
記住我


Overall, 1000 participants living with LC answered the questionnaire. About half (n = 495, 49%) lived in Europe, while the other half were divided between North America (n = 289, 29%) and Asia (n = 216, 22%). Female patients accounted for 44% (n = 441) of the respondent population, with a higher rate in the UK (n = 73, 82%) and lower rates in Spain (n = 33, 33%) and Japan (n = 13, 13%). The median age of the respondents was 52 ± 13 years, with older participants in the UK (66 ± 8 years) and in Japan (63 ± 11 years). Participants were mainly former smokers (n = 667, 67%), while current smokers accounted for 17% (n = 172) and never smokers for 16% (n = 159). See Table 1 for the sociodemographic profile of the respondents.
Table 1 Sociodemographic profileTime since diagnosis was a mean of 2.5 years (95% CI 2.3–2.7), with longer disease history in Japan (3.9 years [95% CI 3.3–4.6]) and shorter in the UK (1.2 years [95% CI 0.7–1.7]). Although most participants (69%) were diagnosed in the last 2 years, 12% had been diagnosed over 6 years ago. When asked about their type of cancer, 47% (n = 465) of respondents indicated NSCLC, 32% (n = 321) SCLC, 6% (n = 64) neither NSCLC nor SCLC, and 15% (n = 150) “unknown”—the last of these driven by high rates in Japan, the UK, and France (36%, 23%, and 23%, respectively). When asked about their stage at diagnosis, many reported early stage (n = 555, 56%) and locally advanced stage (n = 315, 32%); 11% (n = 106) were diagnosed at advanced metastatic stage. Canada reported a higher rate of early stage diagnosis (n = 60, 75%) and the UK reported a higher rate of advanced stage diagnosis (n = 24, 27%). Disease characteristics of the respondents are summarized in Table 2.
Table 2 Disease characteristicsDiagnostic PathwayOn average, participants reported 2.9 (± 1.7) initial symptoms that led them to consult a physician prior to the LC diagnosis. The main five symptoms which made patients decide to go to see a physician were cough (58%), chest pain (42%), shortness of breath (38%), fatigue (37%), and coughing up blood/ mucus (30%). The three main comorbidities reported were chronic obstructive pulmonary disease (COPD) (31%), asthma (22%), and diabetes (12%); whilst 4 out of 10 patients reported not having comorbidities (41%). Pulmonologists/respiratory specialists (P/RS) were the main physicians who made the LC diagnosis (n = 526, 53%), followed by primary care physicians/general practitioners (PCP/GP) (n = 206, 21%) and medical oncologists (MO) (n = 170, 17%).
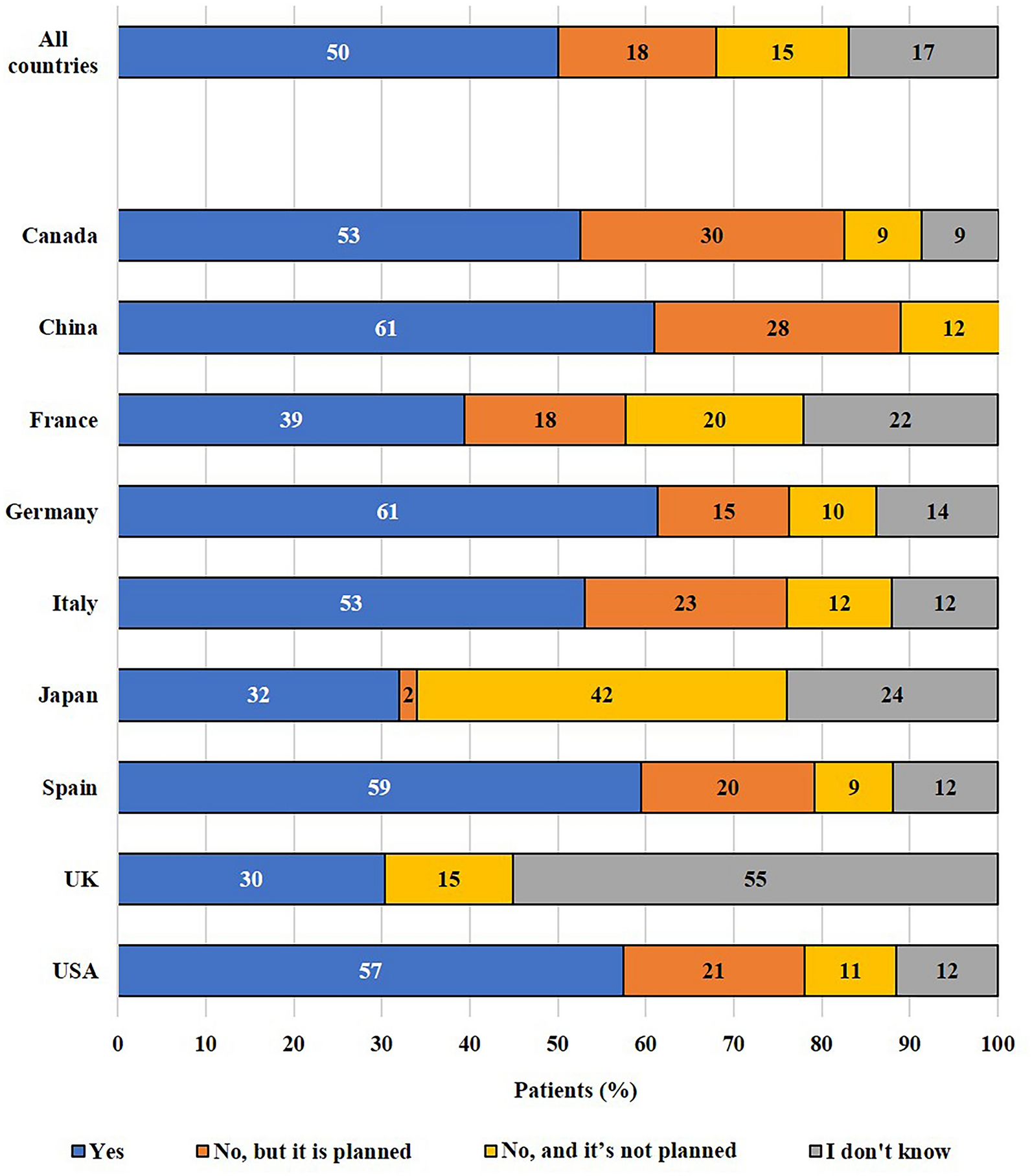
In total, 68% (n = 681) of respondents reported having been tested or planned to be tested for genetic mutations or biomarkers; 15% (n = 151) did not plan to be tested and 17% (n = 168) did not know about their testing status (Fig. 1). Participants living in China reported the highest rate of testing actual/planned (n = 92, 88%), with also high rates from Italy, Spain, Germany, the USA, and Canada (76–83%). The lowest rates were reported in the UK and Japan of testing actual/planned (27 and 34%, respectively). In the UK, a high proportion of respondents (n = 49, 55%) were not aware if genetic/biomarker analyses took place or not.
Fig. 1
Genetic mutation or biomarker testing reported
Treatment Decision ExperienceAlmost three-quarters of participants have undergone surgery for their LC or plan to (n = 737, 74%). Apart from surgery, the initial treatment administered to participants after LC diagnosis was chemotherapy (n = 408, 41%), followed by radiotherapy or radio-chemotherapy (n = 235, 24%), immunotherapy or immuno-chemotherapy (n = 135, 14%), and targeted therapy (n = 79, 8%). Overall, 11% of patients (n = 112) did not receive any treatment at the time they answered the survey.
Concerning the choice of treatment, respondents reported being most influenced by their physicians (Fig. 2). Patients’ family and relatives also ranked highly and seem to play a greater role in the choice of treatment in China, the USA, and Canada (as reported by ~ 50% participants) than in other countries; participants from Japan reported the lowest rate of family influence (n = 23, 21%).
Fig. 2
Main people or sources influencing the choice of treatment. Multiple answers allowed, up to three choices. The following other people/sources were selected by less than 10% of respondents: patient advocacy or support group, specialists from an independent telehealth service, experiences shared from other patients with lung cancer, information found on the internet, nurse, pharmacist, I have taken this decision on my own
When asked about the main reasons to start a specific LC treatment, respondents reported wanting to live longer (n = 535, 54%), to control the cancer (n = 530, 53%), that the treatment was recommended by their physician (n = 512, 51%), and to improve their QoL (n = 442, 44%) (Fig. 3a). Physician recommendation ranked higher in Japan and France (reported respectively by 66% and 57% of participants), but lower in Italy and China (37% and 43%, respectively).
Fig. 3

Main reasons to choose a lung cancer treatment (a) or not to start a lung cancer treatment (b). Multiple answers allowed. QoL quality of life
Participants reported the main reasons for hesitating to start a specific LC treatment to be side effects interfering with daily life (n = 326, 33%), concerns about long-term side effects (n = 298, 30%), and overall treatment impact on QoL (n = 290, 29%) (Fig. 3b). More patients living in China were concerned about long-term treatment side effects (46%) than observed in other countries. Doubts about treatment efficacy were country-dependent: from low doubt (UK, 8%) to highly concerned (28–38%) in the USA, Japan, Canada, and China. Similarly, concern about treatment cost varied, with fewer respondents concerned in the UK (3%) and Canada (5%), and the highest proportion concerned in China (38%) and Japan (29%).
Since the 5-year overall survival in patients living with LC is quite poor—especially in the metastatic stage [11]—earlier detection methods and new treatment modalities are required; therefore, we asked about clinical trials participation. A total of 221 respondents (22%) have participated in a clinical trial for LC. For many patients (n = 582, 58%), participation in a clinical trial was never offered as a potential treatment option for LC, although a significant proportion of them (n = 375, 38%) would have been interested. Highest percentages of participants not being asked to participate in clinical trials were reported in France, Italy, Japan, and the UK (70–85%).
Impact of the DiseaseWhen asked about the impact of LC, participants reported that their disease affected many areas of their daily life, with physical well-being (n = 507, 51%), daily activities (n = 487, 49%), mental well-being (n = 484, 48%), working life (n = 380, 38%), and social life (n = 341, 34%) being the main aspects impacted (Fig. 4a). Participants in Canada reported a higher rate of difficulties in their working life (n = 45, 56%), with the smallest impact observed in the UK (n = 24, 27%). In Japan, the impact of LC on the aspects of patients’ daily life was lower than other countries across all categories, except finances.
Fig. 4

Impact of lung cancer diagnosis on patient’s daily life (a) and on employment status (b). Multiple answers allowed
Between 27% and 56% of participants per country reported their lung cancer diagnosis caused difficulties in their working life—the most reports came from participants in Spain, the USA, and Canada (44–56%), the least reports were in the UK and Japan (27%). About half of the respondents (n = 510, 51%) reported that their employment status was impacted by a LC diagnosis, either because of interrupted employment due to sick leave/early retirement (n = 350, 35%) or because of reduced employment (n = 151, 15%) (Fig. 4b). At the country level, the employment status of participants in Japan seemed the least impacted, with 77% (n = 86) reporting no change. On the other hand, respondents living in China reported the highest change in their employment status (n = 67, 64%).
Patients with LC discussed the effects of the disease/treatments on their QoL mainly with their physician and family (Fig. 5). Globally, 70% of participants (n = 702) had a caregiver supporting them in daily life activities, most frequently a family member or relative (n = 610, 61%), whilst 7% (n = 66) did not have any help but would like to have some. The level of caregiver support reported was the highest among respondents living in China (n = 88, 85%) and the USA (n = 155, 74%), and the lowest in participants living in Japan (n = 63, 56%).
Fig. 5
Main persons/contacts with whom patients discuss quality of life. Multiple answers allowed, up to three choices. LC lung cancer, QoL quality of life. The following other people/contacts were selected by less than 10% of respondents: patient advocacy or support group, other patients with LC in person or on social networks, specialists from an independent telehealth service, social worker or counsellor, nurse, pharmacist, I have not discussed with anyone about QoL
Stigma during the LC pathway was experienced by 8% of participants (n = 77), mainly in the USA, France, and UK (12–14%), whereas no respondent living in China reported experiencing any stigma. A total of 84% (n = 841) of patients with LC never experienced stigmatization.
Information and ServicesInformation most desired by participants was about the type of LC, possible adverse effects of treatment, what to expect after being diagnosed, information on available/potential treatments, information on new treatments, and lifestyle advice (nutrition, physical activity, well-being) (Fig. 6a). A higher interest in ongoing research and new treatments was reported in China and Italy, with the lowest interest in Japan. Participants would have liked to receive this kind of information especially at diagnosis and for treatment decision-making.
For patients with LC, the main source of healthcare information was physicians (Fig. 6b). The next preferred sources of information were patient discussion forums on social media and family/friends. In China, 29% of participants ranked patient discussion forums on social media highly, and they additionally used other online information channels (patient blogs, pharma websites, etc.) more than in other countries.
Fig. 6

Main types of information sought by patients (a) and the services offered to patients since diagnosis (b). Multiple answers allowed. DHS digital healthcare solution.
Participants thought their opinion was sufficiently and equally considered by their physician regarding treatment options, administration preferences, and impact on QoL. Side effects was the topic about which participants would like to hear about the most.
Globally, the five main services offered to participants after LC diagnosis were psychological support, educational support, support from patient with cancer organizations (PO), support through a digital healthcare solution (DHS: like a mobile app, wearable device, or telehealth service), and financial support. From the patients who were offered support services, typically ~ 70% utilized them. Many patients who were not offered these services would have liked to receive them. Specific supportive services offered varied widely between countries. Canada had the highest level of support services offered, with each support service having between ~ 70% and 85% of participants reporting that they were offered. The UK had the lowest level of support services offered, with each support service having only 18–39% of participants reporting that they were offered.
When asked about DHS that would be most helpful for managing LC, participants would like DHS to track and help manage symptoms and side effects, to look up the drugs used to treat LC, and to help manage their diet, exercise, and well-being.
Patients with NSCLC and SCLCCompared to SCLC respondents, NSCLC respondents were older (26% over age 60 vs 18.75), had a longer time to diagnosis (2.7 years vs 2 years), and more likely to have never smoked (19.8% vs 11.5%). NSCLC respondents were more likely to report having no comorbidities (47% vs 30%) and reported lower rates of COPD and asthma (28% vs 35% and 22% vs 27%, respectively).
The experiences, preferences, and unmet needs of NSCLC and SCLC participants were mostly similar. There was a slightly higher rate of SCLC participants who expressed interest in wanting to know more about the adverse effects of treatments (40% vs 33%), and they were higher users across all support services than NSCLC participants (psychological, educational, etc.).
留言 (0)