
記住我




This study is a single-center, randomized controlled trial. Voluntary patients who meet the inclusion criteria will be openly recruited at West China Hospital of Sichuan University. All patients must understand and sign an informed consent form before enrollment. Each center will strictly follow the diagnostic criteria, inclusion criteria, and exclusion criteria to screen cases. After confirming enrollment, a random number will be obtained by applying the random code process until the total number of observed cases is completed, ending the trial.
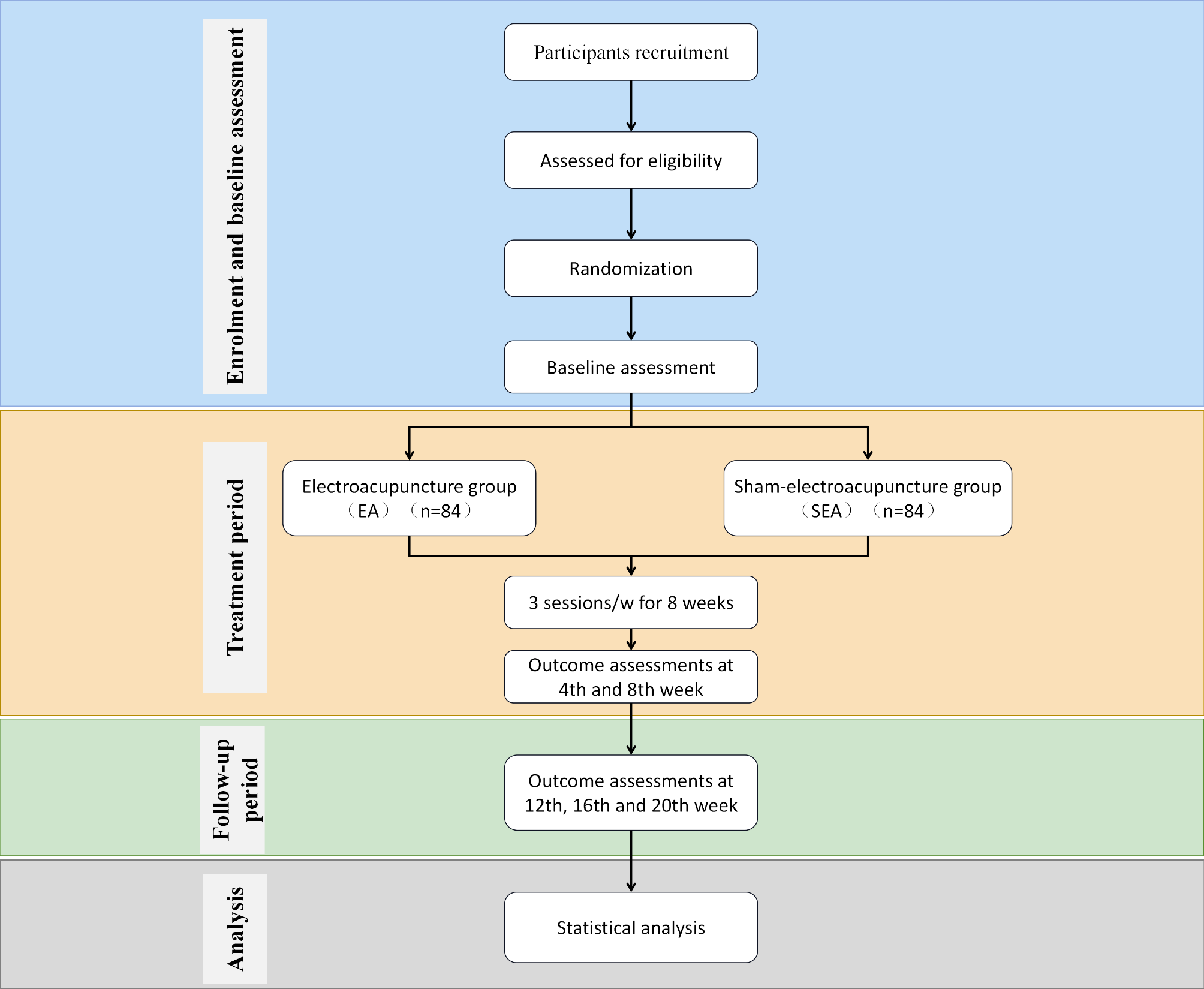
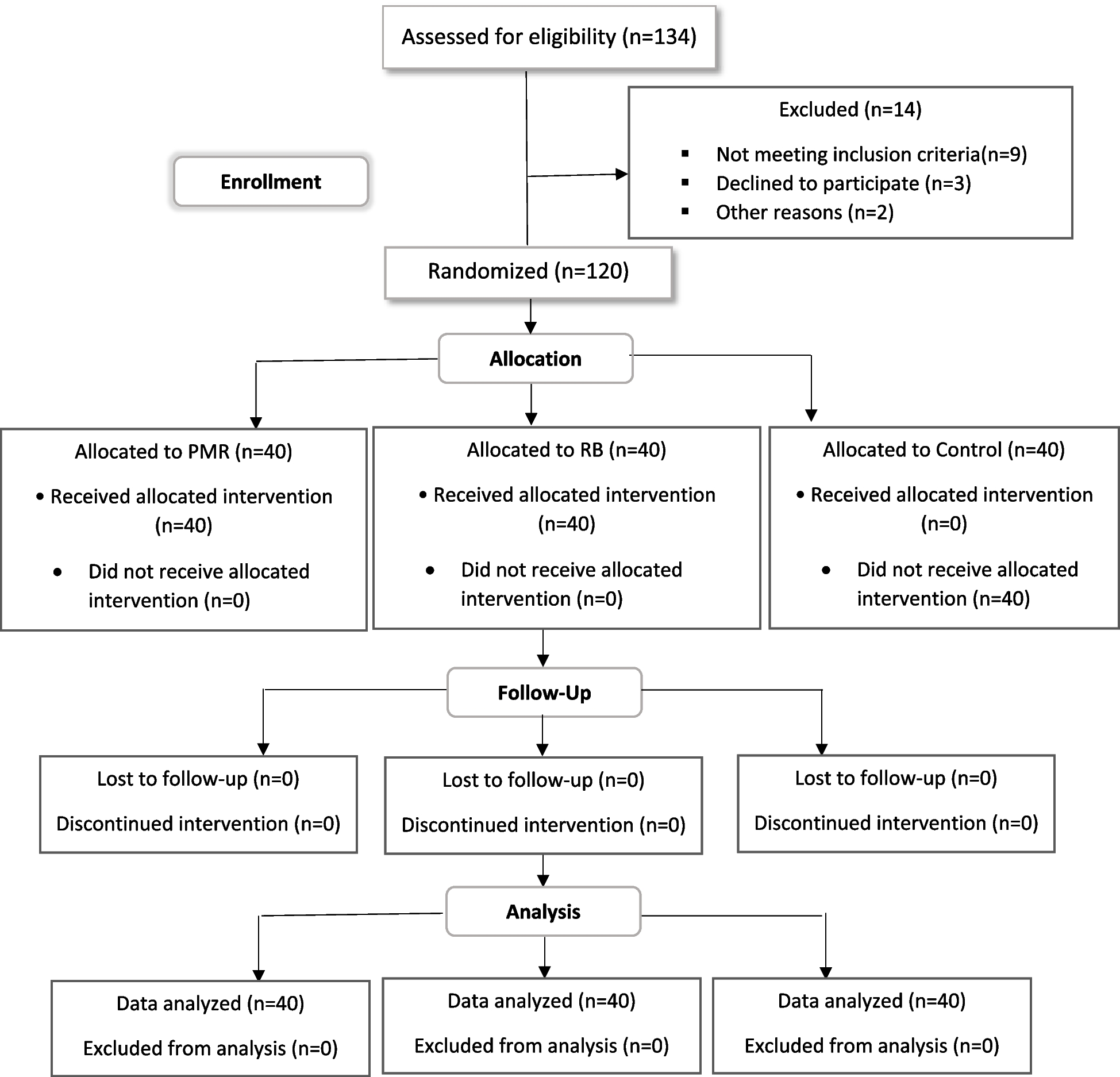
RecruitmentThis trial will be conducted at West China Hospital of Sichuan University. The diagnostic criteria for muscular dystrophy will follow the “2019 Asian Consensus on Muscular Dystrophy Diagnosis.” When patients visit the hospital, they will first be provided with informed consent, followed by an evaluation of their condition by professional researchers and completion of a preliminary screening form. Patients who pass the preliminary screening will undergo baseline evaluations and relevant examinations for further selection. Patients who meet the inclusion criteria will be further confirmed for the feasibility of being randomly assigned to either the acupuncture group or the standard treatment group. Figure 1 illustrates the study flowchart.
Fig. 1
Flow chart of the study procedure
Diagnostic criteriaThe diagnosis of sarcopenia is based on the “2019 Asian Sarcopenia Diagnosis Consensus” published by the Asian Working Group for Sarcopenia (AWGS). A diagnosis can be made if both points (1) and (2) or points (1) and (3) are met, or if all three points are met:
(1) Reduced muscle mass: bioelectrical impedance analysis (BIA) with a male ASMI < 7.0 kg/m2 and a female ASMI < 5.7 kg/m2; (2) Decreased muscle strength: male grip strength < 28 kg, female grip strength < 18 kg; (3) Decreased muscle function: Short Physical Performance Battery (SPPB) score ≤ 9.
Inclusion criteria(1) Meets the diagnostic criteria for “sarcopenia” as outlined in the “2019 Asian Sarcopenia Diagnosis Consensus” published by the Asian Working Group for Sarcopenia; (2) Age between 60 and 80 years old, no gender restrictions; (3) Signs the informed consent form and voluntarily participates in this trial.
Exclusion criteria(1) Suffering from severe kidney disease (glomerular filtration rate < 30 mL/min); (2) Suffering from moderate to severe liver function failure (Child-Pugh Class B or C); (3) Suffering from endocrine diseases related to calcium metabolism disorders (excluding osteoporosis); (4) Suffering from neuromuscular diseases; (5) Taking medications that have a significant impact on musculoskeletal function; (6) Suffering from mental illness, cancer (within the past 5 years); (7) Individuals with drug or alcohol dependence or abuse; (8) Patients participating in other clinical trials.
Withdrawal criteria(1) Specialist physicians are responsible for assessing serious adverse reactions that occur during the study, determining whether to continue or terminate the study; (2) During the study, if symptoms worsen or severe complications or other serious diseases occur that require emergency measures; (3) Researchers discover serious safety issues; (4) Patients who cannot continue treatment for various reasons; (5) The trial participant withdraws informed consent.
Randomization and maskingThis study has a single-blind design. Participants will be unaware of their group allocation, which will only be known to the lead investigator and acupuncture physician. The participants are randomly assigned to EA group and sEA group at a 1:1 ratio. The random sequence will be generated and masked by an online response system maintained by the statisticians. Randomization is stratified by site and defined with a block size of 6. All relevant parameters set during the randomization process are saved in the blinding information. When a qualified participant is enrolled, the person responsible for randomization or clinical researchers will apply for a random number using the central randomization system.
InterventionElectroacupuncture (EA) group1) Main Acupoints: Binao (LI14), Quchi (LI11), Shousanli (LI10), Hegu (LI4), Futu (ST32), Liangqiu (ST34), Zusanli (ST36), and Jiexi (ST41).
2) Procedure: Routine disinfection of acupoints. The Hegu (LI4) Point is located on the back of the hand, at the midpoint of the second metacarpal bone on the radial side. Insert a 0.30 mm×25 mm filiform needle obliquely to a depth of 0.5-1 cun. The Shousanli (LI10) Point is located on the forearm, 2 cun below the transverse crease of the elbow. Insert a 0.30 mm×40 mm filiform needle vertically to a depth of 1-1.5 cun. The Quchi (LI11) Point is located at the elbow, at the midpoint of the line connecting the cubital fossa and the external epicondyle of the humerus. Insert a 0.30 mm×40 mm filiform needle vertically to a depth of 1-1.5 cun. The Binao (LI14) Point is located 7 cun above the elbow, on the anterior edge of the deltoid muscle. Insert a 0.30 mm×40 mm filiform needle vertically to a depth of 1-1.5 cun. The Futu (ST32) Point is located in the anterior thigh area, 6 cun above the bottom of the patella, on the line connecting the anterior superior iliac spine and the lateral edge of the patella. Insert a 0.3 mm×50 mm filiform needle vertically to a depth of 1–2 cun. The Liangqiu (ST34) Point is located in the anterior thigh area, 2 cun above the bottom of the patella, between the vastus lateralis muscle and the rectus femoris tendon. Insert a 0.30 mm×40 mm filiform needle vertically to a depth of 1-1.5 cun. The Zusanli (ST36) Point is located on the outer side of the lower leg, 3 cun below the outer knee point, Insert a 0.3 mm×50 mm filiform needle vertically to a depth of 1–2 cun. The Jiexi (ST41) Point is located in the ankle area, in the central depression in front of the ankle joint, between the long extensor tendon of the big toe and the long extensor tendon of the toes. Insert a 0.30 mm×25 mm filiform needle vertically to a depth of 0.5-1 cun. Immediately after needling, perform vigorous lifting, thrusting, and twisting techniques. Followed by electroacupuncture stimulation, with one set of electroacupuncture connected to the same side’s Quchi (LI11) Point and Hegu (LI4) Point, and another set connected to the same side’s Futu (ST32) Point and Zusanli (ST36) Point. A total of 4 sets of electroacupuncture, with a continuous frequency of 2 Hz and each electroacupuncture stimulation lasting for 30 min. After enrollment, treatment is conducted 3 times per week for 8 weeks.
Sham electroacupuncture(sEA) group1) Main Acupoint: Same acupoint as the EA Group.
2) Procedure: The Park sham placebo acupuncture device (PSD) is used for the procedure. The PSD is a dull-tipped retractable needle. The acupuncturist inserts the needle into the cannula, and once the blunt tip contacts the skin, the needle retracts into the handle, without penetrating the skin. After the needle insertion is completed, the device is connected to a placebo electroacupuncture device that only has a flashing current indicator light but no actual current output, following the same connection method as the EA group.
Observation Period: A total of 21 weeks, including a 1-week baseline period, an 8-week treatment period, and a 12-week follow-up period.
The selected acupoints and their locations are shown in Fig. 2.
Fig. 2
Localisation of acupoints
Outcome measuresPrimary outcomePatient’s grip strength (GS) change after 8 weeks of treatment: Grip strength of the dominant hand was measured using a dynamometer at both baseline and the end of the 8-week treatment period. Three measurements were taken with a 5-minute rest interval between each measurement. The average of the three measurements was calculated. The grip strength change rate was then calculated using the following formula: Grip Strength Change Rate = (Post-treatment Grip Strength-Pre-treatment Grip Strength)/Pre-treatment Grip Strength × 100%.
Secondary outcomes1) Patient’s grip strength change rate at week 4 and week 20: Grip strength of the dominant hand was measured using a dynamometer at week 4 and week 20. Three measurements were taken with a 5-minute rest interval between each measurement. The average of the three measurements was calculated. The grip strength change rate was then calculated by comparing it to the baseline grip strength.
2) Appendicular Skeletal Muscle Index (ASMI) change rate: Patient’s body composition analysis was conducted using the Inbody bioelectrical impedance analysis device (BioSpace, Seoul, Korea). The commonly used SMI was used for evaluation. The SMI change rate was calculated using the following formula: SMI Change Rate = (Post-treatment SMI - Pre-treatment SMI) / Pre-treatment SMI × 100%.
3) Muscle Function Evaluation: The Short Physical Performance Battery (SPPB) was used to evaluate the muscle function of the patients.
4) Daily Function Assessment: The International Physical Activity Questionnaire (IPAQ) will be used for the assessment of It mainly evaluates the frequency and duration of common activities in the past week. Based on the metabolic equivalent tasks (METs) of each activity, weekly energy expenditure is calculated to assess the patient’s daily activity level.
5) Subjective Assessment of Treatment Efficacy by Patients: ① Using a Visual Analog Scale (VAS), please rate your subjective perception of the effectiveness of electroacupuncture. A score of 0 indicates no improvement, while a score of 10 indicates complete improvement. ② Ask patients to evaluate whether electroacupuncture is helpful in treating muscle atrophy using a 7-point scale.
6)Serum inflammatory factor levels: Blood samples were collected from patients to measure CRP, IL-6, and TNF-α levels.
7) Expectation Evaluation of Electroacupuncture and Its Correlation with Primary Outcome Measures: ① Do you believe that electroacupuncture treatment will be effective for your condition? Yes, no, unsure. ② Do you think electroacupuncture will be helpful in improving symptoms such as muscle weakness? Yes, no, unsure. ③ Using a Visual Analog Scale (VAS), please rate your expectation of the effectiveness of electroacupuncture. A score of 0 indicates no improvement, while a score of 10 indicates complete improvement.
8) Evaluation of Electroacupuncture Blinding: Inform the patients about two treatment methods, one being electroacupuncture and the other being placebo electroacupuncture. Then ask the patients to choose: Do you think you received electroacupuncture treatment? Don’t know, yes, no. Simultaneously evaluate the effectiveness of electroacupuncture blinding and its correlation with the patients’ experience with electroacupuncture.
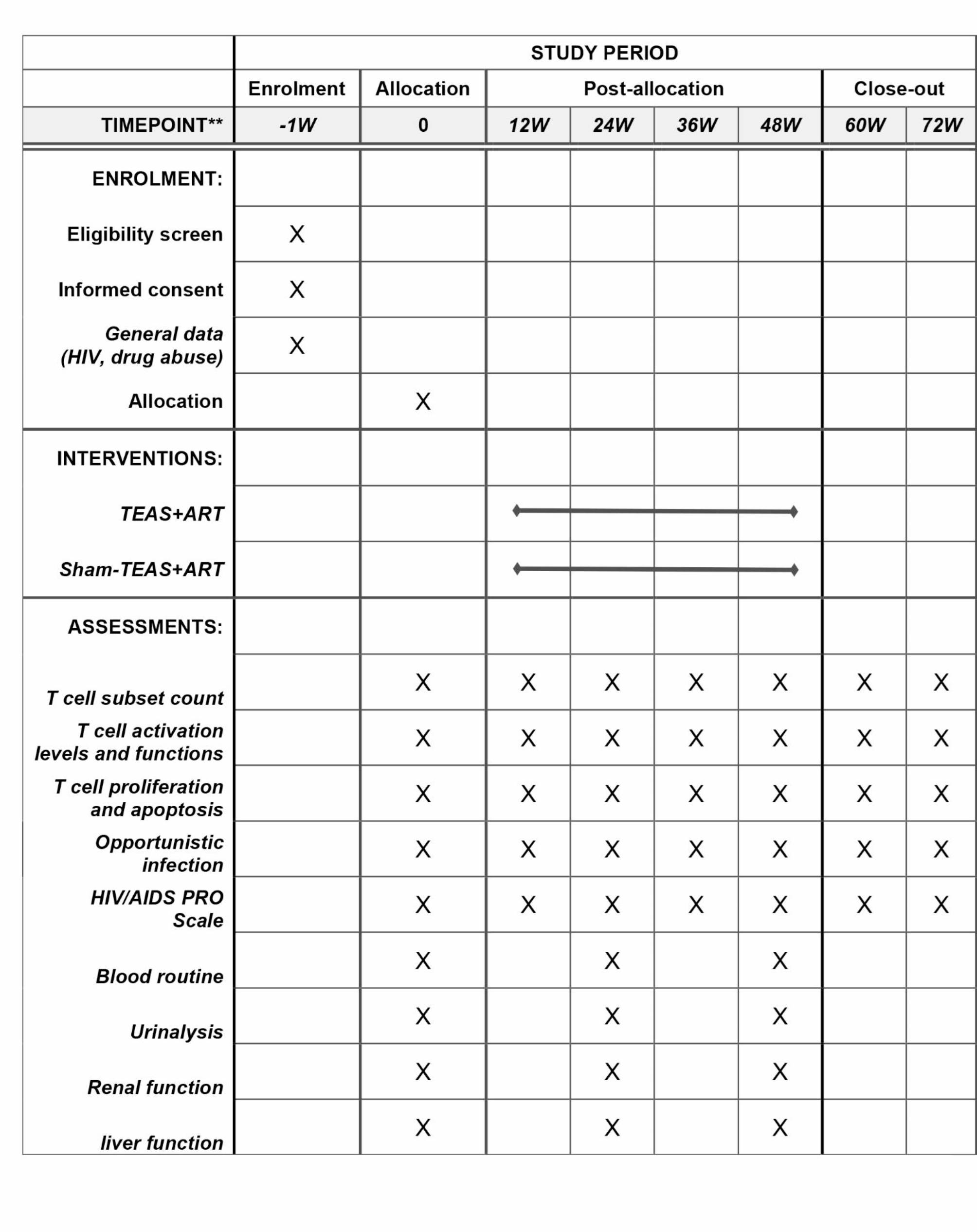
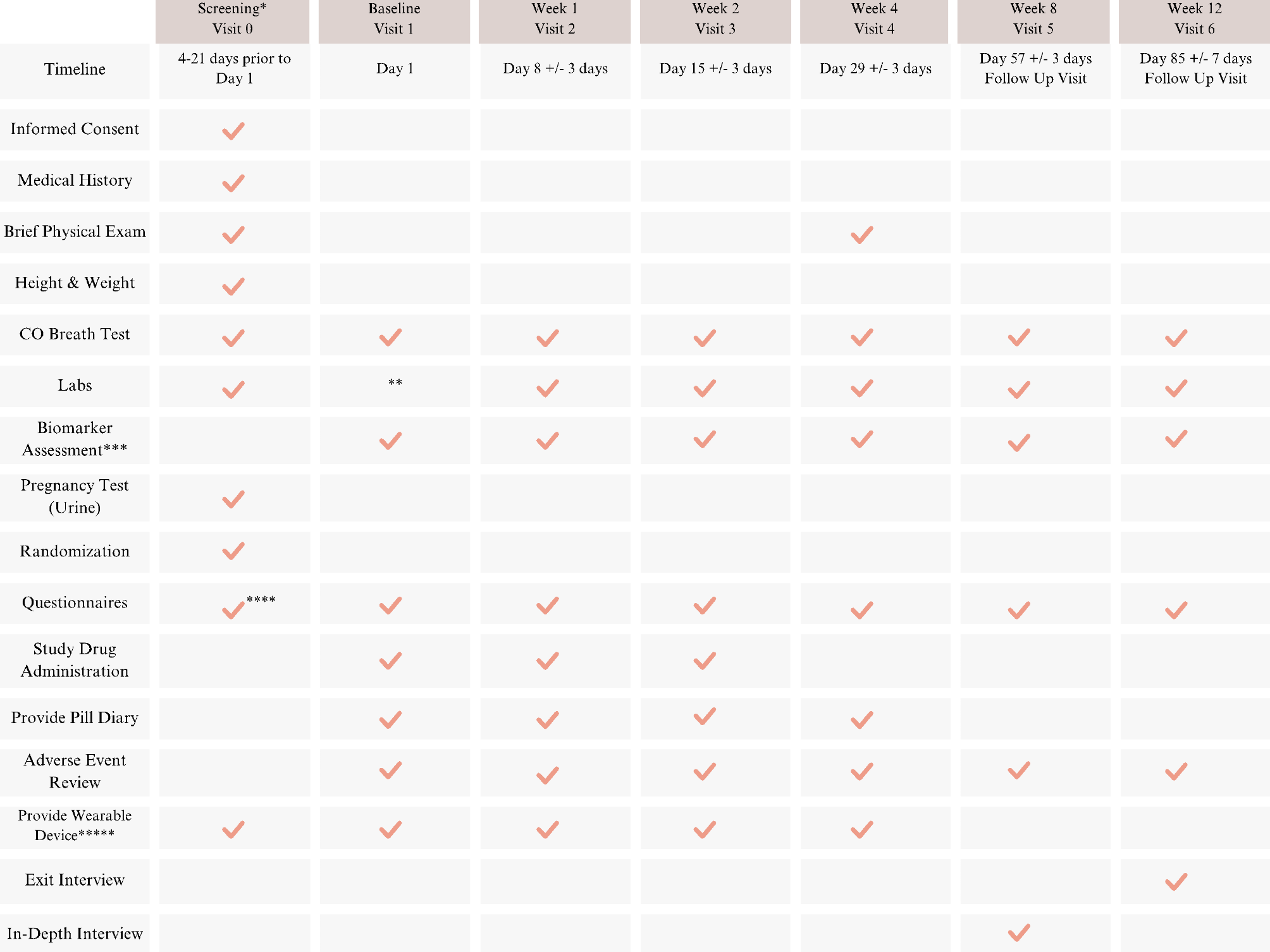
The outcome measurement time points are provided in detail in Table 1.
Table 1 Details of the planned visit scheduleSafety evaluationEA-related safety evaluation during treatment includes the documentation of broken needles, fainting due to needles, intolerable pinprick pain, local hematoma, infection, abscess, and other incidences of discomfort after pinprick. Adverse events will be recorded by the acupuncture physician on a standardized form.
Sample sizeBased on the results of previous similar studies (Soares Mendes Damasceno G, et al. Acupuncture Treatment in Elderly People with Sarcopenia: Effects on the Strength and Inflammatory Mediators. J Aging Res. 2019 Jan 27;2019:8483576), we used a two-sided test of difference and calculated the sample size using PASS 15 software. The average grip strength for the acupuncture group was 24.4 with a standard deviation of 8.59, while the control group had an average grip strength of 21.5 with a standard deviation of 4.51. With α = 0.05, β = 0.2, and Power = 0.8, each group required 70 participants. Considering a 20% dropout rate causing sample size loss, each group needed 84 participants, totaling 168 participants required for the study.
Statistical analysisThe data will be analyzed by R software (R Foundation), version 4.2.1. An independent statistician who does not know the group assignments will run the statistical analysis. Continuous variables will be described as mean ± SD with a 95% CI in a normal distribution and median (range) in abnormal distribution, while categorical variables will be represented by numbers (percentages). All statistical tests will be two-sided, and a p value < 0.05 will be considered statistically significant.
All analyses will be performed according to intention-to-treat (ITT) protocol. Participants who finish the baseline assessment of primary outcome and receive at least one session of either EA or sEA will be included in the ITT analysis. The missing values will be imputed by multiple imputations. Per-protocol population analysis will be also performed, for participants who have finished at least 80% of the treatment protocol after randomization.
The primary analysis used a linear regression model to test whether acupuncture improved GS more than sham acupuncture. Secondary analyses were done for other outcomes. Continuous data (SMI, SPPB, IPAQ scores, serum inflammatory factor levels; and patient subjective evaluation of efficacy) were analyzed using the same linear regression model. Categorical and count datawill be compared by the χ2 test or Fisher’s exact test.
留言 (0)