In the US, it is estimated that ovarian cancer (OC) will result in 12,740 deaths in 2024 [1]. Approximately 90% of OCs are epithelial in origin [2]. Although several biomarkers have been identified to contribute to the development of OC [3], effective screening approaches have not been established to date [4], and most patients present with advanced disease at the time of diagnosis [1]. Standard first-line (1L) treatment for advanced OC consists of either primary cytoreductive surgery (PCS) or interval cytoreductive surgery and platinum-based chemotherapy, alone or in combination with the vascular endothelial growth factor inhibitor bevacizumab [5,6,7]. Although most patients with OC respond to standard 1L treatment, approximately 70% experience disease progression within 3 years, and the 5-year survival rate for patients with advanced epithelial OC (EOC) is 31.4% [5, 7, 8]. Postsurgical residual disease is a known poor prognostic factor, and patients with visible residual disease (VRD) after surgery experience poorer clinical outcomes than those with no visible residual disease (NVRD) [7, 9,10,11].
The potential for maintenance therapy to reduce the risk of disease progression or death after 1L therapy for advanced EOC has been the subject of ongoing investigations, and available 1L maintenance (1LM) treatment options include bevacizumab, poly(ADP-ribose) polymerase (PARP) inhibitors, and the combination therapy of bevacizumab plus a PARP inhibitor [12, 13]. PARP inhibitor 1LM is recommended for patients with advanced EOC who achieve a complete or partial response to 1L platinum-based chemotherapy to delay disease progression or recurrence [12, 14].
Niraparib, a PARP inhibitor, was approved for use as 1LM therapy in patients with advanced EOC on the basis of results from the phase 3 PRIMA/ENGOT-OV26/GOG-3012 (PRIMA) trial (NCT02655016), in which improvement in progression-free survival (PFS) was demonstrated among patients who received 1LM niraparib monotherapy as compared with placebo [15, 16]. In PRIMA, patients at higher risk for recurrence (defined as stage IV disease, or inoperable stage III disease, or suboptimally debulked [> 1 cm] stage III disease), were included in the study, and patients with stage III EOC who had NVRD after PCS were excluded from enrollment [7, 15, 17]. In contrast, the PRIME trial, a randomized, phase 3 study with a design similar to that of the PRIMA trial, included patients with stage III NVRD after PCS. In the PRIME trial, the median PFS in patients treated with niraparib (overall intent-to-treat population: 24.8 months [95% confidence interval (CI), 19.2 months to not estimable]) was longer than that in the PRIMA trial (overall cohort: 13.8 months) [15, 18]. It is not known whether the exclusion or inclusion of patients with higher risk prognostic factors accounted for differences in the magnitude of PFS benefit with niraparib between the PRIMA and PRIME trials.
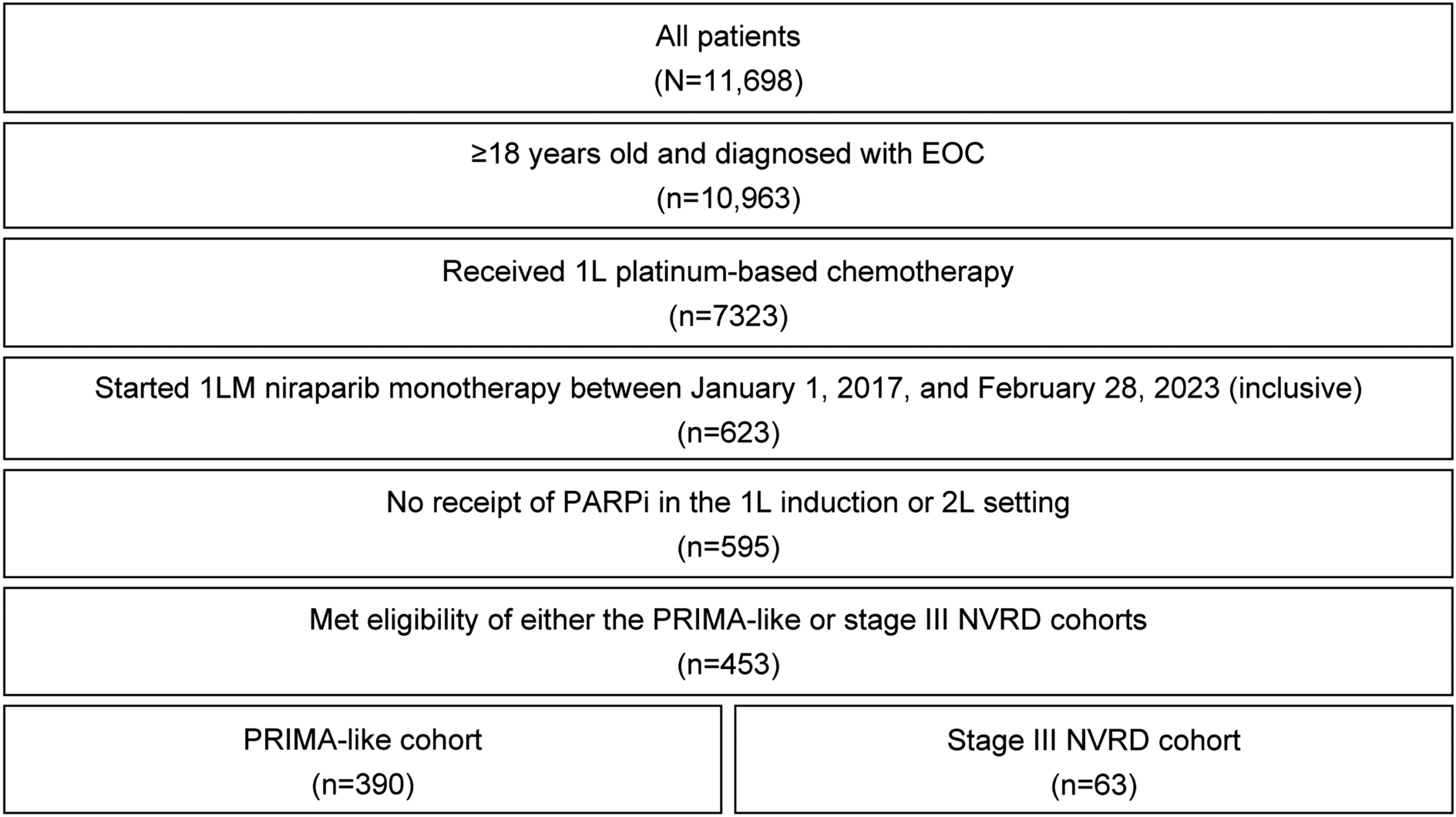
The aim of this retrospective, observational study was to evaluate the potential impact of excluding patients with stage III EOC with NVRD from the PRIMA trial by assessing real-world treatment outcomes in patients who were treated with 1LM niraparib monotherapy in this patient population versus a PRIMA-like population.


留言 (0)