
記住我




In this observational study, a cohort of MASLD outpatients, subsequently divided into mild-advanced hepatic fibrosis (≤ F3 fibrosis) and ACLD based on Liver Stiffness Measurement (LSM), as well as in MASLD-related cACLD [naïve for the onset of previous liver-related decompensation events (LRDEs) and MASLD-dACLD [defined by ongoing LRDEs or LRDEs occurrence in the last 12 months, without gaining recompensation [11, 12]] individuals, were consecutively enrolled.
As detailed below, at the enrollment, clinical-anthropometric data, biochemical variables, and nutritional parameters were collected, as well as the presence/absence of dysgeusia was assessed. During a six-month follow-up period, for dACLD patients, the onset of new LRDEs was recorded.
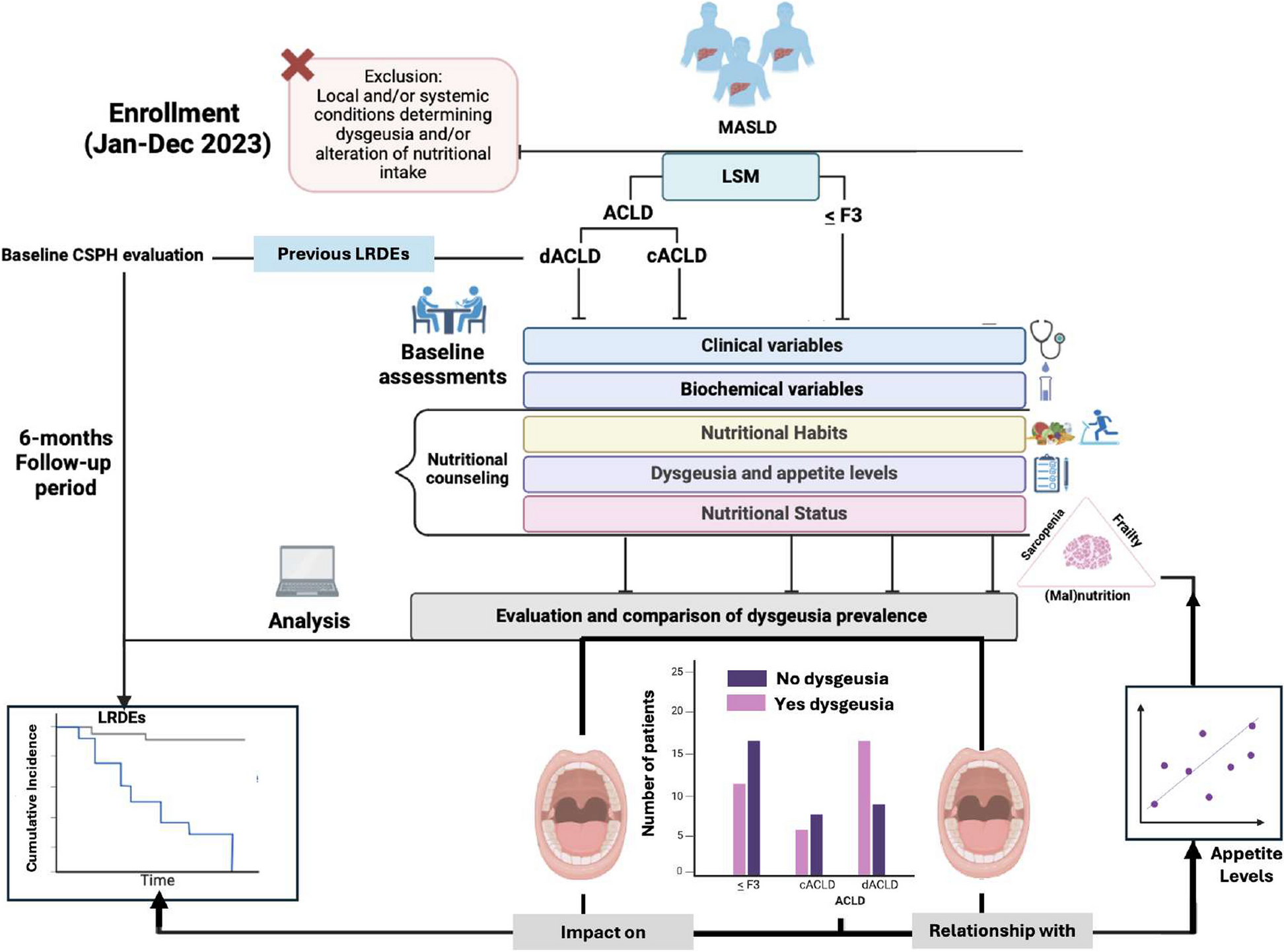
The prevalence of dysgeusia in dACLD patients compared with cACLD and ≤ F3 fibrosis ones represented the primary endpoint of this study. To investigate the relationship of dysgeusia with appetite levels and, indirectly, with the nutritional status in ACLD (cACLD and dACLD) patients, as well as the relative impact on the onset of further LRDEs in dACLD individuals, constituted the secondary endpoint. The experimental design is reported in Fig. 1.
Fig. 1
Experimental flow-chart. LSM was adopted to discriminate ≤ F3 patients and ACLD individuals, whereas the evaluation of LRDEs’ occurrence (ongoing and in the previous 12 months) distinguished cACLD and dACLD patients. In particular, LRDEs were: (a) progressive jaundice in not-cholestatic disease, (b) ascites, (c) HE, (d) variceal bleeding, or (e) any acute bacterial infections. The evidence of esophageal varices defined CSPH. Anthropometric parameters included Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Body Mass Index (BMI), and Waist-hip ratio (Whr) determination. Biochemical variables included platelet count (PLT), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TB), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), Fasting Plasma Glucose (FPG), total cholesterol, High-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides (TG), serum albumin (SA), International-Normalized Ratio (INR), and creatinine. For ACLD, the Child-Pugh-Turcotte score was determined. Nutritional counseling was offered to all the patients: for this purpose, dietary and physical exercise habits were assessed, as well as the presence of dysgeusia (see the main text) and appetite levels. Nutritional status, including the evaluation for sarcopenia and frailty, was opportunely defined by using bioelectrical impedance analysis (BIA) and Liver Frailty Index (LFI) calculation. During a 6-month follow-up period, further LRDEs were recorded for dACLD. At the baseline, as well as during the follow-up, LRDEs considered were (a) progressive jaundice in not-cholestatic disease, (b) ascites, (c) HE, (d) variceal bleeding, or (e) any acute bacterial infections. Jan: January; Dec: December; MASLD: Metabolic dysfunction-associated Steatotic Liver Disease; LSM: Liver stiffness measurement; ACLD: advanced chronic liver disease; cACLD: compensated advanced chronic liver disease; dACLD: decompensated advanced chronic liver disease. LRDEs: liver-related decompensation events; CSPH: Clinically Significant Portal Hypertension
PatientsThis observational longitudinal study complies with the ethical guidelines of the Declaration of Helsinki (1975) and was approved by the ethical committee of the University of Campania Luigi Vanvitelli in Naples (prot n. 0016948/i-2023). The enrollment was carried out at the Hepato-Gastroenterology Division of the University of Campania Luigi Vanvitelli between January and December 2023.
Inclusion criteria were age over 18 years and a proven clinical history of MASLD diagnosed following the relatively updated multi-society Delphi consensus proposed criteria [13].
Exclusion criteria were: (a) chronic liver disorders otherwise than MASLD [CHB, CHC, and alcohol-related liver disorder (ALD), autoimmune hepatitis, chronic cholestasis]; (b) smoke and alcohol abuse history; (c) decompensated type 2 diabetes mellitus (T2DM); (d) severe gastroesophageal reflux disease (GERD); (e) cancer/leukemia/lymphoma diagnosis; (f) pregnancy; (g) psychological/psychiatric problems that could have invalidated the informed consent and/or could have determined taste alterations; (h) acute or chronic kidney diseases with glomerular filtration rate (GFR) < 30 mL/min; (i) previous Sars-CoV-2 infection causing taste alterations from long-Sars-CoV-2 infection or ongoing infection; (j) oral cavity neoplasia; glossitis/stomatitis, including those caused by iatrogenic radiation treatments of the head and neck region; (k) Sjögren's syndrome, rheumatoid arthritis, lupus erythematosus, psoriasis and other autoimmune diseases including thyroid diseases; (l) use of drugs for which taste disorders are reported among adverse drug reactions (ADRs), as well as zinc and vitamin A supplementation in the previous 6 months; (m) presence of eating disorders; (n) neuropathies as injury to the trigeminal and glossopharyngeal nerve, facial paralysis, brainstem tumors, head trauma, stroke, neuromas of the cerebellopontine angle, diabetic neuropathies, and multiple sclerosis. Alcohol consumption was evaluated by using the Alcohol Use Disorders Identification Test (AUDIT-C) questionnaire [14].
At the enrollment, Transient Elastography (TE) was adopted to determine LSM: according to the Baveno VII consensus, LSM values ≥ 15 kilopascals (kPa) discriminate ≤ F3 and ACLD [11]. Adhering to the clinical practice guidelines (CPGs), for ACLD patients, the evidence of ongoing LRDEs or the occurrence of LRDEs in the 12 months preceding the enrollment, without gaining recompensation [11, 12], identified dACLD. In detail, LRDEs were: (a) progressive jaundice in not-cholestatic disease, (b) ascites, (c) HE, (d) variceal bleeding, or (e) any acute bacterial infections [15].
At baseline, for each patient, anthropometrical evaluations included Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP) (mmHg) measurements, as well as Body Mass Index (BMI) calculation by dividing the weight (kg) by the square of height (m), and the waist-to-hip ratio (WHR) determination. In dACLD patients with ongoing severe ascites, BMI and WHR were obtained after Large Volume Paracentesis (LVP). SBP ≥ 130 with DBP ≥ 85 mmHg configured arterial hypertension, and a BMI > 30 identified obesity [13].
The biochemical variables included: platelet count (PLT) (count/mm3), aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP) (U/l), total bilirubin (TB), Fasting Plasma Glucose (FPG), total cholesterol, High-density lipoprotein (HDL), Low-density lipoprotein (LDL), triglycerides (TG), creatinine (mg/dl), serum albumin (SA) (g/dl), and International-Normalized Ratio (INR). For ACLD patients, the Child–Pugh (CP) score was determined [16].
For all patients, we investigated pharmacological history [including the administration of recognized “disease-modifying drugs”: non-selective beta-blockers (NSBBs) and human albumin [17, 18]], as well as the presence of MASLD-related comorbidities (obesity, arterial hypertension, dyslipidemia, T2DM) [13]. The evidence of esophageal varices configured clinically significant portal hypertension (CSPH) [11].
Furthermore, specialized nutritional counseling evaluating dietary habits, physical exercise, and body composition was offered to all enrolled subjects. On this occasion, sarcopenia, frailty, dysgeusia, and appetite levels were also opportunely investigated. Finally, dACLD patients were followed for 6 months, and the onset of new LRDEs, opportunely recording those requiring hospitalization, was registered.
Liver stiffness measurementLSM was performed using FibroScan® [version 502 (Echosens, Paris, France)] with M and XL probes [19]. We used the XL probe when the ultrasound-measured distance between the skin and the liver capsule was greater than 2.5 cm and/or when the patient's BMI was > 30. FibroScan® was performed by an expert physician obtaining 10 acceptable measurements, with the maximum number of attempts set at 20. The criteria proposed by Boursier et al. defined measurement as “very reliable” (IQR/M ≤ 0.1), “reliable” (0.1 < IQR/M ≤ 0:3 or IQR/M > 0.3 with LS median < 7.1 kPa), or “poorly reliable” (IQR/M > 0.3 with LS median ≥ 7.1 kPa [19, 20].
Nutritional assessmentEvaluation of physical exercise and dietary habitsThe validated “International Physical Activity Questionnaire Short Form” (IPAQ-SF) was adopted to simultaneously assess the time spent on moderate physical exercise and sitting periods [21] (Supplementary File 1).
To assess dietary habits, individuals reported daily meal intake (types of food and quantity) in a dedicated electronic diary. The Winfood Software 2.0 package (Medimatica s.r.l., Martinsicuro, Italy) analyzed and processed the collected data. Based on the quantity and quality of foods consumed, the software analysis evaluated the percentage of macronutrients and micronutrients in each food, the grams per body weight (g/kg) daily assumed, and the energy intake (kcal/die) relative to a complete week (including weekends). According to the European Society for Clinical Nutrition and Metabolism (ESPEN) CPGs on the topic, the following cut-offs for malnutrition and muscle depletion in cirrhotic patients were adopted to oral diet-derived intake: a) total energy intake: ≥ 35 kcal/kg/die; b) protein intake ≥ 1.5 g/kg/die [22].
Body composition assessmentA multifrequency bioelectrical impedance analysis (BIA) system (BIA MC-980A, Tokyo, Japan) was used to perform the body composition assessment and simultaneously determine multicompartment body composition parameters. The BIA system, thanks to a series of types of machinery algorithms elaborated the Free Fat Mass (FFM), the Fat Mass (FM), the body cell mass (BCM), the extracellular cell mass (ECM), expressed both in percentage and kilograms (Kg), as well as the total body water (TBW) and Skeletal Muscle Mass (SM) (Kg).
SMM-Index (SMMI) was calculated by dividing the SMM by the square of the height (m2) [23], whereas the impedance index was determined by dividing the square of the height (m2) by R [24].
The following single sex-specific validate equations, for which a strong correlation with dual-energy X-ray absorptiometry (DXA)-determined values have been revealed [25], were adopted to estimate Appendicular SM (ASM): (a) ASM-Men = 0.197 × (impedance index) + 0.179 × (weight) −0.019; (b) ASM-Women = 0.221 × (impedance index) + 0.117 × (weight) + 0.881 [26]. Finally, ASM/h2 was obtained by dividing the ASM by the square of the height (m2) (Kg/m2).
To maximally standardize body composition measurements, the BIA was performed in the morning (constantly in the time slot between 8.00 a.m. and 9.00 a.m.), and all patients were fasting since the night before (i.e. last meal was permitted no later than midnight).
Furthermore, as well as for anthropometrics, in dACLD patients with ongoing severe ascites, all the BIA-assessed parameters were obtained after LVP.
Sarcopenia and frailty assessmentThe following parameters were considered to assess sarcopenia: (a) muscle quantity, (b) muscle strength, and (c) physical performance [27]. Respectively, (a) the ASM/h2 estimated the muscle quantity, and (b) the hand-grip (HG) test, by using the digital dynamometer SUAVER® and obtaining the average of 3 consecutive measurements (Kg) for each patient, as well as the chair-stand test (measuring the times in seconds, considering 5 repetitions, required to get up from the chair) defined the muscle strength. Furtherly, (c) the timed-up and go (TUG) test (measuring the time in seconds required to get up from a chair, walk three meters, turn around, return to the chair, and sit down again), the gait speed test (measuring the velocity in m/second to complete a 4 m linear course), and the Short Physical Performance Battery (SPPB) [combining the results of the chair-stand test, gait-speed test, and a balance test (BT) evaluating the time in seconds holding 3 increasing difficulty positions “side-semi tandem-tandem”, ranging from a total score of 0–12] were adopted to define physical performance [27]. An impairment of muscle strength was determined by HGT < 27 kg in males (and < 16 kg in females) and chair-stand test > 15 s, whereas an SPBB < 8, a gait speed test < 0.8 m/second, and a TUG ≥ 20 s configured a physical performance reduction. An ASM/h2 < 7 kg/m2 (males) [< 5.5 kg/m2 (females)] defined muscle quantity impairment.
According to the revised criteria proposed by the European Working Group on Sarcopenia in Older People (EWGSOP2), sarcopenia was diagnosed when muscle strength impairment was revealed, and muscle quantity impairment or physical reduction was evidenced [27].
Liver Frailty Index™ (LFI) [28], non-invasively determined the relative frailty status. The frailty status was determined by using validated cut-offs: robustness (LFI < 3.2), prefrailty (LFI between 3.2 and 4.4), and frailty (LFI ≥ 4.5) [29] (Supplementary File 2).
Evaluation of dysgeusia and dysgeusia-related appetite levelsTo assess the dysgeusia, all patients received a questionnaire composed of specific questions (items), fitting to ACLD features, opportunely extracted from the adapted Italian version of the validated CITAS questionnaire [30] (Supplementary Files 3A and 3B).
The questionnaire was composed of three sections for a total of 17 items, with a score from 1 to 5 for each question exploring taste-related features relative to the last six months. Since a dedicated visual analog scale (VAS) was separately predisposed to evaluate the appetite levels, “Item” 18, which normally assesses appetite in the original CITAS questionnaire, was herein not included.
Respecting the creator’s instructions [30], the total single score related to the 4 dimensions of TDs was calculated as follows: (1) Reduction of flavors (1st single score) = add the scores of questions from 2 to 6 and divide by 5; (2) Discomfort (2nd single score) = add the scores of questions from 13 to 17 and divide by 5; (3) Fantageusia and parageusia (3rd single score) = add the scores of questions from 10 to 12 and divide by 3; (4) General alterations in taste (4th single score) = add the score of question 1 to those of questions 7 to 9 and divide by 4 [30]. For a correct evaluation, no omissions were admitted. By adding the single scores, the “Dysgeusia Total Score” (DTS) was obtained. A Dysgeusia Total Score of > 4 sufficiently defined the dysgeusia (Supplementary File 3A and 3B).
Finally, the impairment of appetite levels was separately assessed by using an appetite-dedicated VAS (VASAI): each patient was required to circle numbers [ranging from 1 (no reduced appetite) to 5 (appetite reduced: “very very much”)] which best described his/her condition over the last six months. A VAS total ≥ 2 was sufficient to define an appetite impairment. The used VASAI follows the specific validated CITAS-item 18 and is reported in full in Supplementary File 4. Dysgeusia and appetite levels were assessed after LVP when dACLD patients presented ongoing severe ascites.
Statistical analysisThe sample size was estimated by using a chi-square test confronting two independent proportions, singularly predicting a 50% difference in the prevalence of subjects presenting dysgeusia in the dACLD group compared to cACLD, as well as in the cACLD compared with ≤ F3 group, (significance: 0.05, type II error: 0.1; power: 0.9) (STATA14 for MacOS) and resulted in n 50 individuals for each group.
Continuous data were described as mean and standard deviations, while categorical variables as n (%). The Kolmogorov–Smirnov test for normality was performed to evaluate if the parametric or non-parametric analysis should be applied. Mann–Whitney and t-test for independent groups, the Kruskal–Wallis test, or ANOVA test, with posthoc Dunn-Bonferroni or Tukey–Kramer analysis, according to the non-normal or normal distribution, were performed to compare the continuous variables.
Linear regression analysis was adopted to evaluate the relationship (R) between continuous variables. The log-rank test analysis with Kaplan–Meier curve comparison, including the time-to-event (TTE) analysis, was adopted to determine the risk (Hazard Ratio) (HR) and compare the cumulative incidence (incidence proportion) (IP) and incidence ratio rate (IRR) of further LRDEs in dACLD patients affected by dysgeusia compared to those not affected. Logistic regression (weighted by sex, age, diabetes, BMI, baseline CSPH, administration of NSBB, and human albumin administration) analysis was used to test the variables independently associated (Odds ratios) (OR) with further LRDE occurrence. Statistical significance was defined as p < 0.05 in a two-tailed test with a 95% confidence interval (C.I.). GraphPad Prism vs.10.1.1 was used to perform the analysis.
留言 (0)