relationship between SII and MetS, as well as its components, including elevated FBG and high BP, even after controlling for relevant confounding variables. These findings were consistent when analyzing SII in categorical scale. In subgroup analysis, obesity status acted as an effect modifier in the relationship between SII and elevated WC, revealing the positive association in obese individuals, whereas a negative association was observed in non-obese individuals.
SII is a well-recognized index for predicting cancer treatment efficacy and prognosis in various malignancies, including gastric, cervical, and breast cancers [34]. Previous studies have also demonstrated its predictive value in the context of other metabolism-related diseases, such as CVD [21], obesity [35], hyperlipidemia [23], hypertension [36], and diabetes [25].
Recently, a growing number of studies have focused on the significance of hematological parameters in diagnosing and preventing metabolic conditions such as MetS. For instance, it has been shown that LC [37], PC [38], and NC [39], were significantly higher in individuals with MetS compared to those without MetS, as demonstrated in our study. Some studies have also investigated the ratios of various types of blood cells in relation to MetS and have reported inconsistent findings [40]. Results from previous studies generally indicate that hematological parameters, whether assessed individually or in combination as ratios, can serve as useful predictors for MetS. However, the SII provides a more comprehensive assessment of the inflammatory state [18] by incorporating the balance between pro-inflammatory (neutrophils) [41] and anti-inflammatory (lymphocytes) responses [42], along with the role of platelets in inflammation and thrombosis [43].
Conditions such as MetS, characterized by chronic inflammation [9] and insulin resistance [44], may benefit from the inclusion of SII in risk assessment and management strategies. Two recent studies have underscored the predictive role of the SII as an inflammatory marker in relation to MetS in the general adult population. Zhao et al. [28], analyzed data from the NHANES (2011–2016) and found a non-linear association between elevated SII scores and MetS. In contrast, a study by Zeng et al. [27], using NHANES data (2015–2018), identified a linear association between SII scores and MetS. Notably, both studies were conducted in the U.S. population, focused on adults aged ≥ 20 years, and utilized NHANES data [27, 28], yet they reported differing results. The inconsistent findings regarding the shape and nature of the association between the SII and MetS and its components from two previous studies underscore the complexity of this association and highlight the need for further research to clarify these relationships.
In this study, we also observed a linear association between the LnSII and MetS. The significant positive relation between the SII and MetS, observed in our study as well as previous studies, suggests that SII plays a key role in the diagnosis of MetS across different age groups. Importantly, our findings extended prior research by demonstrating that this significant relationship may also apply to older populations, who are at higher risk for cardiometabolic disorders.
Regarding the components of MetS, our study further identified a significant linear association between the SII and elevated FBG, both on continuous and categorical scale of SII, even after adjusting for other components. This finding contrasts with two existing studies [27, 28] where the association between SII and elevated FBG disappeared upon adjusting for multiple confounders. This discrepancy may be attributed to differences in the characteristics of the study populations, such as age, prevalence of hyperglycemia, and baseline SII levels. In our study, the mean age was 69 years compared to 47 years in the two previous studies [27, 28]. Older adults are more likely to have higher levels of inflammation and a greater prevalence of MetS components. For instance, the prevalence of MetS was 36% and 27% in two previous studies [27, 28], compared to 39.2% in our study. Additionally, the mean SII was 448.8 and 242.5 in two previous studies [27, 28], compared to 513.0 in our study. Moreover, the prevalence of elevated FBG in our study was approximately 41%, compared to 26% and 30% in two previous studies [27, 28]. To our knowledge, no other studies have investigated the association between SII and hyperglycemia. However, a study utilizing data from the NHANES (2017–2020), which analyzed 7877 participants over the age of 20, indicated a positive association between SII and diabetes (1.04; 1.02–1.06) after adjusting for multiple confounders [25].
The association between inflammation, as indicated by elevated SII, and high FBG involves a complex interplay of multiple biological mechanisms. Chronic inflammation triggers the release of pro-inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) from immune cells, including macrophages and adipocytes. These cytokines disrupt insulin signaling pathways by inducing serine phosphorylation of insulin receptor substrates (IRS), leading to insulin resistance [45]. Insulin resistance impairs glucose uptake in peripheral tissues, such as skeletal muscle and adipose tissue, resulting in elevated FBG. Additionally, inflammation promotes hepatic insulin resistance, causing increased gluconeogenesis and reduced glycogen synthesis, further contributing to hyperglycemia [49]. Inflammatory mediators also activate stress-sensitive signaling pathways, such as nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and c-Jun N-terminal kinase (JNK), which exacerbate insulin resistance and impair pancreatic β-cell function [50].
We further identified a positive association between the SII and high BP, which aligns with findings from two previous studies in this field [27, 28]. However, the shape of this association was linear in both Zhao et al. [28] and our study, while it was found to be non-linear J-shaped in Zeng et al. [27] study. Research on the association between the SII and hypertension is increasingly common. A recent cross-sectional analysis of 13,742 adults from the NHANES (2017–2020) study noted a U-shaped relationship between SII and hypertension risk in American adults, with a threshold point at SII = 501.2 [36]. Additionally, another study utilizing a larger population from NHANES (1999–2018), which included 44,070 participants aged ≥ 20 years, also found a U-shaped association between the SII and hypertension, with an inflection point at SII = 363.1 [51]. The linear association between the SII and high BP in our study may be attributed to several age-related factors such as chronic low-grade inflammation, often referred to as “inflammaging” which contributes to increased cardiovascular risk and reduced physiological resilience in older adults [11, 12]. As individuals age, they tend to have higher baseline levels of SII due to cumulative exposure to various risk factors [12], leading to a more pronounced and continuous association between inflammation and BP. Further research is necessary to explore these dynamics comprehensively and validate these findings across diverse populations. The mechanisms linking the SII to hypertension involve several interconnected pathways influenced by inflammation. Research has shown that inflammation can lead to endothelial damage and dysfunction, resulting in increased vascular resistance and elevated BP [52]. Additionally, inflammation increases the production of ROS, which further impair endothelial function, promote vascular remodeling, and activate signaling pathways such as PKC and NF-κB. These pathways contribute to vascular inflammation and stiffness [45, 53]. Moreover, chronic inflammation contributes to insulin resistance, which is associated with increased sympathetic nervous system activity and sodium retention, both of which elevate BP [54]. A study by Araos et al. [55] has also demonstrated that neutrophils may play a role in the infiltration of immune cells into tissues, releasing chemokines and cytokines that promote pro-inflammatory states, contributing to the onset of arterial hypertension. Another mechanism is that inflammation can activate angiotensin II, a key component of the renin-angiotensin-aldosterone system (RAAS). Angiotensin II promotes vasoconstriction and sodium retention, further exacerbating hypertension. Additionally, angiotensin II enhances the expression of adhesion molecules and chemokines, facilitating the recruitment of inflammatory cells to tissues and perpetuating a cycle of inflammation that exacerbates hypertensive conditions [56].
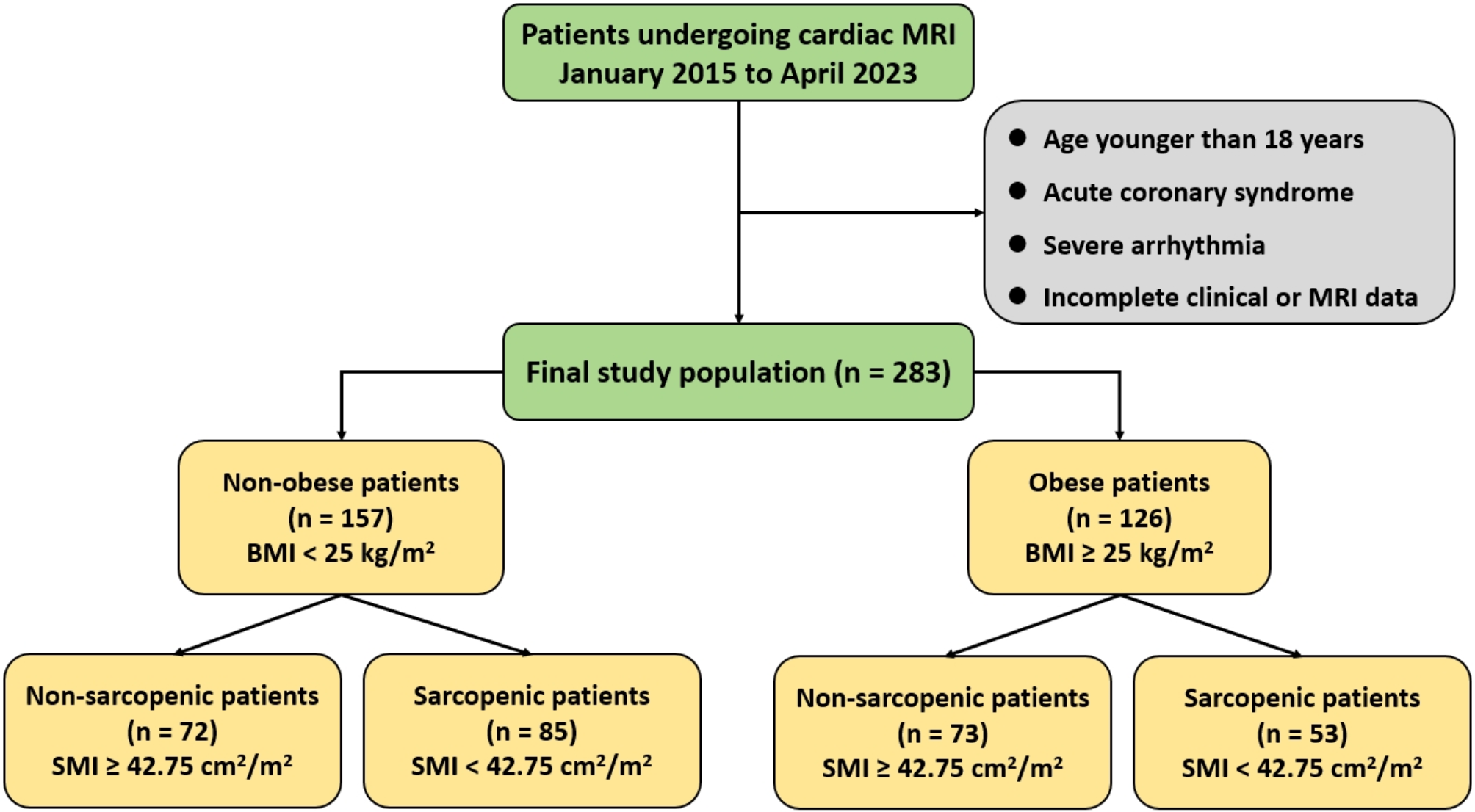
Fig. 1
Flowchart of participants included in the study, MESA cohort (2010–2012). MESA: Multi-Ethnic Study of Atherosclerosis
Fig. 2
Restricted cubic spline curve depicting the association (with 95% CI) between LnSII and MetS and its components; MESA cohort (2010–2012). The solid line represents the OR, and the gray shaded area indicates the 95% CI. The horizontal dashed line represents the null value (OR = 1), and the vertical dashed line marks the threshold of LnSII at which the OR changes direction. OR: odds ratio; 95% CI: 95% confidence interval; SII: systemic immune-inflammation; LnSII: natural logarithm-transformed SII; MetS: metabolic syndrome; HDL-C: high-density lipoprotein cholesterol; BMI: body mass index; BP: blood pressure; FBG: fasting blood glucose; TG: triglycerides; MESA: Multi-Ethnic Study of Atherosclerosis. The models were adjusted for age, sex, race, BMI, total physical activity level, family history of diabetes, alcohol consumption, education and smoking
Fig. 3
The association between systemic immune-inflammation and metabolic syndrome in subgroups based on sex, age, race, and obesity status; MESA cohort (2010–2012). The association between LnSII and MetS was estimated using logistic regression model fitted separately for each subgroup, adjusting for age, sex, race, BMI, total physical activity level, family history of diabetes, alcohol consumption, education level, and smoking status. MESA: Multi-Ethnic Study of Atherosclerosis; OR: odds ratio; CI: confidence interval; SII: systemic immune-inflammation; LnSII: natural logarithm-transformed SII; MetS: metabolic syndrome; BMI: body mass index; non-obese: BMI < 30 kg/m2; obese: BMI ≥ 30 kg/m2
In summary, the current evidence demonstrates bidirectional relationships between inflammation and Mets components. For example, while inflammation may drive metabolic dysfunction, metabolic abnormalities per se (e.g., hyperglycemia, hypertension) can also exacerbate inflammation, creating a vicious cycle [55, 56].
We did not find a significant association between the LnSII and three other components of Mets: high TG, elevated WC, and low HDL-C in total population. However, in categorical scale, we identified 40% higher prevalence of low HDL-C in quartile 2 of the LnSII compared to quartile 1 (Model 4). We did not observe a significant association between the SII and elevated WC or TG. However, two previous studies reported a significant positive correlation between SII and high WC [28] as well as high TG [27]. The discrepancy between our findings and those of the mentioned studies could be attributed to the differences in adjustment methods. In our analysis, we further adjusted for the other components of MetS to examine the independent relationship between SII and specific MetS components, free from the influence of the other remaining components. This adjustment is crucial, as MetS components are often interrelated. In contrast, the previous studies [27, 28] did not account for these interrelationships. Without such adjustments, the association observed between a specific MetS component and SII may be confounded by the presence of other interrelated components. For instance, insulin resistance can contribute to both hypertension and dyslipidemia [57]. When assessing the relationship between SII and elevated TG, this association may be influenced by the presence of high BP, or insulin resistance. Failure to adjust for these components could obscure the true association between SII and elevated TG.
The independence associations of the SII with MetS components, particularly high FBG and high BP, free from other components of MetS in our study, highlight the potential of SII as a comprehensive marker for metabolic disturbances and underscores its relevance in understanding glucose and BP regulation within the context of MetS. This finding suggests that monitoring SII levels may help identify individuals at risk for hyperglycemia and hypertension, even before the full manifestation of MetS.
Subgroup analysis in this study revealed a positive relationship between SII and high WC in obese individuals, while a negative association was observed in non-obese participants. The contrasting associations between SII and elevated WC in obese versus non-obese participants could be attributed to differences in body composition, as obese individuals typically have a higher proportion of visceral fat associated with increased inflammation [58], leading to a stronger positive correlation between SII and elevated WC. Additionally, non-obese individuals may exhibit a healthier metabolic profile, where inflammation does not translate to increased abdominal fat. Further investigation using longitudinal studies is necessary to elucidate the underlying mechanisms.
The strengths of our study lie in its utilization of the MESA data, which provides a large, diverse, and well-characterized cohort with detailed information on cardiovascular and metabolic risk factors. Additionally, our study addresses a critical gap in the literature by focusing on middle-aged and older adults, a population at heightened risk for cardiometabolic disorders. This focus contributes valuable insights to the field and enhances the relevance of our findings for public health strategies aimed at improving metabolic health in this vulnerable demographic. Furthermore, in our investigation of the association between SII and each MetS component, we made additional adjustments for other components that were not considered in previous studies [27, 28]. Finally, we achieved a statistical power of over 99% to detect a significant OR of at least 1.20 for MetS and its components, including elevated FPG and high BP, per one-unit increase in lnSII. This robust statistical power enhances the reliability of our findings and underscores the validity of the observed associations.
However, it is important to acknowledge the limitations of our study. First, the cross-sectional design restricts our ability to draw causal inferences regarding the examined associations. Second, there may be unmeasured confounding factors, such as dietary intake or lifestyle variables, that could influence the results. Third, our study was conducted within a U.S. population with participants aged over 45 years. This focus on a specific demographic may limit the applicability of our findings to younger populations.
留言 (0)