
記住我
This randomized, single-blind, controlled trial was approved by Ethics Committee of Alborz University of Medical Sciences (Approval ID: IR.ABZUMS.REC.1401.084). The trial adhered to the CONSORT guidelines. All individuals gave written consent prior to study participation.
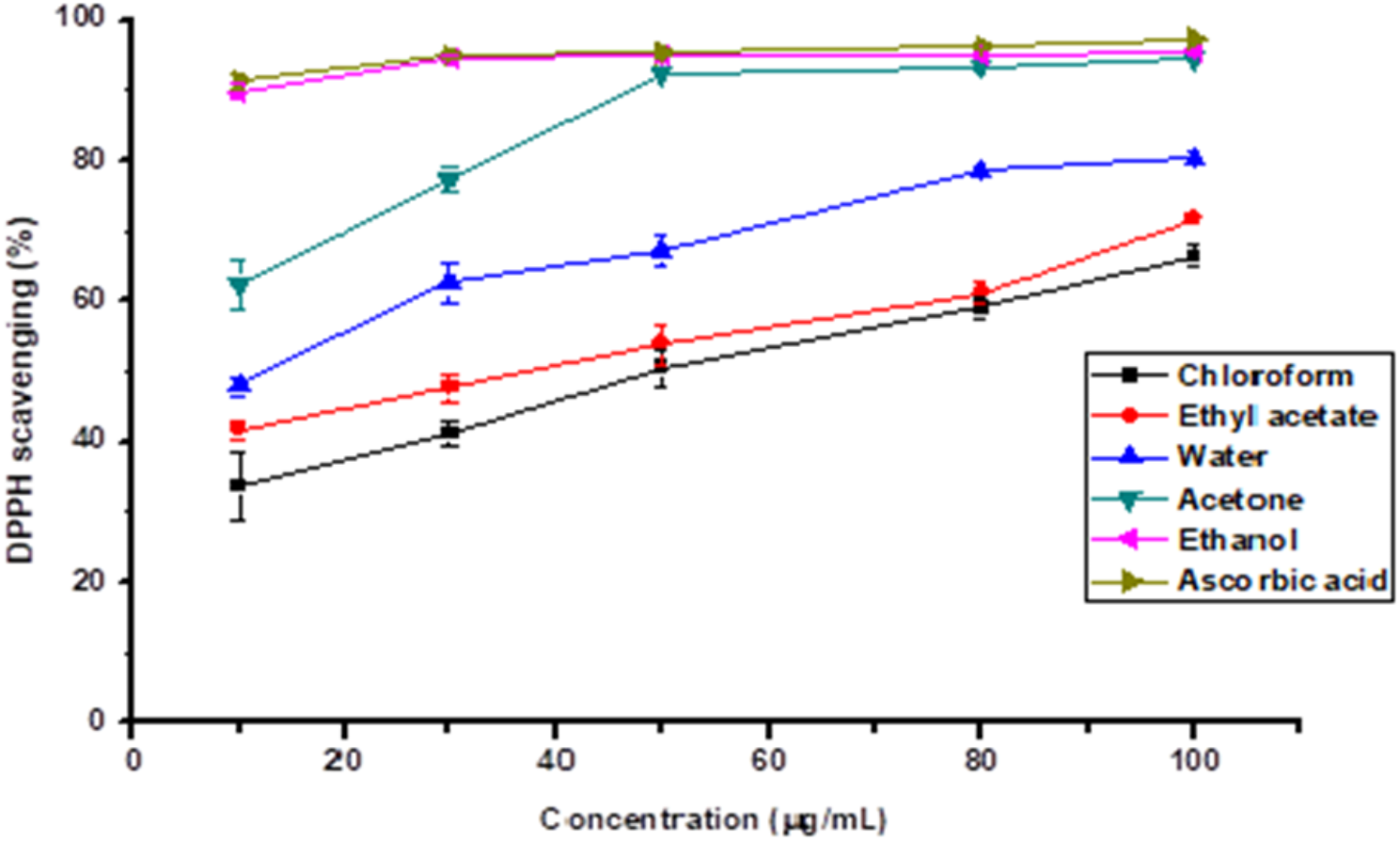
Participants and randomizationThe research population consisted of children hospitalized in Imam Ali Hospital of Karaj in Alborz Province, Iran. The inclusion criteria involved children aged 3 to 10 years, being admitted to the ward for at least 48 h, staying in the hospital for at least 5 days, and obtaining informed consent from the child’s parents. The exclusion criteria included having cognitive, neurological, and learning problems, child unconsciousness, and inability to participate in the interventions [22]. The required sample size with a confidence factor of 95% (5% error rate) and a test power of 95% was 25 for each group, using the sample size formula and the study of Davidson et al. [23]. After obtaining consent from the parents and ensuring the confidentiality of their information, 75 childrenTotally, 75 children were included (n = 25 for each group) meeting the inclusion criteria were selected from among those referring pediatric ward of Imam Ali Hospital of Karaj, Iran from 2022 to 2023 until reaching the required sample size using the limited randomization method according to the random allocation rule. The CONSORT flowchart is illustrated in Fig. 1. For this purpose, a random sequence was generated based on three groups using Random Allocation Software 2.0, and then the participants were assigned to three groups: storytelling group (A), play therapy group (B), and control group (C).
See Fig. 1 for an overview of the screening and recruitment process.
Fig. 1
To prevent bias in the selection and assignment of participants, a limited randomization method was used. First, a random sequence was generated based on three groups ([A], [B], and [C]) using Random Allocation Software 2.0. This process ensured that participants were randomly assigned to each of the three groups according to the random allocation rule, reducing selection bias. In addition, the allocation was concealed, meaning that the person assigning participants to groups was unaware of the group allocations at the time of assignment, further reducing the risk of bias. Moreover, both the participants and the research team conducting the interventions were blinded to group assignments (single-blind design) to minimize performance and detection bias. To ensure that the sample was representative and that randomization was properly implemented, the process was continuously monitored by an independent researcher who was not involved in the interventions.
Intervention procedureDemographic profile questionnaireInitially, a demographic profile questionnaire was used to collect the children’s personal information based on parents’ responses to the questions at the first day. Additionally, other questionnaires were completed by each participant before the interventions began. In other words, the data collected on the first day correspond to the period prior to the start of the interventions. Parents were allowed to stay with their children during the procedures, ensuring the children felt secure in a familiar presence.
Control groupIn the control group, the usual ward procedures were carried out. These included monitoring vital signs, administering injections, and providing drug therapy as prescribed by the attending physician. No additional therapeutic interventions were implemented in this group.
Play therapy interventionIn the play therapy group, children participated in therapeutic play sessions using toy medical kits to engage in patient-doctor role play. Additionally, medical equipment available in the hospital, such as microsets, cotton, needleless syringes, and abselang, were used to create craft activities. Play therapy was conducted individually for each child, under the supervision of the researcher. The intervention lasted for 30 min each day for 2 consecutive days. The goal of this intervention was to reduce anxiety and help children process their medical experiences through play.
Storytelling interventionIn the storytelling group, two books were used to address the children’s hospital experience:
On the first day, the book “Should I Go to the Hospital?” by Pat Thomas, translated by Dr. Geeta Mullally, was read to the children.
On the second day, the book “Franklin Goes to the Hospital” by Paulette Bourgeois, translated by Shohreh Hashemi, was read by either the child’s parents or one of the researchers.
The goal of the storytelling intervention was to familiarize children with the hospital environment and reduce anxiety through narrative and familiarization with hospital procedures.
Anxiety measurementAfter the interventions, children’s anxiety levels were assessed using two anxiety scales:
A blinded researcher collected the data from the children to measure their anxiety levels. In the groups, anxiety was measured daily using the Spence Children’s Anxiety Scale. For children aged 3–4 years, parents were asked to respond to the SCAS questions based on their observations of the child’s behavior. For children aged 5–10 years, the SCAS was administered directly to the children, with any clarifications provided if needed. Notably, children’s anxiety was measured over three consecutive days.
MesurementsThe data collection tool included a demographic questionnaire, including child age and gender, the number of children, the number of pregnancies, the use of assisted reproductive technology, what number the hospitalized child is for the mother’s child? and the shadow of hospitalization. We used two anxiety scales as complementary: (1) general measures of anxiety and severity of anxiety (2) administered by self-report.The Spence Children’s Anxiety Scale (1997) was designed to assess the anxiety of children [24], consisting of 45 questions and six domains and measuring children’s anxiety based on a four-point Likert scale (never: 0, sometimes: 1, often: 2, always: 3). The six investigation domains include separation anxiety, social anxiety, obsessive-compulsive disorder, panic-agoraphobia, generalized anxiety, and post-traumatic stress disorder. A 0–44 score indicates a low level of children’s anxiety, 44–88 a medium level of anxiety, and above 88 a high level of anxiety. Cronbach’s alpha in Zargami’s research et al. for this questionnaire was estimated above 0.7 (0.86) [25]. The Visual Facial Anxiety Scale was invented in 1990 by Piyeri. According to the images below (Fig. 2), the Visual Facial Anxiety Scale for anxiety assessment includes seven facial expressions with a number under each, which makes a numerical scale of 0 to 6. Face 1 has a neutral expression, but faces 2–7, respectively, show the increase in anxiety. This tool is shown to the child to measure anxiety; he is asked to report his anxiety corresponding to one of the faces [26].
Fig. 2
Five-face scale for assessing distress in children modified smiley faces scale. Aadpted from [16]
Analysis methodThe Mixed effect model statistical method was used to analyze the data. Assuming the data structure and baseline time control, the random intercept effect was used in this model so that possible heterogeneity was also controlled with this method. Also, due to the non-normal distribution of the data, this model was fitted to the data based on the inverse Gaussian distribution. Since the response scale for 3-8-year-old children was different from 8-10-year-old children, first the data was normalized and then the desired model was fitted to the data to homogenize the scale and involve all children in the study and accurately compare the results. To achieve the most accurate results in this model, the effect of some variables was controlled, listed in Table 1. Finally, SPSS 22 was used for data analysis; the significance level was set at 0.05.
Table 1 Description of children’s anxiety in different times and treatment groupsTiral registrationThe study registered at the Iranian Registry of Clinical Trials (Code: IRCT20220704055367N1) as of July 13, 2022; it is avalible at the website: https://irct.behdasht.gov.ir/.
留言 (0)