This study revealed no significant association between IHD and overall ovarian cancer risk. However, a notable finding was the observed protective association between IHD and endometrioid ovarian cancer, with a reduced risk indicated by the MR analysis. This result highlights potential subtype-specific effects of systemic cardiovascular conditions on ovarian cancer. The observed association may be explained by shared biological mechanisms, including chronic inflammation, oxidative stress, and endothelial dysfunction, which are common in both IHD and cancer. Moreover, hormonal regulation and immune responses, known to differ between ovarian cancer subtypes, could play a crucial role in mediating this protective effect. These findings emphasize the need for further research to better understand the interplay between cardiovascular diseases and ovarian cancer subtypes.
Our results suggest that IHD may be a potential protective factor for endometrioid ovarian cancer, while no causal relationship was found between IHD and other ovarian cancer subtypes, such as serous, mucinous, and clear cell ovarian cancers. IHD and its potential association with the risk of endometrioid ovarian cancer may involve several mechanisms, including hormonal levels and pharmacological effects. First, hormonal levels may play a crucial role in this relationship. Particularly in postmenopausal women, where estrogen levels are relatively low, the incidence of IHD is often higher [37]. Lower estrogen levels may reduce the promotive effects of estrogen on endometrioid ovarian cancer cells, thus lowering the risk of cancer development. Estrogen has been shown to play a significant role in the initiation and progression of endometrioid ovarian cancer by promoting the proliferation and metastasis of cancer cells. Therefore, lower estrogen levels may reduce susceptibility to this cancer. Additionally, statins, commonly used in the treatment of IHD, may also exert anti-cancer effects. Statins lower cholesterol levels, improving cardiovascular health, but they may also influence the occurrence and progression of cancer, including ovarian cancer [38]. Studies suggest that statins, by inhibiting HMG-CoA reductase, reduce cholesterol synthesis and modulate the tumor microenvironment, which could help reduce the proliferation of endometrioid ovarian cancer cells. In addition to regulating cholesterol levels, statins may inhibit cancer cell proliferation, metastasis, and induce apoptosis, thereby influencing the development of endometrioid ovarian cancer. Research indicates that statins could provide a potential protective effect through these mechanisms, particularly in relation to IHD. Moreover, statins may also influence the risk of endometrioid ovarian cancer through immune modulation. Statins have been shown to enhance T-cell immune function, which may help suppress tumor development and progression. By reducing inflammation and regulating immune cell function, statins could alter the tumor microenvironment, suppress immune evasion by cancer cells, and lower the risk of endometrioid ovarian cancer as well as other cancers. The immune system plays a critical role in tumor immune surveillance, and modulation of immune responses may represent another pathway through which IHD influences cancer risk. In conclusion, IHD may affect the risk of endometrioid ovarian cancer through changes in hormonal levels, the direct anti-tumor effects of statins, and immune modulation mechanisms. Although these mechanisms provide theoretical support for understanding the relationship between IHD and endometrioid ovarian cancer, further clinical studies and experimental validation are needed to explore these pathways and their potential implications in greater detail.
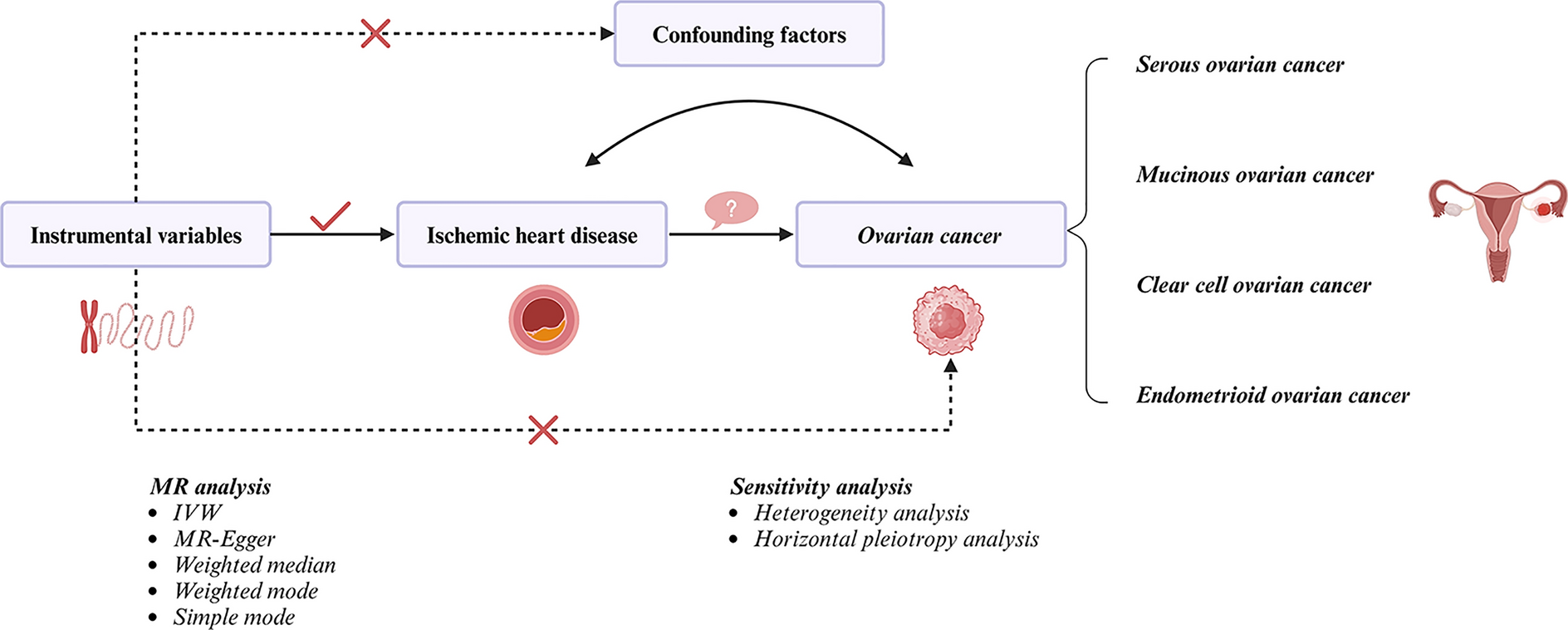
This study addresses a critical gap in the literature by investigating the causal relationship between IHD and ovarian cancer subtypes using a robust MR approach. Prior research has largely focused on the overall link between cardiovascular diseases and cancer, often overlooking the heterogeneity among cancer subtypes. By stratifying analyses according to ovarian cancer subtypes, this study provides novel insights, including a potential protective effect of IHD on endometrioid ovarian cancer, which has not been previously reported. Understanding such subtype-specific associations is crucial for advancing both clinical practice and research, as it enables the development of more tailored prevention strategies and therapeutic interventions. Furthermore, these findings underscore the importance of considering tumor heterogeneity in future research to unravel the complex interplay between systemic diseases and cancer biology.
MR offers distinct advantages over traditional observational studies, especially in assessing causal relationships. By utilizing genetic variants as IVs, MR minimizes the risks of confounding factors and reverse causality, providing a more reliable inference of causal effects. The use of randomly allocated genetic variants ensures that findings are less influenced by environmental or lifestyle factors, enhancing the robustness of the conclusions. Furthermore, rigorous quality control measures in MR, such as ensuring the independence of SNPs and testing for pleiotropy, strengthen the validity of the results. These methodological strengths make MR a powerful tool for studying complex diseases like cancer, offering a more accurate estimate of causal relationships between exposures and outcomes. This study highlights the potential of MR to uncover meaningful biological insights that may inform future research and clinical decision-making.
One possible explanation for the lack of association between IHD and other ovarian cancer subtypes, such as serous, mucinous, and clear cell ovarian cancers, lies in the differing pathophysiology and hormonal dependencies of these subtypes. For instance, serous ovarian cancer is primarily driven by genetic mutations such as BRCA1/2 and TP53, which may have limited overlap with the pathways influenced by cardiovascular conditions like IHD [39]. Similarly, mucinous and clear cell ovarian cancers are characterized by distinct molecular and environmental risk factors, such as chronic inflammation and endometriosis, which may not be directly linked to IHD-related mechanisms [40]. These subtype-specific differences highlight the complexity of ovarian cancer biology and underscore the importance of stratifying analyses by histological subtypes in future research.
However, there are certain limitations inherent in MR studies [41]. One of the major concerns is the potential for horizontal pleiotropy, where genetic variants influence multiple traits, which could bias the results. While we performed rigorous tests to detect and correct for pleiotropy, it remains a limitation that requires careful consideration. Another limitation is the selection of appropriate instrumental variables. In this study, we ensured that the SNPs used were strongly associated with IHD and independent of each other, but the choice of genetic proxies is always crucial in MR analysis. Additionally, while MR can suggest causal relationships, it does not fully capture the biological mechanisms behind these associations. Further research, including functional studies, is needed to investigate how IHD could influence endometrioid ovarian cancer at the molecular and cellular levels. Finally, despite the use of MR to reduce confounding, there remains the possibility of residual confounding. While MR is less susceptible to confounding and reverse causation compared to traditional observational studies, it could still be influenced by unmeasured or inadequately controlled confounders. For example, although we have adjusted for multiple potential confounders by selecting appropriate genetic variants, factors such as lifestyle, environmental exposures, or other genetic influences not captured in the study could still affect the results. Therefore, while our findings suggest a potential causal relationship between IHD and ovarian cancer, further research, including experimental and cohort-based studies, is needed to confirm these results and explore other potential confounding factors.




留言 (0)