
記住我

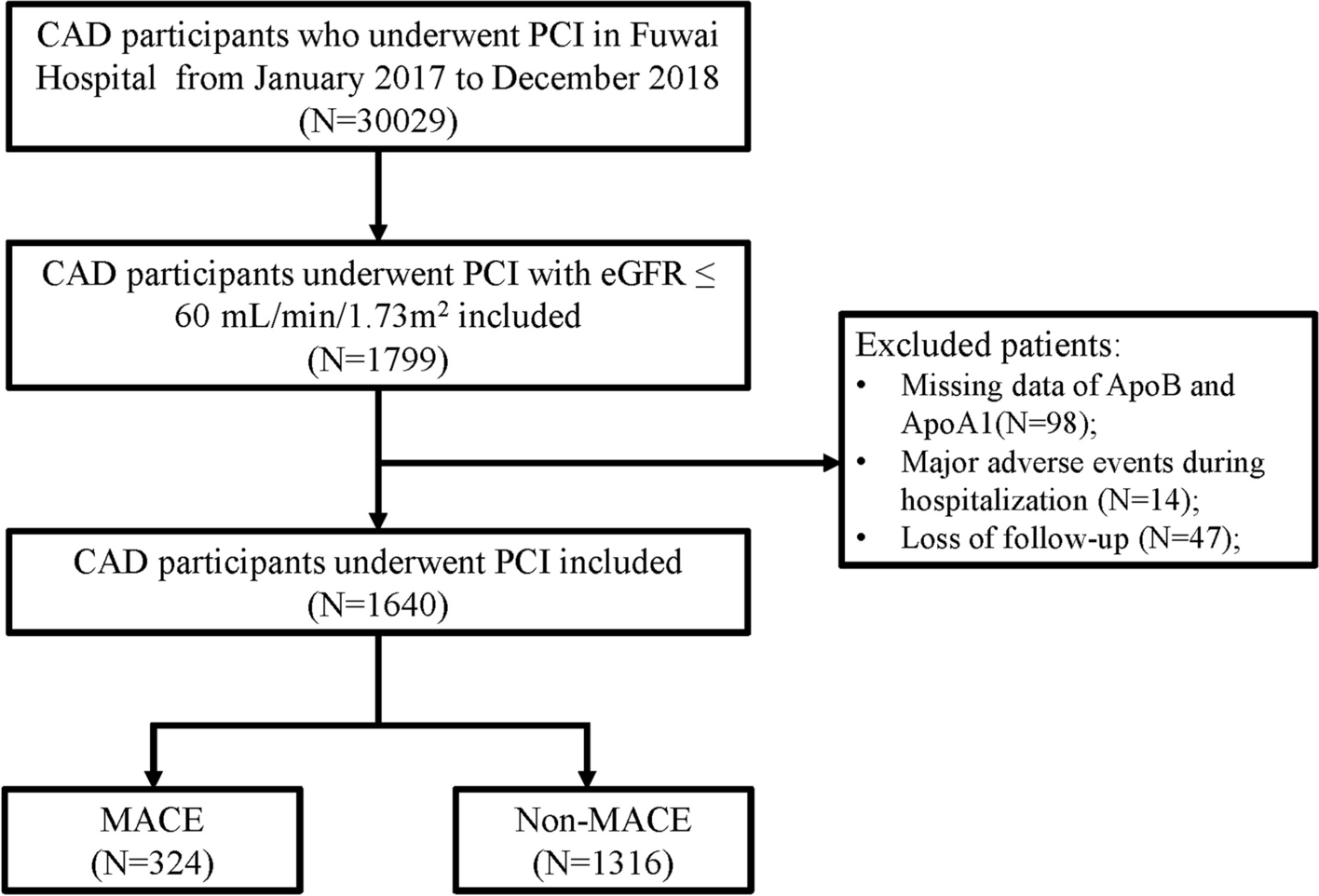



Among a cohort of 1,640 patients, 40.9% were male, with a median age of 69 years. The median eGFR was 53.16 mL/min per 1.73 m2. Table 1 provides a comprehensive overview of the baseline characteristics of participants categorized by MACE outcomes. The prevalence of ACS and DM was found to be higher in the MACE group. Besides, there was a notable upward trend in age, creatinine levels, HbA1C, ApoB, ApoB/ApoA1, TG, LDL, white blood cells (WBC), and stent length when comparing the non-MACE group to the MACE group. Conversely, eGFR, ApoA1, HDL, and hemoglobin (HGB) showed a downward trend.
Apolipoprotein groupsAccording to the multivariable-adjusted RCS analysis, a linear relationship was observed between ApoA1, ApoB, and ApoB/ApoA1 levels with MACE events (P for nonlinear > 0.05). The critical threshold values were 0.76, 1.32, and 0.58, which were close to the median values used for binary classification. Based on the levels of ApoB, ApoA1, and ApoB/ApoA1, patients were stratified into two groups: low-level and high-level groups, with cut-off values set according to the RCS analysis. Survival analysis, as illustrated by KM curves, suggests that stratifying based on these thresholds effectively distinguishes between populations with CAD and impaired kidney function about MACE events, indicating a significant association between these apolipoproteins and MACE occurrences (Fig. 2).
Fig. 2
Relationship between various Apos and MACE risk in patients with impaired kidney function who underwent PCI via RCS analysis (ApoA1(A), ApoB(B), and ApoB/ApoA1(C), cutoff values were 0.76, 1.32, and 0.58, P for nonlinear > 0.05). RCS, restricted cubic spline; MACE, major adverse cardiovascular events; HR, hazard ratio; CI, confidence interval; ApoA1, apolipoprotein A1; ApoB, apolipoprotein B
According to Supplemental Table 1, 837 individuals were assigned to the low ApoB level group, while the remaining 803 were classified into the high ApoB level group. The mean ApoB level in the low-level group was 0.63, compared to 0.93 in the high-level group. Additionally, levels of ApoA1, ApoB/ApoA1, TC, TG, LDL, HDL, hemoglobin, and platelet (PLT) counts all increased with rising ApoB levels.
Furthermore, as indicated in Supplemental Table 1, 834 patients were placed in the low ApoA1 level group (mean ApoA1 value of 1.15), while 806 patients were in the high ApoA1 group (mean value of 1.50). Age, eGFR, ApoB, TC, TG, LDL, HDL, and successful PCI rates all increased with higher ApoA1 levels, whereas creatinine (CR), ApoB/ApoA1 ratio, and WBC counts decreased with rising ApoA1 levels.
Table 1 Baseline characteristic of CAD patients with impaired kidney diseaseAccording to Supplemental Table 2, 820 patients were grouped in the low ApoB/ApoA1 level category (mean value of 0.47), while 806 patients were assigned to the high ApoB/ApoA1 group (mean value of 0.72). The proportions of diabetes, HbA1C, PLT, WBC, ApoB, TC, TG, and LDL all increased with higher ApoB/ApoA1 levels.
Correlation of apolipoprotein levels with MACEDuring a median follow-up period of 3.1 years, a total of 324 MACE events were recorded. This included 165 deaths (10.0%), 77 CV deaths (4.7%), 62 nonfatal myocardial infarctions (3.8%), 19 strokes (1.2%), and 144 unplanned revascularizations (8.8%).
As shown in Fig. 3 and Table 2 both univariable and multivariable Cox regression analyses indicated a statistically significant correlation between high ApoB and ApoB/ApoA1 levels and the increased incidence of MACE (adjusted HR [95%CI] 1.668[1.044–2.666]; adjusted HR [95%CI] 2.231[1.409–3.533], respectively). In contrast, lower ApoA1 levels were also significantly associated with a higher incidence of MACE (adjusted HR [95%CI] 0.505[0.326–0.782]). Consistent results were obtained when different apolipoprotein values were analyzed as both continuous and categorical variables. Tests based on the Schoenfeld Residuals indicated that all analyses met the proportional hazards assumption, allowing for the use of the Cox proportional hazards model (P > 0.05, Supplementary Fig. 1).
Fig. 3
The cumulative incidence for MACE in ApoA1(A), ApoB(B), and ApoB/ApoA1(C) illustrated by Kaplan–Meier survival curves. MACE, major adverse cardiovascular events; ApoA1, apolipoprotein A1; ApoB, apolipoprotein B
Table 2 The relationship between various Apos and MACE risks via Cox regressionMoreover, the results of the ROC curve analysis (Supplementary Fig. 2A) indicated that the predictive performance of ApoA1, ApoB, and ApoB/ApoA1 for MACE risk among CAD patients with impaired kidney function did not differ significantly when incorporated into predictive models. Additionally, there was no noteworthy difference in predictive capability compared to traditional risk stratification factors such as LDL (P for DeLong test > 0.05).
Apolipoprotein levels and clinical outcomesIn various clinical outcomes, both ApoA1 levels and all-cause mortality, along with cardiovascular-related mortality, showed a statistically significant association (adjusted HR [95% CI] 0.234 [0.125–0.437] and 0.181 [0.072–0.454], respectively). There was also a notable positive correlation between ApoB/ApoA1 levels and all-cause mortality and stroke incidence (adjusted HR [95%CI] 2.839 [1.516–5.318], and 5.655 [1.056–17.327], respectively). The correlation of ApoB with various clinical outcomes was consistent with MACE results, although without significant statistical significance (Supplemental Table 4–6). The ROC curve analyses (Supplementary Fig. 2B-F) indicated that the predictive performance regarding different clinical outcomes for CAD patients with impaired kidney function did not markedly differ when ApoA1, ApoB, and ApoB / ApoA1 were included in the predictive models, respectively. Furthermore, the predictive capability remained comparable to traditional risk stratification factors such as LDL, with no significant differences noted (P for DeLong test > 0.05).
Sensitivity analysisAfter excluding patients with CKD stage 5 and those on dialysis, a total of 1,633 CAD patients with impaired kidney function were included in the sensitivity analysis. The results of the Cox regression analysis were similar to those observed in the overall population (Supplemental Table 7). High levels of ApoB and the ratio of ApoB to ApoA1 were associated with an increased incidence of MACE (adjusted HR [95% CI] 1.584 [1.086–2.543] and adjusted HR [95% CI] 2.190 [1.377–3.482], respectively). Conversely, lower levels of ApoA1 were significantly associated with a higher incidence of MACE (adjusted HR [95% CI] 0.496 [0.319–0.771]).
In subgroup analysis, the associations between the aforementioned apolipoproteins (ApoA1, ApoB, and ApoB/ApoA1) and MACE persisted among patients with CAD and an eGFR greater than 45 mL/min/1.73 m2. Specifically, the adjusted hazard ratios were as follows: ApoA1 (adjusted HR [95% CI], 0.391[0.229–0.666]), ApoB (adjusted HR [95% CI], 1.999[1.131–3.534]), and ApoB/ApoA1 (adjusted HR [95% CI] 3.090[1.791–5.331]). However, for patients with moderate to severe renal impairment (eGFR < 45 mL/min/1.73 m2), the associations between these apolipoproteins and MACE did not reach statistical significance (Table 3).
Table 3 The subgroup analysis across various kidney functions via Cox regression
留言 (0)