
記住我





This study was performed in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Hospital of Chengdu University of Traditional Chinese Medicine (Date July 6, 2022/No. 2022KL-058-01). Written informed consent was obtained from all individual participants included in the study.
DesignThis multicenter, randomized controlled trial (RCT) has been carried out to clinically evaluate the efficacy of standardized tai chi in prefrail older adults with relevant conditions such as immunosenescence, balance ability, bioenergetic metabolism, and quality of life. A total of 144 eligible participants in this clinical trial with a parallel design were enrolled and randomized into four groups at a 1:1:1:1 ratio, and they underwent a 12-week intervention. The trial was planned to be conducted within three institutions in Sichuan Province, China, including the Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu Eighth People’s Hospital, and Hanyuan Traditional Chinese Medicine Hospital.
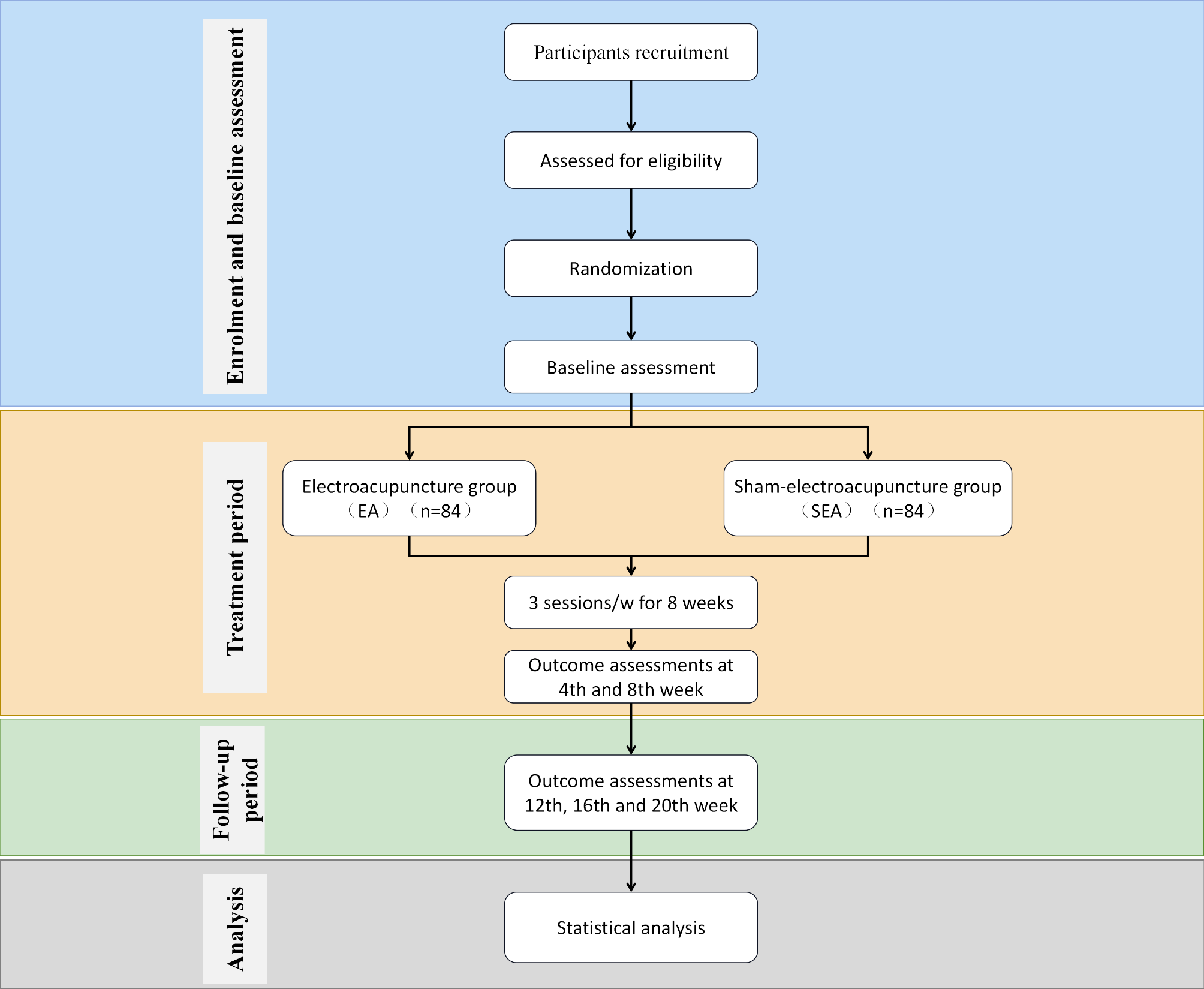
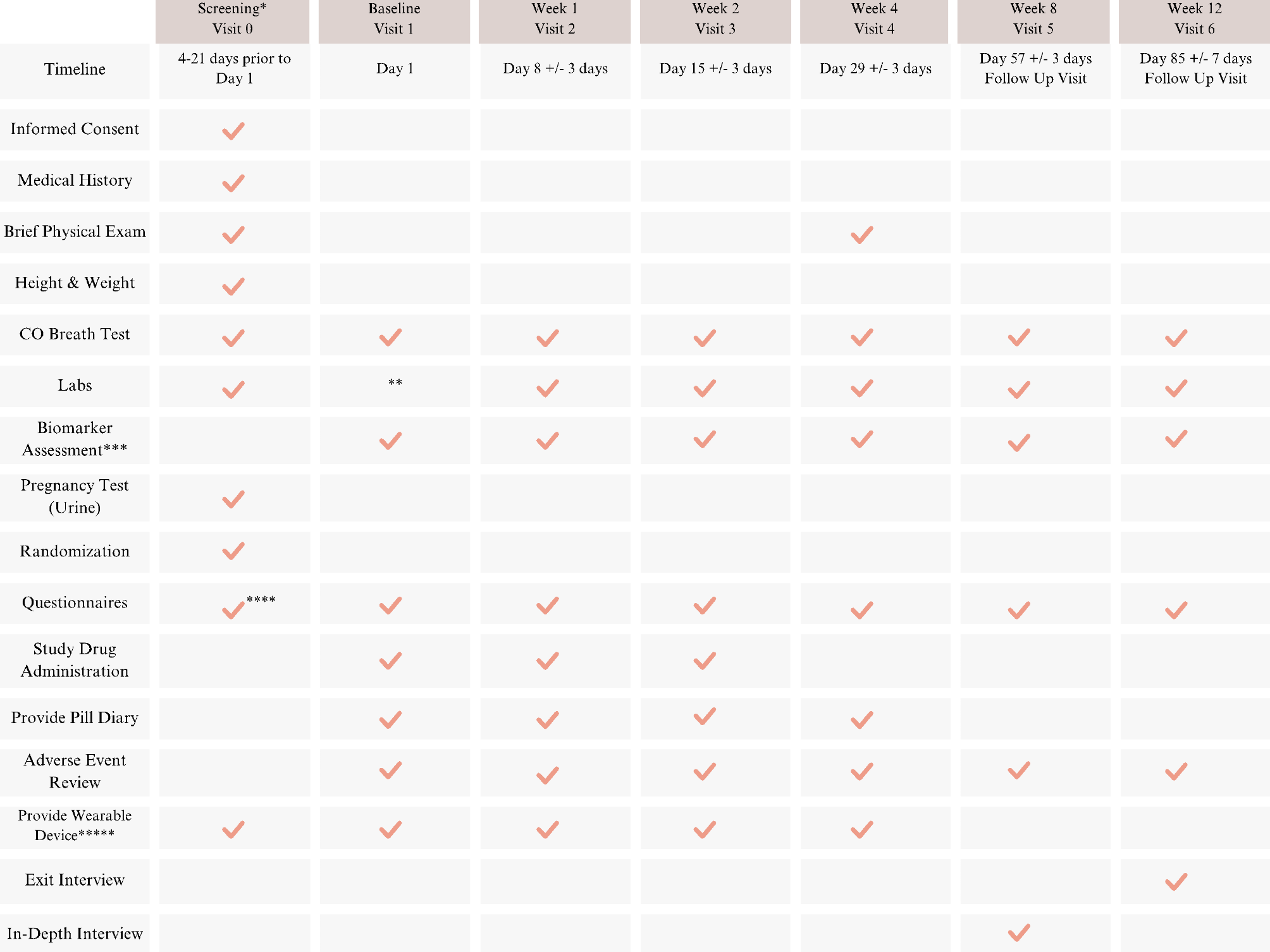
Along with the use of Fried’s frailty phenotype scale as a screening tool to recruit eligible participants, the participants were also analyzed using the frailty index, Berg balance scale, and sarcopenia quality of life (SarQoL) at randomization and 4, 8, and 12 weeks post-randomization. All the participants underwent 36 sessions of standardized tai chi training within 12 weeks, with each session lasting 60 min. The outcome measures used were indicators of sarcopenia, bioenergetic metabolism, immune risk profile, and the scales mentioned above at baseline as well as at 4, 8, and 12 weeks post-randomization (Table 1).
Table 1 Trial process chartA blinded design is not applicable to this study. Only the outcome assessment, data management, and statistical analysis personnel were blinded in this study, and the letters A, B, C, and D were used to replace the groups in the case report form (CRF). The protocols used in this study were approved by the ethics committee and local institutional review board. The present protocol (version 2.0, Jul. 15th, 2022) satisfied the Declaration of Helsinki and was conducted following CONSORT reporting guidelines [10]. Written informed consent was obtained from each participant before registration.
Inclusion/exclusion criteriaFried’s frailty phenotype scale was used for evaluating eligible participants at randomization (baseline phase). The Fried frailty phenotype includes weight loss without a known reason, fatigue, grip strength decline, slower walking speed, and poor physical performance. Patients meeting 1–2 standards were classified as prefrail, those meeting > 3 standards were classified as frail, and patients meeting no standards were classified as robust. Only prefrail patients were recruited for this clinical trial.
The candidates who met the following criteria were included in this study: (1) were between 60 and 75 years of age; (2) met 1–2 items on Fried’s frailty phenotype scale; (3) were able to walk independently without assistance, with a Berg scale score greater than 40; (4) were willing to participate in this study and could provide informed consent; and (5) did not perform physical activity more than once a week for the six months before the survey.
The exclusion criteria were as follows: (1) had moderate to severe osteoporosis and a history of fractures; (2) had severe musculoskeletal disorders affecting activity levels; (3) had serious heart, lung, liver, kidney, or other serious diseases; (4) had a severe psychological condition or mental illness history; (5) had hearing impairment and/or a visual impairment and were unable to cooperate with training; (6) were planning to participate in other training programs during the study period; (7) had metal implants (e.g., artificial pacemakers, joint replacement); and (8) had skin lesions limiting the use of bioelectrical impedance analysis (BIA).
Statistical analysisThe data were analyzed by a special reviewer who was blinded to patient grouping. The data were analyzed using the IBM SPSS Statistic 25.0 statistical software package.
This work deemed the intention-to-treat (ITT) population to be randomized cases. The basic features of the ITT population were examined. The primary and secondary outcomes were analyzed for the ITT population. Moreover, this study analyzed the per-protocol (PP) population and compared the results with those of ITT analysis to ensure consistency in the results. Missing data during ITT analysis were managed using the last observation carried forward method.
First, the basic features of the diverse groups were compared. The effects in the morning tai chi group were then compared with those in the control and resistance training groups. Furthermore, the effect in the morning tai chi group was compared with that in the afternoon tai chi group. For normally distributed data, repeated measures analysis was adopted for evaluation at diverse time points; to be specific, primary outcomes were evaluated at 4, 8, and 12 weeks post-randomization. Furthermore, generalized estimating equations (GEE) were used to analyze alterations with time. Numerical variables were analyzed by ANOVA, while categorical variables were analyzed by the chi-square test. A value of p < 0.05 (two-sided) was considered to indicate statistical significance.
Recruitment, randomization, and allocationPrior to the present trial, a power analysis was carried out, and the sample size in an interventional group was estimated to be 30 participants according to the formula. Considering the drop-out rate, 36 prefrail participants were necessary for each group. Therefore, a total sample size of 144 participants was included in this study. The participants in the present study were enrolled in the inpatient department and outpatient clinics of the three institutions mentioned in study desigh section by physicians. Participants were recruited using advertisements, referrals, etc. Recruitment materials were approved by the ethics review board, and informed consent was obtained from all participants. Potential participants underwent a screening process to ensure they met the eligibility criteria. Recruitment was scheduled to begin in Jan, 2024 and was planned to conclude by Dec, 2025. This timeline was estimated based on anticipated participant availability. All patients (from the outpatient clinic or inpatient department) met the inclusion criteria, but neither of the exclusion criteria, were randomized as a control or treatment group until each participant was grouped. Random assignment sequence specialized statistical analysts were commissioned to use the statistical software SPSS Statistics 25.0 (IBM, Chicago, IL, USA) to generate random numbers from 1 to 144. Eligible subjects were numbered according to their inclusion order and randomized into four groups at a 1:1:1:1 ratio as follows: (1) the control group (CG), (2) the morning tai chi group (MT), (3) the morning resistance training group (MR), and (4) the afternoon tai chi group (AT). One independent research assistant who was blinded to subject enrollment, assessment, and tutoring was responsible for maintaining the allocation sequence. The random allocation sequence was concealed in an opaque envelope.
InterventionPrior to the intervention, all the older adults received health education regarding frailty, including its risk factors, prevention interventions, and poor prognosis. All subjects also received dietary guidance, including nutrition, a balanced diet, a healthy lifestyle, and eating habits, based on the Dietary Guidelines for older adults in China revised by the Chinese Nutrition Society in 2022. The treatment groups were to have different physical exercise regimens at different times (in the morning or the afternoon), while the control group received only health education without any regular physical exercise. The subjects in the treatment groups performed physical exercise thrice weekly for 12 consecutive weeks. Each exercise session lasted for 40 min in total, including 10 min of warm-up exercise, followed by 25 min of standardized tai chi and 5 min of cool-down exercise. All the exercises were performed under the supervision of professional tutors to ensure the safety of the subjects and the accuracy of every movement. The morning and afternoon tai chi groups were assigned to perform standardized tai chi in the morning or afternoon, respectively, while the morning resistance training group was assigned to perform resistance exercise in the morning.
Standardized tai chi is a simplified version for beginners and was promoted by the Atrial Art Administration Center of the General Administration of Sport of China to publicize and popularize tai chi. Based on the existing schools of tai chi, the General Bureau of Atrial Art Physical Education started with core techniques involving eight kinds of arm movements and five kinds of steps. The whole set of movements is simple in structure, mild in intensity, and easy to learn and practice.
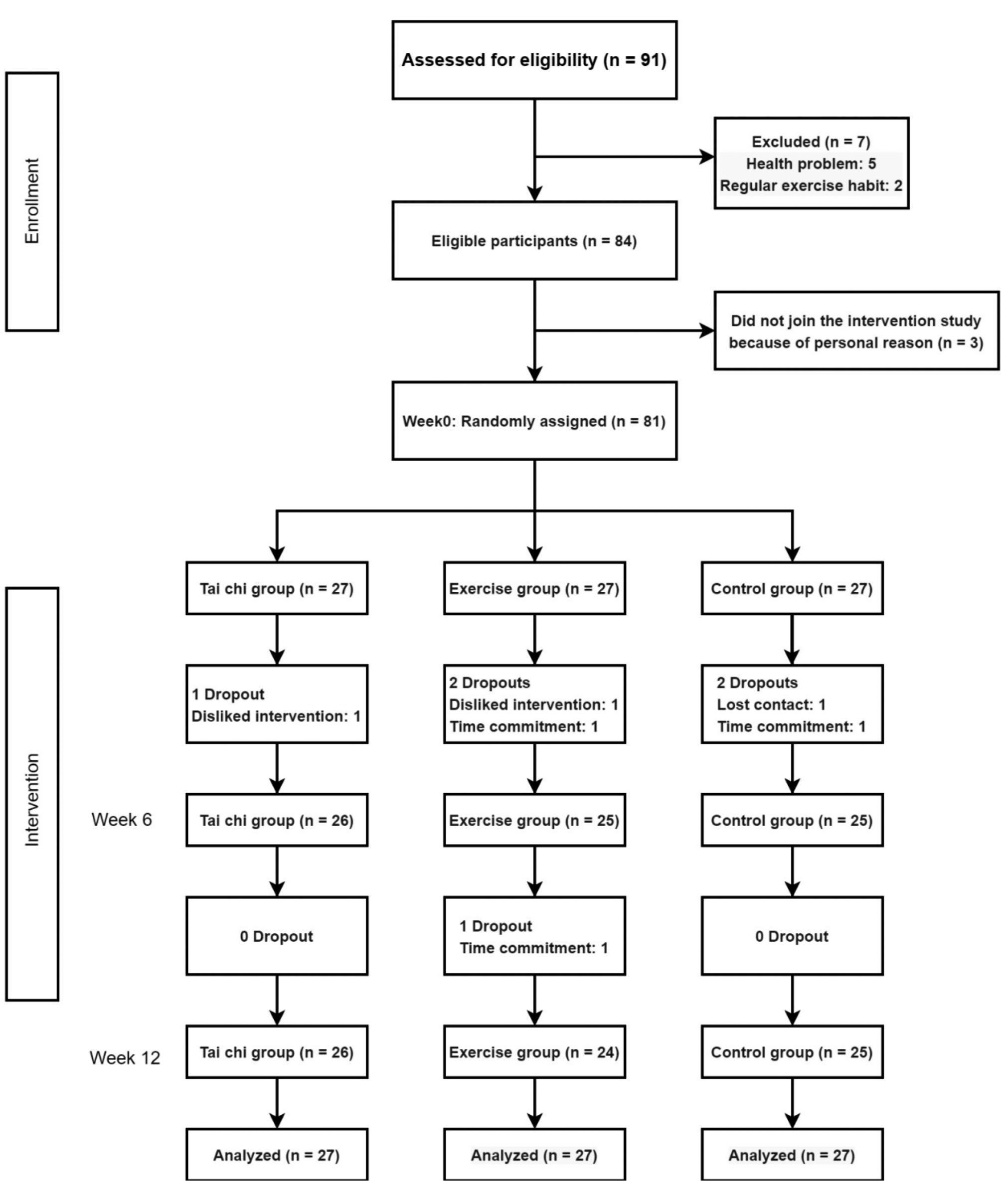
In the resistance training group, weight lifting was used to train the skeletal muscles of the upper limbs, and a resistance band was used to train the skeletal muscles of the lower limbs (Fig. 1).
Fig. 1
Flow chart of the trial. A total of 144 prefrail participants were included in this study and were randomized (1:1:1:1) to four groups: (1) a control group with only health education; (2) a morning tai chi group; (3) a morning resistance training group; and (4) an afternoon tai chi group
Evaluation during the intervention periodDaily activities during the intervention period were recorded and evaluated. To exclude the impact of daily physical activity on the exercise intervention, all subjects completed the daily activity table at 4, 8, and 12 weeks after randomization, and the average daily activity and duration in the past week were recorded. The types of daily activities included sleep, static work, low-, medium-, and high-intensity activities, and activity profiles were collected by telephone follow-up.
Exercise intensity was assessed using the percentage maximum heart rate. The heart rate was monitored during the whole exercise process using a Mio Alpha II heart rate monitor (USA). The average heart rate output after the exercise was the measured heart rate of the exercise. The same subject was evaluated three times to obtain the mean value. The calculation equation is as follows: maximum heart rate % = (measured heart rate/(220- age)) ×100%.
Sports attendance was also recorded and evaluated. The rate of sports attendance was checked by the intervention supervisor at each training session. Those who participated in training for < 20 min each time were deemed to be absent. Following the intervention, the sports attendance rate was recorded. The sports attendance rate was calculated using the following equation: Attendance %= (training session number/total planned session number) ×100%.
Outcome measuresPrimary endpointsPrimary outcomes in this trial included the frailty index, physical performance, muscle strength, and muscle mass. The frailty index (FI) was assessed before randomization (baseline phase) as well as at 4, 8, and 12 weeks post-randomization. FI, obtained from the theory of deficit accumulation evaluation, is rated according to the potential unhealthy measures of an individual as a percentage of all measures at a given point in time.
Moreover, physical performance, mass strength, and muscle mass were also evaluated as primary outcomes. Muscle mass was determined using bioimpedance analysis (BIA) (DBA-510). Hand grip strength is determined by a dynamometer (JAMAR). The subjects stood with their upper arms close to the torso. The primary outcomes of this trial included bending of the elbows at 90°, deviation of the forearms from the ulchi at 0–15°, and extension of the wrists at 0–30°. The strength of both upper limbs was measured twice, and the maximum value was taken, with one decimal point reserved for the reading.
Physical performance was assessed with three indicators: short physical performance battery (SPPB), timed up and go (TUG), and the 6-minute walk test. The SPPB is a mature tool for monitoring the physical function of older adults. There were three assessments: standing on the feet in three different positions for 10 s, measuring the walking speed within 3–4 m, and getting up from a chair five times. The 6-minute walking test is a simple way to assess physical capacity by asking patients to walk for 6 min and recording the longest distance they walk. It is necessary to guide subjects to walk in a straight line without speeding up or slowing down. The TUG test is a rapid quantitative assessment of functional walking ability. The subjects sat in an armchair with a backrest. A ribbon, a thick visible line or a visible marker is placed on the floor 3 m away from the seat. When the investigator says “go,” the patient needs to stand up from the reclining chair, step forward 3 m as one would normally walk, cross the line or marker, turn around, walk back to the chair, turn around, and sit back. No physical assistance was provided during the test. The investigator records the time (in seconds) taken by the patient’s back to leave the chair and sit back again.
Secondary outcomeThe secondary outcomes in this trial included the bioenergetic anti-stress index (BASI), immune risk profile (IRP), Berg balance scale score, and Sar QoL.
To date, there are no definite biomarkers for assessing frailty. Mitochondrial metabolism and stress are closely related to aging and the health of older adults. The BASI is used as a biomarker of frailty and measures the level of mitochondrial respiratory function in peripheral blood cells to determine the baseline bioenergetics of participants to assess their quality of life.
While immunosenescence is a potential therapeutic target for treating frailty, the IRP is a well-recognized indicator of immune function in older adults. Therefore, blood samples were obtained from all participants, and the presence of immune cells in the peripheral blood circulation was determined by flow cytometry. The cell count and function of induced T cells/helper T cells (CD4+), inhibitory T cells/cytotoxic T cells (CD8+), and the CD4/CD8 ratio were also assessed. Enzyme-linked immunosorbent assay (ELISA) was used to detect the presence of the circulating inflammatory factor interleukin 6 (IL-6)/tumor necrosis factor-α (TNF-α).
Each participant was analyzed using the Sar QoL scale and Berg balance scale at randomization (baseline phase) as well as at 4, 8, and 12 weeks post-randomization. The Sar QoL scale reflects symptoms such as loss of muscle mass or strength caused by aging and muscle wasting diseases and reflects the effect of muscular health on daily life. The berg balance scale is a comprehensive scale for assessing body balance function. The balance function is divided into 14 items from easy to difficult, and each item is divided into 5 levels, namely, 0 (lowest)-4 (highest), yielding total scores of 0–56.
One independent outcome assessor with no knowledge of patient grouping was responsible for the assessment at each institution to ensure outcome creditability. To avoid inter-assessor bias, assessors needed to complete the assessment of each patient before and after randomization. Moreover, the experts responsible for the statistical data analyses were blinded to the groups.
Demographic collection and safety measurementsUpon enrollment, demographic data (including age, gender, race/ethnicity, education, and living arrangements), vital signs, medical conditions, alcohol/smoking fall-related data (falls and admission times within the past year), and physical activity of patients were extracted from the CRF. Before randomization, the participants underwent routine tests for urine, blood, electrocardiogram, random blood glucose, kidney function (BUN, Crea), and liver function (ALT, AST) to exclude those suffering from severe disorders of the liver, heart, or kidney.
Every adverse event was recorded carefully, managed appropriately, and followed up until proper resolution or stabilization. Unexpected events and serious adverse events (SAE), such as falls and muscular or joint pain, were reported to the Ethics Committee and competent authorities as needed.
In addition, all investigators require adequate training to ensure their understanding of the clinical trial in detail. The training included understanding the background, aim, and protocol of the trial, physical exercise intervention and quality control measures. For instance, each recruiter should be familiar with the inclusion/exclusion criteria of the study, the central randomization process, and the standard operation methods of various screening scales and tests. Outcome assessors should master the standard operation methods for each outcome measure. After the evaluation, all the real data on the CRF were recorded, signed, and recorded. The same evaluation was performed by the same assessor before and after the intervention. During the intervention, tai chi coaches were required to conduct unified and standardized movements, guide the subjects to practice throughout the whole process, and correct non-standard movements as needed. The researchers supervised every training session and made on-site sign-ups, and the rate of attendance was counted after the intervention. Those unable to attend the intensive practice were required to ask for leave in advance, and it was recorded to ensure that they received 40 min of exercise thrice a week.
To ensure quality control, one specific quality examination form was prepared to check the trial procedure and document the detailed process twice a month at each institution. In addition, inspectors audited the research at 3-month intervals at each institution. Follow-up was conducted via on-site clinical consultation or telephone or mobile calls. Any withdrawal or drop-out is well documented during the intervention and follow-up periods. Research assistants should determine the real reasons for subjects withdrawing from clinical studies and provide health education on basic therapies to improve and reverse prefrailty after withdrawal. If serious safety issues occur, the clinical trial will be suspended. Follow-up with subjects is necessary to ensure their safety. The trial will be terminated if the ethics committee considers that the safety of the subjects is unable to be effectively ensured.
留言 (0)