
記住我
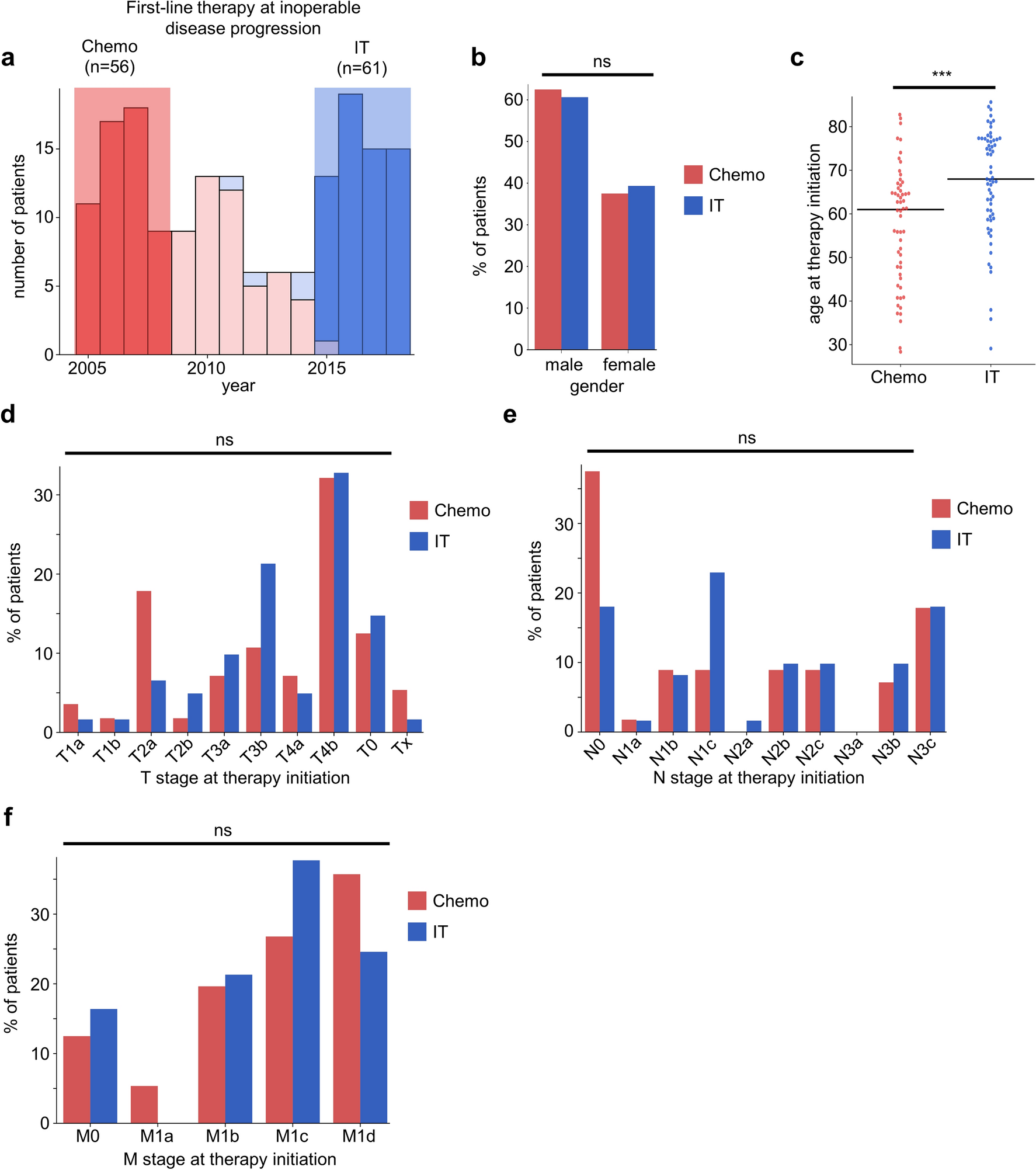

For our current study, we generated two patient groups with inoperable metastatic melanoma that were either treated only with IT or only with chemotherapy in our department. To minimize the risk of confounding effects of prior adjuvant therapies, we chose to include in the IT group only patients from 2015 until the introduction of adjuvant IT in 2018 (Fig. 1a, Table 1). To generate a similar group of patients that were only treated with chemotherapy, we selected the period from 2005 to 2008 long before the introduction of IT (Table 1). In a first step, we characterized the composition of the IT and chemotherapy patient groups. Whereas both groups showed a similar distribution of male and female patients (Fig. 1b), patients treated with chemotherapy were significantly younger compared with patients treated with IT (Fig. 1c). This difference might be due to the good tolerability of IT, so that more elderly patients were eligible for therapy. Next, we compared the TNM stages of patients at therapy initiation. Most patients from both groups harbored primary tumors from high-risk T stages ≥ T3 (Fig. 1d). Patients from the chemotherapy group showed fewer locoregional metastases, with 37.5% of patients in N0 stage (Fig. 1e). Furthermore, we observed a trend towards patients affected by metastases outside of the brain (M1c) in patients treated with IT, whereas a higher proportion of patients treated with chemotherapy showed brain metastases (M1d) without reaching statistical significance (Fig. 1f).
Fig. 1
Group characteristics at therapy initiation of patients treated with IT and chemotherapy. a Number of patients with inoperable melanoma receiving systemic therapy. Shaded areas indicate the patients included in subsequent analyses. b Distribution of genders between IT and chemotherapy groups at therapy initiation. ns not significant, Fisher’s exact test. c Patient age at therapy initiation. Black bars indicate the median. ***p < 0.005, Mann–Whitney U test. d–f Distribution of T (d), N (e), and M (f) stages of patients at therapy initiation. ns not significant, Mann–Whitney U test. IT immunotherapy
Patients with Inoperable Metastatic Melanoma Treated with IT Show Higher Response Rates and Longer Overall Survival Compared with Patients Treated with ChemotherapyIn order to assess how the introduction of IT has changed the treatment of patients with advanced melanoma, we compared the therapy response rates and the overall survival for the patient group treated with IT to the patient group treated with chemotherapy. As expected, patients treated with IT showed a significantly improved ORR (IT 42.5%, chemo 3.6%, p < 0.005) and longer overall survival compared with patients treated with chemotherapy (Fig. 2a, b). These findings are comparable to previously published reports [25]. Whereas patients treated with IT frequently showed durable responses to therapy, most patients treated with chemotherapy demonstrated no or only brief therapy responses (Fig. 2c). These data demonstrate that the efficacy of IT observed in clinical trials successfully translates into improved patient outcome in a real-world setting.
Fig. 2
Outcome and therapy response characteristics of patients treated with IT or chemotherapy. a Overall survival of patients with inoperable melanoma treated with IT or chemotherapy. The shaded area indicates the 95% confidence interval. ***p < 0.005, log rank test. b Objective response of first-line therapy stratified by treatment regimen. For the statistical analysis, the objective response rates from patients treated with chemotherapy and patients receiving IT were compared. ***p < 0.005, Fisher’s exact test. c Swimmer plot of the inoperable melanoma group. Patients are ordered by the response achieved by first-line therapy. Colors indicate the best therapy response. Deceased patients are indicated by crosses. IT immunotherapy, HR hazard ratio, CI confidence interval, CR complete response, PR partial response, SD stable disease, PD progressive disease
Patients Treated with IT Do Not Show an Altered Pattern of Metastatic Disease Progression Compared with Patients Treated with ChemotherapyThe efficacy of IT depends on the activation of cellular immunity. The brain is considered to be an immune-privileged organ as a result of the restriction of leukocyte trafficking into brain tissue due to the blood–brain barrier [21]. Similarly, the liver is also regarded as an immune-privileged organ because of the potential to induce immune tolerance and thereby suppress immune activation [27]. We hypothesized that the pattern of metastatic progression would differ between patients treated with IT and chemotherapy. Specifically, we expected that patients treated with IT would more frequently develop metastases in the immune-privileged organs liver and brain. To address this hypothesis, we compared the frequency of melanoma metastases in different organs at therapy initiation and at disease progression for the patient groups treated with IT or with chemotherapy. We did not observe statistically significant differences in the frequency of metastases at therapy initiation at any target site between patients treated with IT or chemotherapy (Fig. 3a), highlighting the comparability of our groups. Both patients from the IT and chemotherapy groups showed an increase in the frequency of brain and liver metastases with disease progression (Fig. 3a, b). Patients treated with chemotherapy showed a higher frequency of brain metastases during treatment compared with patients treated with IT without reaching statistical significance (Fig. 3a, b). Furthermore, patients showed a trend towards harboring fewer skin metastases during treatment with IT (Fig. 3a, b). Next, we assigned six distinct metastatic patterns to patients on the basis of the presence of metastases to the immune-infiltrated organs skin and lymph node only, additional metastases to the lung or visceral organs excluding liver and brain, or metastases to the immune-privileged organs liver, brain, or liver and brain. We found that patients treated with chemotherapy showed a higher proportion of the “brain” pattern compared with patients treated with IT both before and during therapy (Fig. 3c, d). Patients treated with IT instead showed a higher frequency of the “lung” pattern during disease progression (Fig. 3d). Because the frequency of patients receiving IT harboring lung metastases did not increase during disease progression (Fig. 3a, b), we hypothesize that the increase of patients with the “lung” pattern indicates the efficacy of IT in preventing further metastatic dissemination to other organs such as liver or brain. Subsequently, we compared the overall survival between patients treated with chemotherapy and IT stratified by the metastatic patterns at therapy initiation. Interestingly, while patients from all metastatic patterns treated with IT showed improved overall survival compared with patients treated with chemotherapy, IT-treated patients harboring the “liver” pattern showed the poorest overall survival compared with the other metastatic patterns (Fig. 3e). In summary, these results show that patients treated with IT showed no alteration in the pattern of metastatic disease progression compared with patients treated with chemotherapy. However, our findings suggest that patients treated with IT harboring liver metastases show worse outcome compared with patients with metastases in other organs.
Fig. 3
Patients with liver metastases show poor outcome despite therapy with IT. a, b Proportion of patients grouped by the metastatic target site at therapy initiation (a) or during metastatic disease progression (b). Patients with multiple metastases were counted for each metastatic site group. ns not significant, Mann–Whitney U test. c, d Patients were classified into six different metastatic patterns based on the presence of metastases in specific target sites. Shown are the frequencies of patterns for patients before therapy initiation (c) or during metastatic disease progression (d). e Kaplan–Meier survival curves for overall survival of patients treated with chemotherapy or IT stratified by metastatic pattern at therapy initiation. IT immunotherapy, LN lymph node
Patients Treated with IT Show Longer Survival After Metastatic Progression to Lymph Node, Lung, or Brain But Not After Metastatic Progression to the Liver Compared with Patients Treated with ChemotherapyAfter we observed an unfavorable outcome of patients treated with IT harboring liver metastases compared with patients with metastases in other organs, we sought to understand which metastases ultimately limit patient survival. For this, we analyzed the time from metastatic disease progression until death, which we termed post-progression survival. Patients treated with chemotherapy showed a similar post-progression survival for all analyzed metastatic target sites, with a median of 2.9–4.0 months from metastatic progression to the lymph node, lung, liver, or brain until death (Fig. 4a, d). Patients treated with IT showed a significantly more favorable outcome after metastatic progression to lymph node or lung compared with patients treated with chemotherapy (Fig. 4a, b). Interestingly, patients with metastatic progression to the brain also showed a prolonged post-progression survival after treatment with IT, whereas patients with metastases in the liver showed short post-progression survival with no difference between the IT and chemotherapy group (Fig. 4c, d). These results suggest that metastases to the liver might ultimately limit patient survival of patients treated with IT.
Fig. 4
The onset of liver metastases is associated with a short post-progression despite treatment with IT. Survival of patients after onset of metastatic disease progression to lymph node (b), lung (c), liver (d), or brain (e). The shaded area indicates the 95% confidence interval. ns not significant, *p < 0.05, log rank test. IT immunotherapy, HR hazard ratio, CI confidence interval, LN lymph node
留言 (0)