Study population
We obtained data from the NHANES, a population-based survey to assess the nutritional and health status of the non-institutionalized United States civilization. The survey was conducted in two-year cycles using a complex stratified, multistage probability design. Using sampling weights, we obtained a nationally representative sample across the U.S.. Methodological details of the NHANES are available at www.cdc.gov/nchs/nhanes/. The Ethics Review Board of the National Center for Health Statistics (NCHS) granted approval for the survey protocol. Written informed consent form was obtained from all participants.
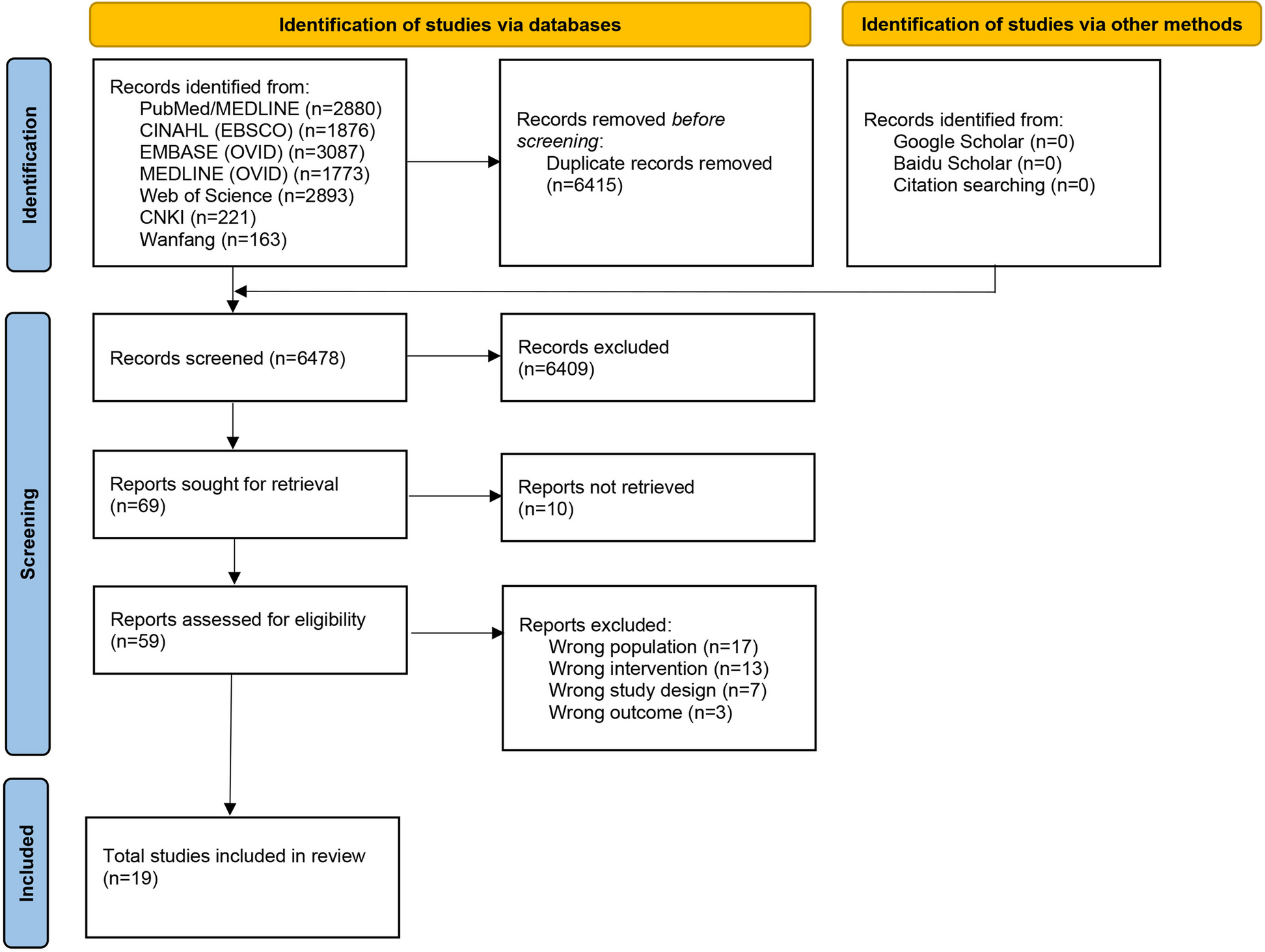
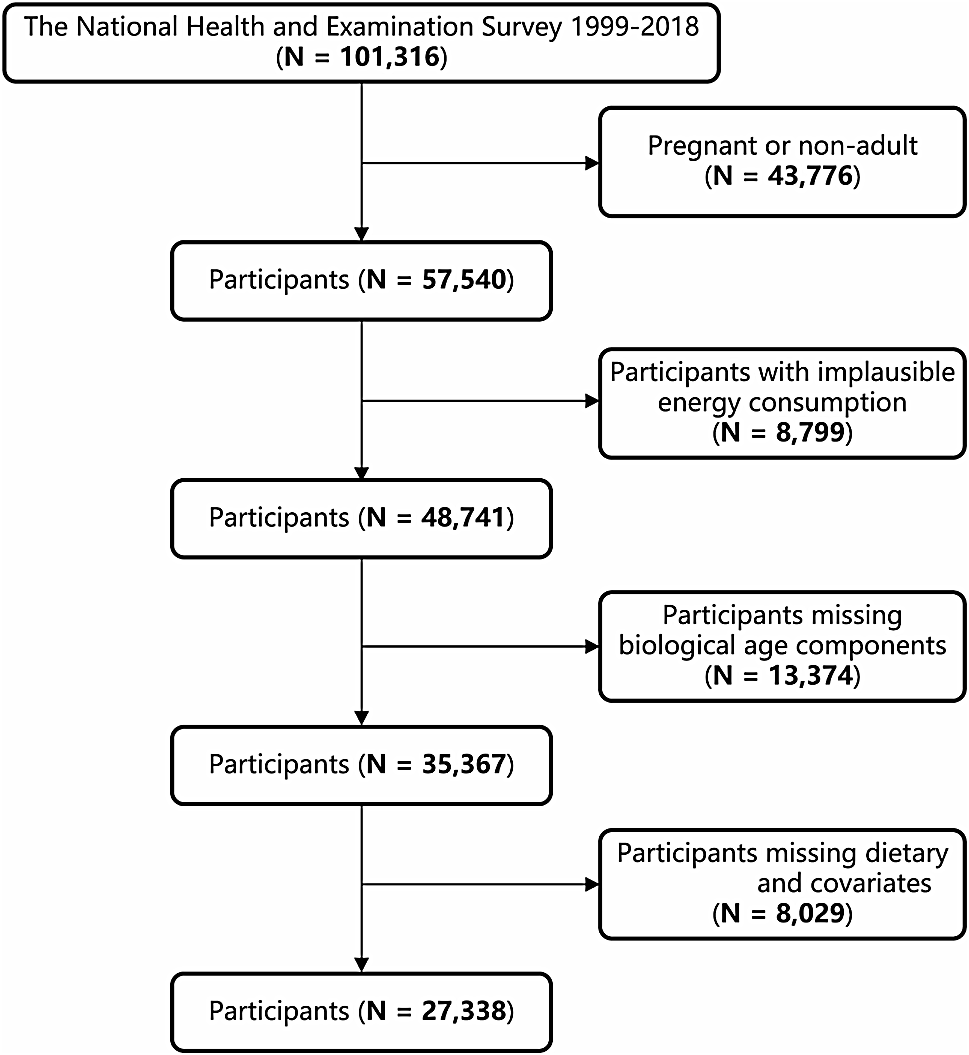
The present study utilized data from ten consecutive NHANES survey cycles (1999–2018). The exclusion criteria were as follows: (1) age < 18 years, (2) pregnant individuals, (3) participants without survival status (4) participants without dietary information, and (5) participants without hypertension. After exclusion, a total of 16,190 participants with hypertension remained for the final analysis (Fig. S1).
Definition of hypertension
Hypertension was defined as self-reported diagnosis by a physician, taking prescribed antihypertensive medications, or presenting with mean SBP ≥ 140 mmHg, or mean DBP ≥ 90 mmHg. In sensitivity analyses, the cut-off value of BP was set as mean SBP ≥ 130 mmHg, or mean DBP ≥ 80 mmHg according to the guidelines of American College of Cardiology/American Heart Association [7].
Collection of dietary information
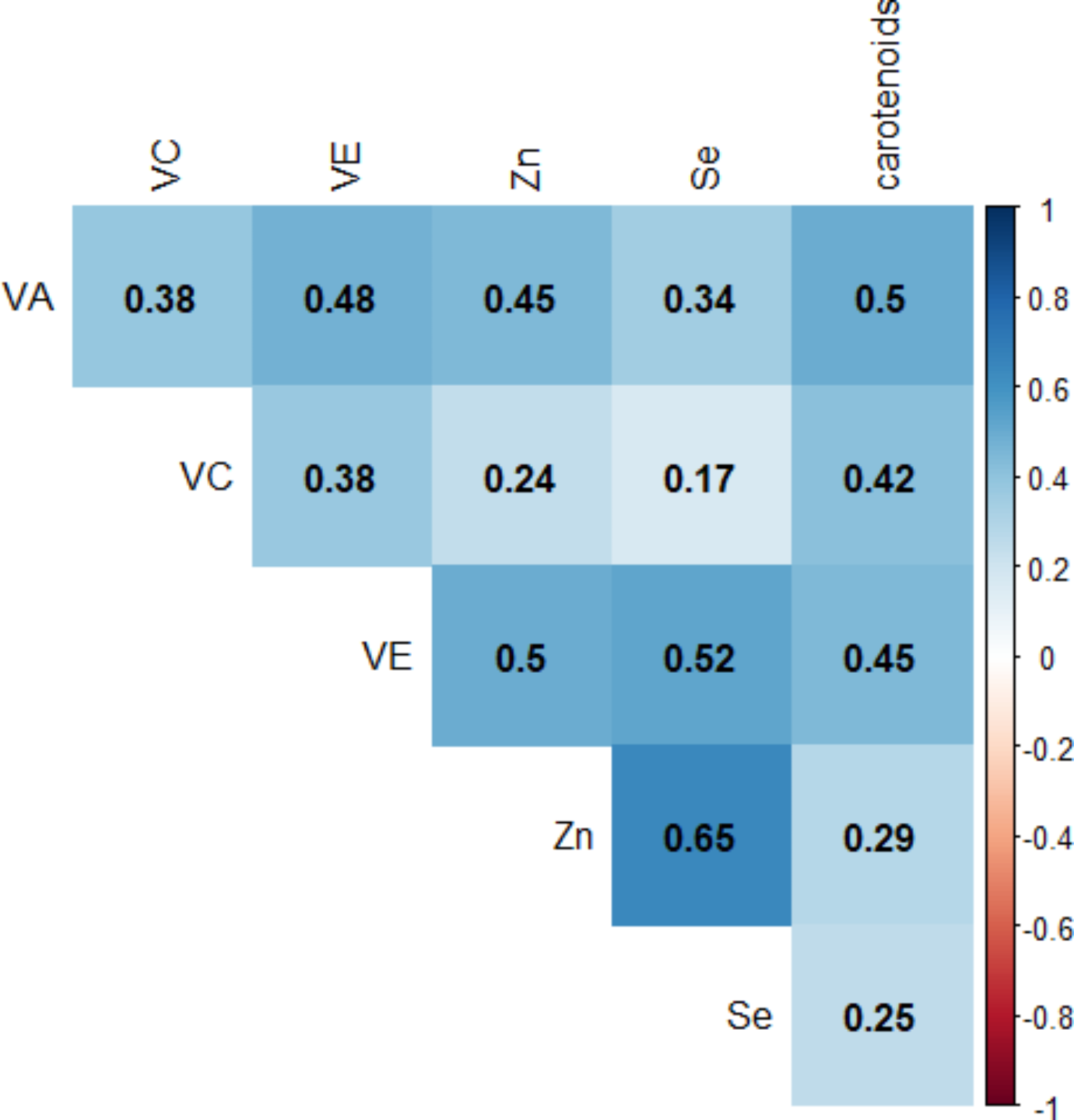
Total nutrient intakes were obtained from two separate 24-hour dietary recalls, which included the types and amounts of foods and beverages consumed during the 24-hour period prior to the interview. The first recall was collected by an in-person interview in the mobile examination center (MEC), and the second recall was scheduled 3–10 days later by telephone. The mean intake of two dietary recalls was used in our analysis. Six antioxidants were concerned in our study, including vitamin A, vitamin C, vitamin E, zinc, selenium, and total carotenoids. The assessment of dietary antioxidants did not encompass antioxidants derived from dietary supplements, medication, or drinking water. The joint effect of dietary intake was evaluated with CDAI developed by Wright et al. [15, 16]. Briefly, the CDAI was calculated as the sum of the normalized intakes of the six antioxidants. Normalization was performed by subtracting the mean of the intake of each antioxidant and divided by the standard deviation.
Assessment of the outcome
Death outcomes were ascertained by linkage to National Death Index records through December 31, 2019. Follow-up time was defined as the period from the date of interview on MEC to the date of death or to the end of follow-up. CVD death was defined as ICD-10 codes I00-I09, I11, I13, and I20-I51.
Covariates
Covariates include age, sex (male or female), race (non-Hispanic white, non-Hispanic black, or others), educational level (less than high school or high school and above high school), body mass index (BMI), smoking history (current, former, or never), total energy intake (kcal), type 2 diabetes (T2D, yes or no), cardiovascular disease (CVD, yes or no), and chronic kidney disease (CKD, yes or no).
BMI was calculated as the ratio of body weight (kg) to the square of height (m) and expressed as kg/m2. T2D was diagnosed with the following criteria: fasting glucose ≥ 7 mmol/L, random glucose ≥ 11.1 mmol/L, glycated hemoglobin A1c ≥ 6.5%, the usage of hypoglycemic drugs, or a history of diabetes. CVD was recognized by a self-reported physician’s diagnosis of congestive heart failure, coronary heart disease, angina, heart attack, or stroke. The estimated glomerular filtration rate (eGFR) was calculated based on the Chronic Kidney Disease Epidemiology Collaboration creatinine equation [17]. CKD was determined by eGFR < 90 ml/min/1.73m2 or albuminuria > 30 mg/g [18].
Statistical analysis
All analyses incorporated proper sample weights, and the weighted statistical analyses were conducted with R package “survey” conforming to NHANES analytic guidelines to produce national-representative estimates. Continuous variables were analyzed with Mann-Whitney U test and presented as medians (interquartile ranges). Categorical variables were analyzed with χ2 test and presented as frequencies. Correlation between pairwise antioxidants was assessed using Spearman correlation coefficients. Missing rates for all covariates were < 5%, and missing data were imputed using the random forest algorithm with the R package “missForest”.
We conducted weighted multivariable cox proportional hazards regressions to estimate the risk of antioxidants for all-cause and CVD mortality. Model 1 was unadjusted, whereas Model 2 was adjusted for age, sex, and race. Model 3 was further adjusted for educational level, BMI, smoking status, total energy intake, T2D, CVD, and CKD. The results were expressed as hazards ratios (HRs) with 95% confidence intervals (95% CIs). To explore the potential non-linear relationship, we plotted 4-knots (5th, 35th, 65th, and 95th percentiles) weighted restricted cubic spline (RCS) based on the fully adjusted model. The nonlinearity was tested using the likelihood ratio test. The Kaplan–Meier method was used to construct the survival curves among patients with different CDAI quartiles, and the differences of survival probability were evaluated with log-rank test.
Subgroup analyses were stratified by age (< 60 or ≥ 60 years), sex (male or female), BMI (< 25, 25–30, or ≥ 30 kg/m2), T2D (yes or no), CVD (yes or no), and CKD (yes or no). The interaction effects between CDAI and those variables were evaluated.
Several sensitivity analyses were also performed to test the robustness of our study. First, patients who died within the first two years of follow-up were excluded to reduce inverse casualty. Second, we further enrolled participants with mean SBP ≥ 130mmHg or mean DBP ≥ 80mmHg [19]. Third, we further adjusted for the supplementary consumption of antioxidants. Fourth, we further adjusted for the medication use. Lastly, we repeated the main analyses after excluding patients with missing covariates.
Additionally, we conducted WQS regression with R package “gWQS”. WQS is a novel method used in estimating the joint and independent effects of mixed exposure [20]. The data were randomly split into training sets (40%) and validation sets (60%), and the training set was bootstrapped 400 times. The overall effect of six antioxidants and weight of each component (represents the contribution of certain exposure to all-cause mortality) were calculated. Weights of all antioxidants constrained to sum to 1 and the exposure with weight over 0.17 was considered to be the major contributor of the association between antioxidants and all-cause mortality. The covariates adjusted in WQS were the same as the fully adjusted cox regression model. A two-sided p < 0.05 was considered as statistically significant. All analyses were performed with R (version 4.1.0).


留言 (0)