CS are cartilage-forming malignant mesenchymal tumors infrequently occurring in the head and neck region (1–12%) and particularly rare in the larynx [42]. A diagnosis of laryngeal CS was first made in 1935 by New [43], and its etiology has since then remained essentially unknown [6]. About 95% of CS are low-intermediate grade (G1–G2) tumors [34, 44]. Even though the latest WHO Classification of Head and Neck Tumors (2024) [8] states that “tumor location, grade, subtype, and therapy do not seem to influence outcome (other than possibly for dedifferentiated tumors),” this assumption may be hampered by the exceedingly rare occurrence of the most aggressive forms of CS, per se already an infrequent diagnosis. In fact, laryngeal G3 CS represents a very rare (or absent) occurrence even in the largest series in the literature [3, 7, 9,10,11], and this means that even tertiary, academic, head and neck cancer referral centers may encounter such clinical scenarios once per decade or even less often. Histologic grade is the most significant prognostic factor for metastatic relapse, occurring in about 70% of G3 [45,46,47] and 31% of MY CS [48] at all sites. Such figures are lacking for laryngeal CS because of their intrinsic rarity even though the clinical impression is that certain subtypes even in this location may display a more aggressive behavior with higher rates of loco-regional and distant recurrences compared to their well-differentiated counterparts.
The MY subtype, originally believed to be a slow-growing and low-grade CS, showed high rates of local recurrence and distant metastasis in long-term follow-up studies [12, 49], especially when associated with high cellularity and low myxoid content [12]. Distant metastases are more common than regional ones, and most metastatic CSs are poorly differentiated or DD [50].
Aggressive subtypes of laryngeal CS, due to higher rates of metastasis and poorer prognosis (5-year overall survival [OS] < 10–25% for DD at all sites) [46, 47], emphasize the need for comprehensive removal of the lesion at its first presentation. This means that an organ-sparing surgical philosophy (i.e., TOLMS or open partial laryngectomies) can be adopted if it is aimed at obtaining the most representative sample of the lesion (within R0 or R1 margins) and rule out its possible aggressive nature. In case of a final histopathologic diagnosis of a G1–G2 lesion, such an approach can be reasonably followed by close endoscopic and/or radiologic surveillance, whereas when a G2–G3/G3, DD, and possibly also MY CS have been identified, a more aggressive surgical resection should be discussed with the patient in a multidisciplinary environment.
Unfortunately, due to the rarity of laryngeal G3, DD, and MY CS, the published literature is scarce and generally represented by case reports or very small retrospective case series, based on which strong recommendations are difficult to formulate.
Patient and Tumor Characteristics
In line with the available literature [3, 23], the aggressive subtypes of laryngeal CS occurred more frequently among males older than 50 years, differently from CS arising in other head and neck subsites (skull base or maxillofacial bones) that most commonly occur in 50-year-old or younger women. Local symptoms of G3, DD, and MY may not be different from their less aggressive counterparts and usually include hoarseness, along with progressive dyspnea and dysphagia, the latter especially frequent when the neoplasm has a posterior location compressing the post-cricoid portion of the hypopharynx. However, if not involving the glottis by ankylosing a crico-arytenoid joint, these tumors may remain asymptomatic for long periods and sometimes be incidentally discovered during endoscopic or intubation procedures. A non-negligible subgroup of aggressive CS may also exhibit unusual symptoms such as an enlarging neck mass, pain, and hemoptysis at diagnosis, which are not reported in the most common G1–G2 lesions.
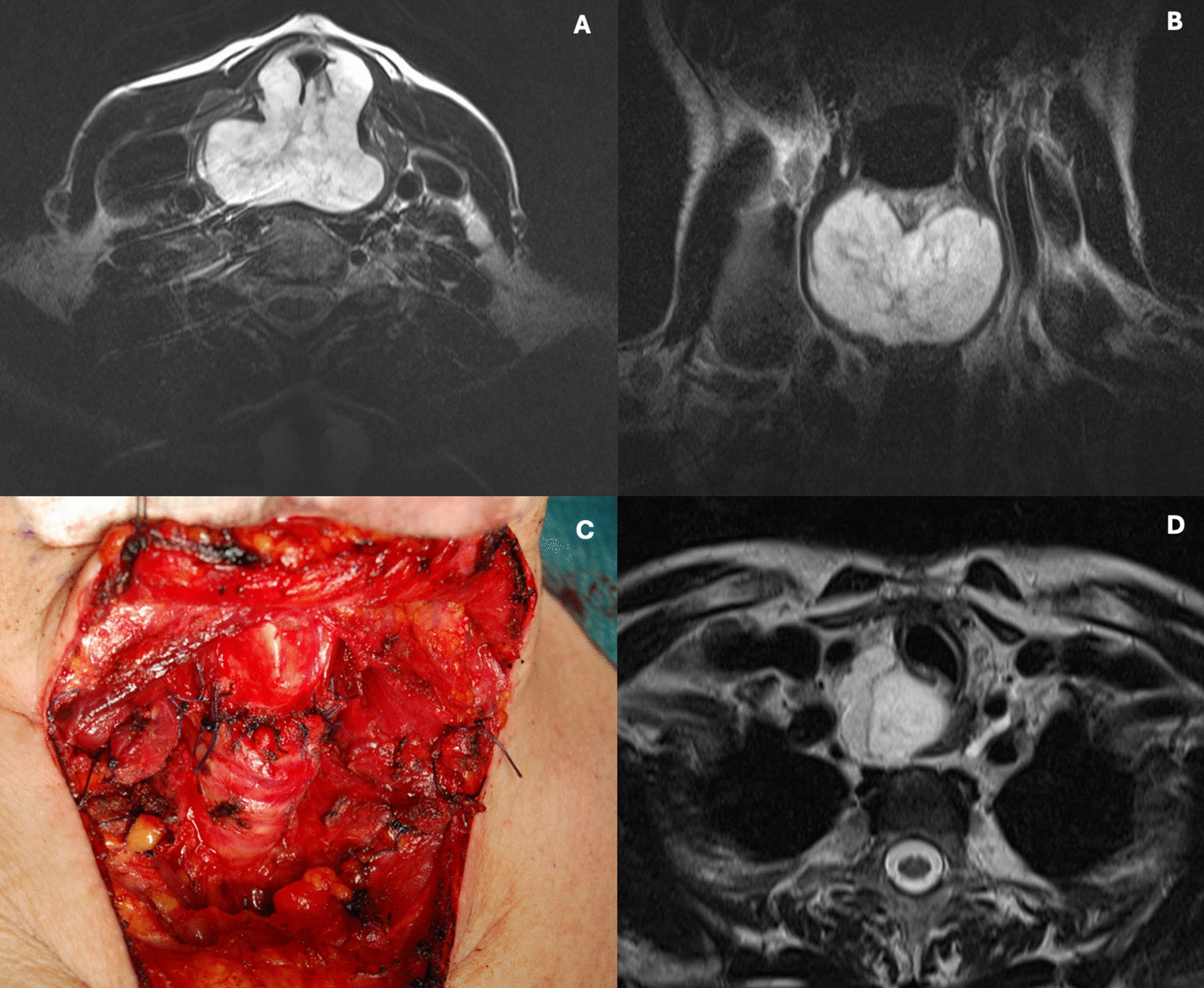
Laryngoscopy followed by computed tomography (CT) and/or magnetic resonance (MR) are fundamental diagnostic evaluations allowing definition of the cartilaginous nature of the lesion due to its pathognomonic appearance at imaging, even though its grading requires assessment of the entire lesion, which can be difficult in small biopsy samples in particular [9]. From a histopathologic point of view, we confirm the exceedingly rare incidence of the more aggressive subtypes of CS, with only 38 patients documented in a literature review spanning 24 years [3, 19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38]. Preoperative diagnosis of CS can be difficult outside high-volume referral centers and can sometimes be misdiagnosed or, more frequently, down-graded based on small biopsy specimens that are not representative of the entire lesion. In our systematic review, one case [35] was first diagnosed as a reparative giant-cell granuloma and aneurysmal bone cyst arising from the cricoid, and only after several recurrences and TL was it correctly identified as a DD CS.
Preoperative CTs and/or MRs are definitely useful to make a presumptive diagnosis of cartilaginous tumor and evaluate its site of origin, three-dimensional extent, and dimensions but are usually not able to establish a differential diagnosis among different subtypes and the degree of biologic aggressiveness. In particular, CT detects “popcorn” calcification and MR identifies high-intensity signals in T2, which are both highly specific for CS [51]. The association of radiologic characteristics, large dimensions (> 4 cm), clinical data (such as rapid growth or soft tissues involvement and atypical symptoms), and histologic evaluation of a large sample is helpful in establishing the correct diagnosis. A representative biopsy or, even better, definitive histologic evaluation of the entire surgical specimen allows assessment of the possible coexistence of areas with varying degrees of differentiation.
According to the literature, CSs arise from hyaline cartilage, and the cricoid is the most common site of origin (66.7% in our study population compared to 75% commonly reported in the literature, also including the less aggressive subtypes) [23]. In particular, the posterior lamina of the cricoid cartilage accounts for most of the malignancies [3], probably in association with an age-related ossification phenomenon, classically starting where the posterior crico-arytenoid muscles insert [52]. We found only one case (4.1%) originating at the level of the epiglottis [23], in line with the 3% involvement of the epiglottis or accessory cartilages reported previously [25]. However, due to the frequently large dimensions of aggressive CS at diagnosis, the precise site of origin of these tumors often remains unknown.
Treatment
Surgery is the mainstay of treatment. A conservative approach is often chosen for G1–G2 CS when at least one crico-arytenoid joint, posterior crico-arytenoid muscle, and recurrent laryngeal nerve can be safely preserved together with a reasonable laryngeal function [7, 16, 53, 54]. The reason is the indolent, non-aggressive, and non-metastatic course of these lesions that allows even multiple, repeated conservative resections without affecting OS. However, a different approach must be considered for the more aggressive subtypes. A surgically conservative approach should be applied only for diagnostic purposes but, once a G3, DD, or even MY CS has been diagnosed, their relatively poor prognosis and higher local and distant recurrence rates should prompt a more radical approach. Indeed, TL was the most common treatment (69%), performed in 73.3% of G2–G3/G3, 61.5% of DD, and 10% of MY (the type of surgical approach was not available for 80% of MY) [3]. Among the patients treated with conservative approaches, 42.8% had loco-regional recurrences [19, 21, 30, 35, 38].
In 1973 [55], Jones gave some useful indications for TL as treatment of CS. According to his view, TL should be applied to tumors with extensive laryngeal involvement and ensuing inability to preserve airway patency, recurrences after previous treatments, and dedifferentiated histology (such as in the present systematic review). Aggressive CS subtypes and bilateral massive involvement of the posterior lamina of the cricoid cartilage or both cricoarytenoid joints make TL the first choice of treatment, particularly in the presence of DD CS. In this review, primary surgical conservative approaches were proposed in 48.3% of patients [3, 19,20,21, 25, 29, 30, 32, 34,35,36, 38], but 42.8% experienced loco-regional recurrences and 35.7% underwent TL for local recurrence after a mean of 35.6 months [19, 21, 30, 35, 38].
Controversy still exists regarding laryngeal function-sparing excision versus TL for treatment of laryngeal CS. When feasible, a conservative approach in G1–G2 CS is better because it seems that the ultimate cure rate after TL performed for recurrent disease is comparable to that of primary TL (77 vs. 86%) [40, 56, 57]. In general, transoral treatment is possible only for small lesions or to debulk large tumors and get a proper diagnosis, with laser, allowing better control of resection and bleeding. In the literature, series of CS [7] treated with TOLMS are reported but mostly concerning G1–G2 CS. Indeed, herein TOLMS was performed in only two patients [25, 29]. On the other hand, several different open partial laryngeal resections have been described, while the aim of systematizing their use and indications is far from the scope of this paper. No guidelines are available for regional surgical treatment, but lymphatic spread of laryngeal CS seems to have a low incidence.
CSs have been classically considered radio-resistant tumors. However, recently this concept has gradually evolved, and new radiation modalities have proven useful in these lesions, especially when resection within free margins cannot be obtained [27]. Even if not indicated for G1–G2 lesions, adjuvant RT is recommended in G3 or aggressive subtypes of CS, especially in cases with involved margins [58]. In our cohort, 42.1% of patients received adjuvant treatments, in particular RT (n = 15) [3, 21, 22, 24, 27,28,29, 33, 34, 38], CRT (n = 2) [26, 30], or CHT only (n = 1) [29].
Even if CSs rarely are good responders to CHT and this approach is applied only for metastatic unresectable CS, DD seems to be more sensitive to CHT compared to conventional CS [1]. According to Italiano and coworkers [1], systemic conventional CHT significantly improved survival compared to no treatment, while the number of chemotherapeutic agents used (single vs. multiple) did not significantly improve OS. Several types of CHT regimens have been used for CS, usually including anthracycline (doxorubicin), but also gemcitabine-based combinations, dacarbazine, oral etoposide, and ifosfamide [1].
Promising therapeutic modalities include the use of proton and carbon beam irradiation. However, although it has been used to treat skull base CS with a good rate of local control (92%) [59], there is currently no evidence for laryngeal tumors. Immunotherapy, particularly immune checkpoint inhibition targeting the PD-1/PD-L1 pathway, is an emerging area of clinical research. Studies have shown increased PD-1 expression in non-laryngeal CS compared to normal bone, with PD-L1 expression correlating with factors like tumor grade, size, and recurrence [60, 61]. Although PD-L1 levels and tumor mutational burden are generally low in sarcomas, an analysis of the expression of PD‐L1 protein in conventional mesenchymal, clear cell, and DD CS revealed an upsurge in PD‐L1 expression in 41% of DD CS [62, 63]. Clinical responses to immune checkpoint blockade remain mixed but show potential, especially in tumors with higher PD-L1 expression, but no data about laryngeal CS have been reported in the literature so far.
Oncologic Outcomes
In general, head and neck CSs have a better disease-specific survival (DSS) at 5 and 10 years (87.2% and 70.6%, respectively) compared to other sites, even if the anatomic complexity and functional density in this area often make it difficult to obtain clear resection margins. Not surprisingly, the local recurrence rate is higher than in other sites [64–67]. Laryngeal CS appears more favorable than CS in other parts of the body, even if G3 and DD behave similarly in the larynx and elsewhere, still remaining aggressive subtypes [1, 6, 19].
G3 and DD CS have a metastatic potential of 70% [42, 47, 68] and, even after radical treatment, the 10-year survival rate is around 29% [47] compared to 47.6% and 53.6% for all CS [2, 3]. The recurrence rate after surgery with or without adjuvant RT remains high (35–40%) [48]. In our systematic review, the recurrence rate was 33.3% with a mean time of 21.6 months, which is considerably shorter than the recurrence time usually reported for G1–G2 lesions [7, 9, 15]. Recurrences appeared in 33.3% of G2–G3/G3, 46.2% of DD, and 10% of MY CS. Five cases of loco-regional relapse were treated primarily with conservative surgery, while most cases with distant metastases were first treated by TL, and only two cases received palliative lung metastasectomy [27, 38]. Comparing the recurrence rate after TL performed as first-choice treatment with that after TL when other treatments had failed, the surgical curative rate was apparently not affected. In our population, all salvage TL patients, except for two whose follow-up was not available, were alive without evidence of disease, while among primary TL, except for one lost to follow-up, seven had died (4 of disease and 3 for other causes). Indeed, recurrence does not seem to affect survival and overall outcomes [57]. In our population, 66.7% of patients were alive without evidence of disease at the end of follow-up, and death from disease was rare, usually related to uncontrolled local growth or untreatable distant metastasis.


留言 (0)