This study employed a three-arm, double-blind RCT design. The trial was registered at http://www.umin.ac.jp/ctr/index.htm (ID no. UMIN000042051, first posted October 8, 2019) and was preceded by a pilot intervention phase. It was conducted at the cognitive impairment unit of a nursing home in Hainan province, China, between December 2020 and July 2021.
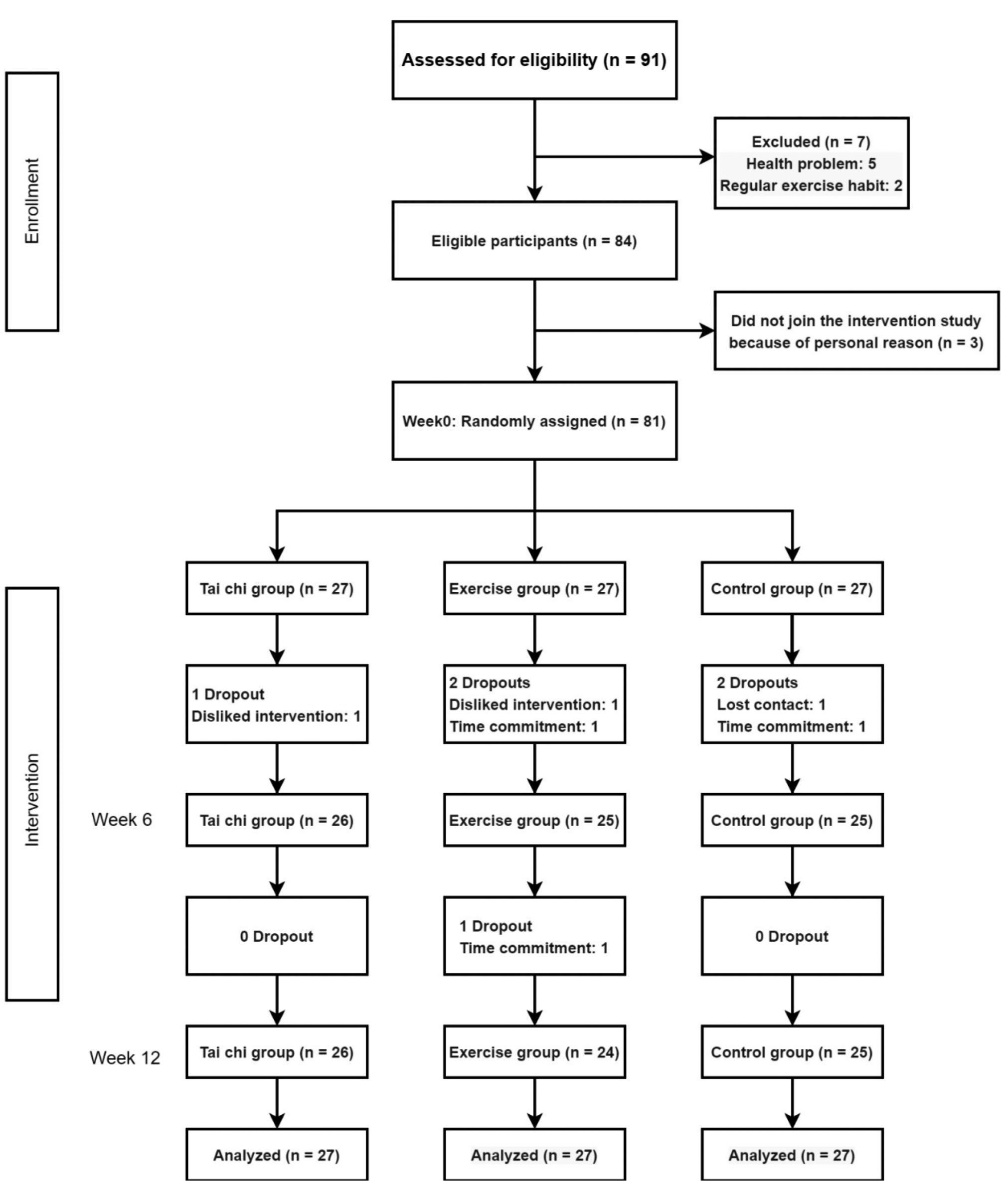
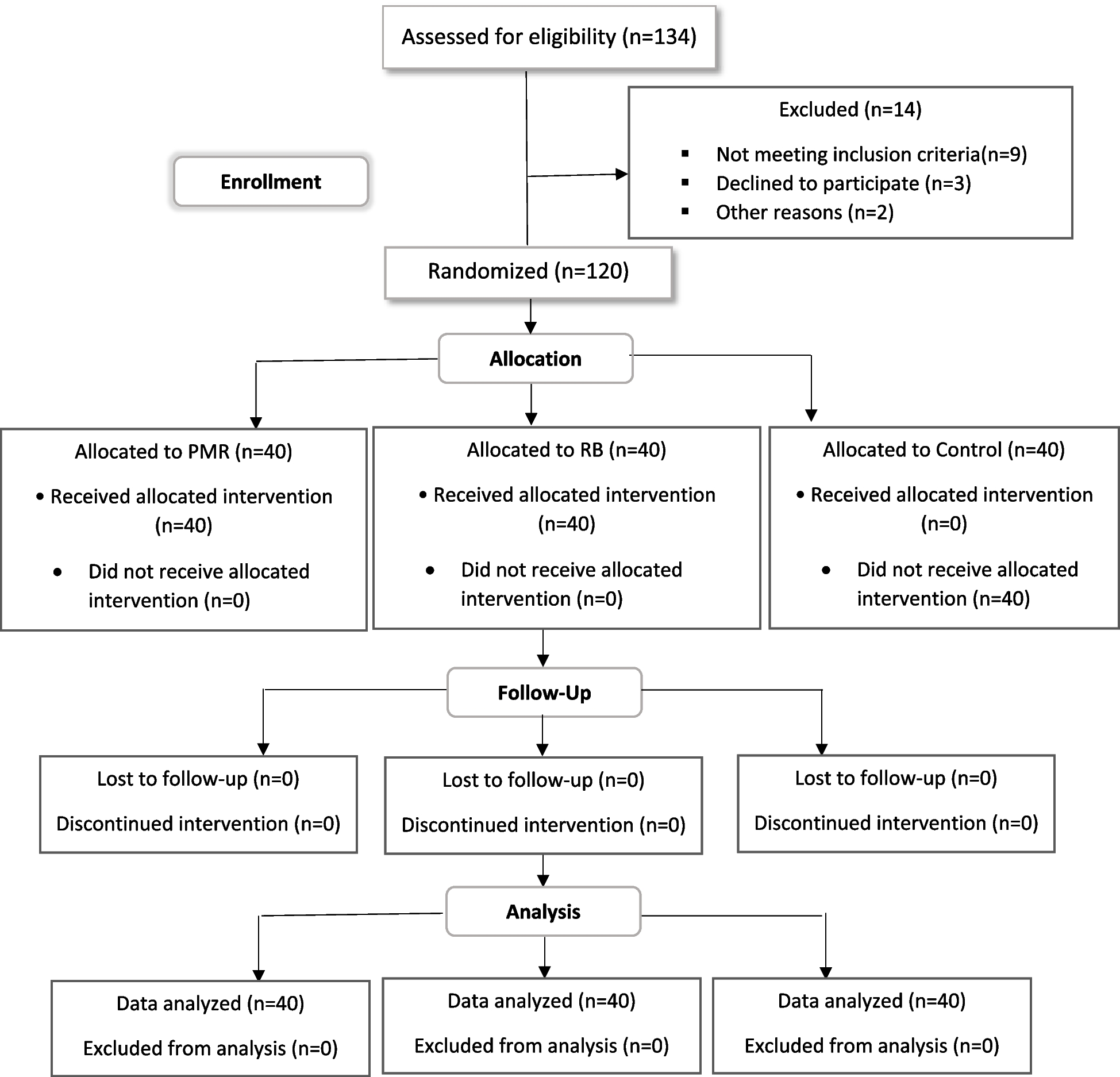
After screening and collecting baseline data, participants who met the inclusion criteria were assigned numbers from 1 to 81, and a random number table was produced by random number generation software. A block-randomization distribution was adopted to ensure that the number of participants in each group was equal and to control for potential confounders. An independent researcher who was not involved in the study placed the random computer-generated numbers into opaque, sealed envelopes according to the chronological order of the participants’ recruitment. The two interventions were conducted on different days of the week to prevent the participants from knowing other participants’ group assignments or comparing themselves with participants in other groups. The professional instructors and research assistants were informed about the study protocols before the interventions. Research assistants involved in the collection of post-test data were blinded to the group assignments.
Participants
Potential participants were recruited from the cognitive impairment unit of a nursing home in Hainan province, China. The inclusion criteria were as follows: (a) age of ≥ 65 years; (b) the ability to speak and understand Chinese; (c) a confirmed diagnosis of cognitive impairment and a score of 10–23 points on the mini-mental state examination (MMSE, a test widely used to diagnose cognitive impairment; <10 points indicates severe cognitive impairment and > 24 points indicates no cognitive impairment [16]); (d) the ability to see the body movement demonstrations clearly and hear the coach’s instructions clearly (both of which were tested before the intervention); (e) a physical condition that allowed the completion of the prescribed exercise plan (as assessed before the intervention); (f) stable condition and medication doses for at least 30 days before the intervention; and (g) agreement to participate in the study and sign the informed consent form. The exclusion criteria were as follows: (a) a diagnosis of severe illness or pain that would prevent full participation in the exercise interventions (e.g., metastatic cancer or musculoskeletal disorders) and (b) regular exercise over the past year (≥ 30 min, 3 times per week for over 3 months).
Intervention
A pilot study was conducted before the formal intervention to ensure the safety and feasibility of our protocol. Six potential participants were randomly selected and allocated to a tai chi (TC) group, a conventional exercise (CE) group, and a waitlist control group with no intervention, and the pilot interventions were implemented for 1 week. The feedback obtained from participants was discussed with the research team and a conventional exercise physiotherapist to modify the program. After conducting the pilot study and finalizing the intervention programs, participants in the TC and CE intervention groups attended three 50-minute intervention sessions per week for 12 weeks. The sessions were guided by a physiotherapist with more than 5 years of teaching experience and appropriate qualifications. All physical therapists held a national advanced tai chi coach certificate. Research assistants monitored participants during the intervention sessions to ensure their safety.
Previous research has shown that eight-form tai chi is easy to learn and suitable for patients with mild to moderate cognitive impairment [16, 17]. Accordingly, we selected the eight-form tai chi method created by China’s Physical General Office. The training was performed on Mondays, Wednesdays, and Fridays, and the details of the intervention are summarized in Table 1. Each session included a warm-up and cool-down, and the participants were instructed to slowly stretch at a comfortable intensity rather than forcing themselves to perform the movements. They were also advised to focus on their lower body while fully extending their upper body.
The conventional exercise intervention was based on relevant literature and was developed through consultation with an exercise physiotherapist [18]. The intervention sessions took place on Tuesdays, Thursdays, and Saturdays. The conventional exercise sessions included the same warm-up and cool-down exercises as the tai chi intervention (Table 1).
Table 1 Tai Chi and conventional exercise interventionThe waitlist controls maintained their normal daily routine care and were given the option to participate in either a tai chi or conventional exercise program after the 12-week assessment.
Sample size
A sample size of 81 was calculated with a power analysis using the F-test (one-way analysis of variance [ANOVA], fixed effects, omnibus) with the G*power program [19]. Following the methods of previous research, the participants were divided into three groups according to the presence of multiple independent variables and multiple regression modeling with a medium effect size (f2) of 0.36 [20], in which α was set to 0.05 and the power was set to 0.80. The results indicated that each group required 26 participants. The reported turnover rate of older adults participating in a similar study was 14% [21]; thus, the target number of participants in each group was 30 (90 in total).
Outcome measures
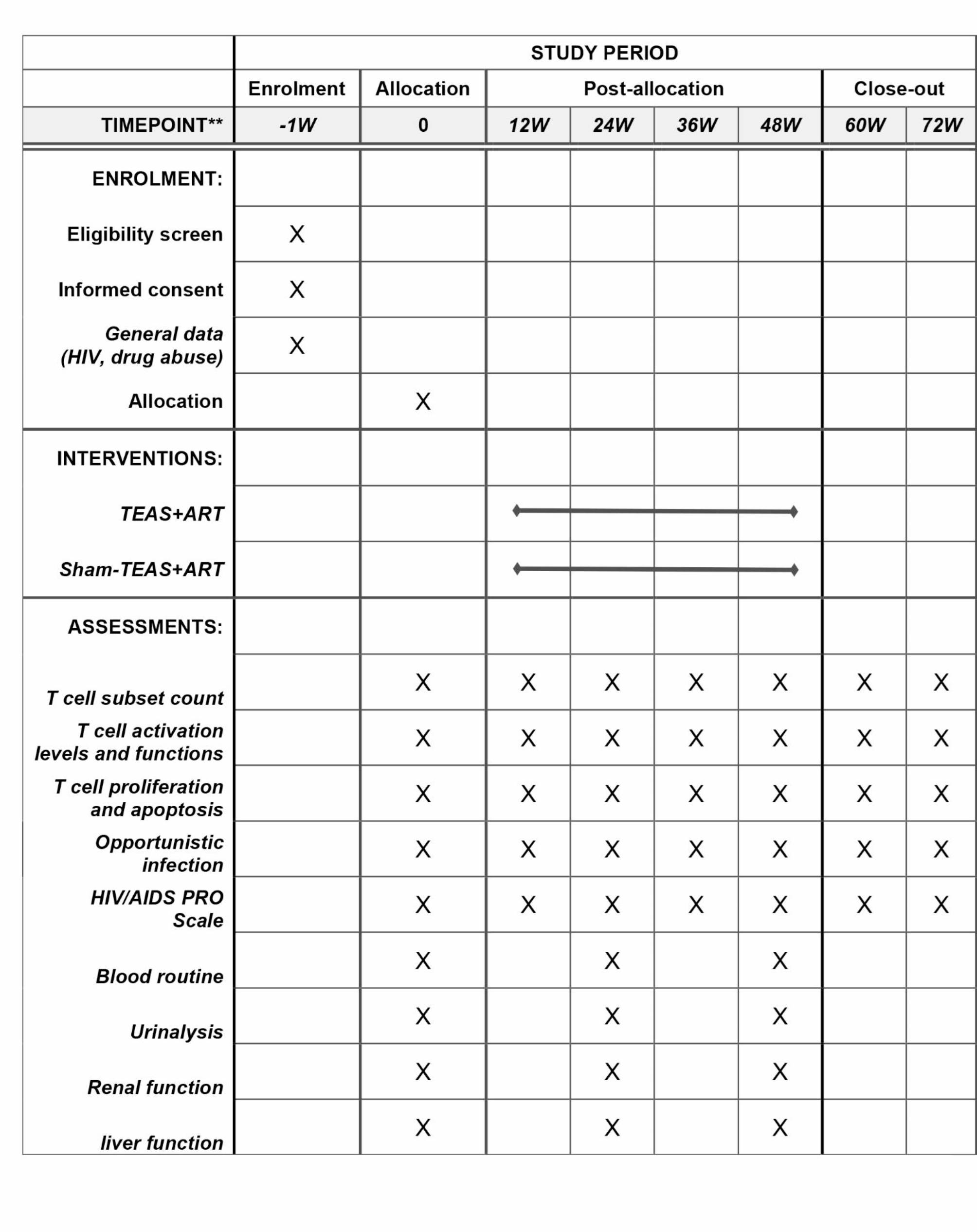
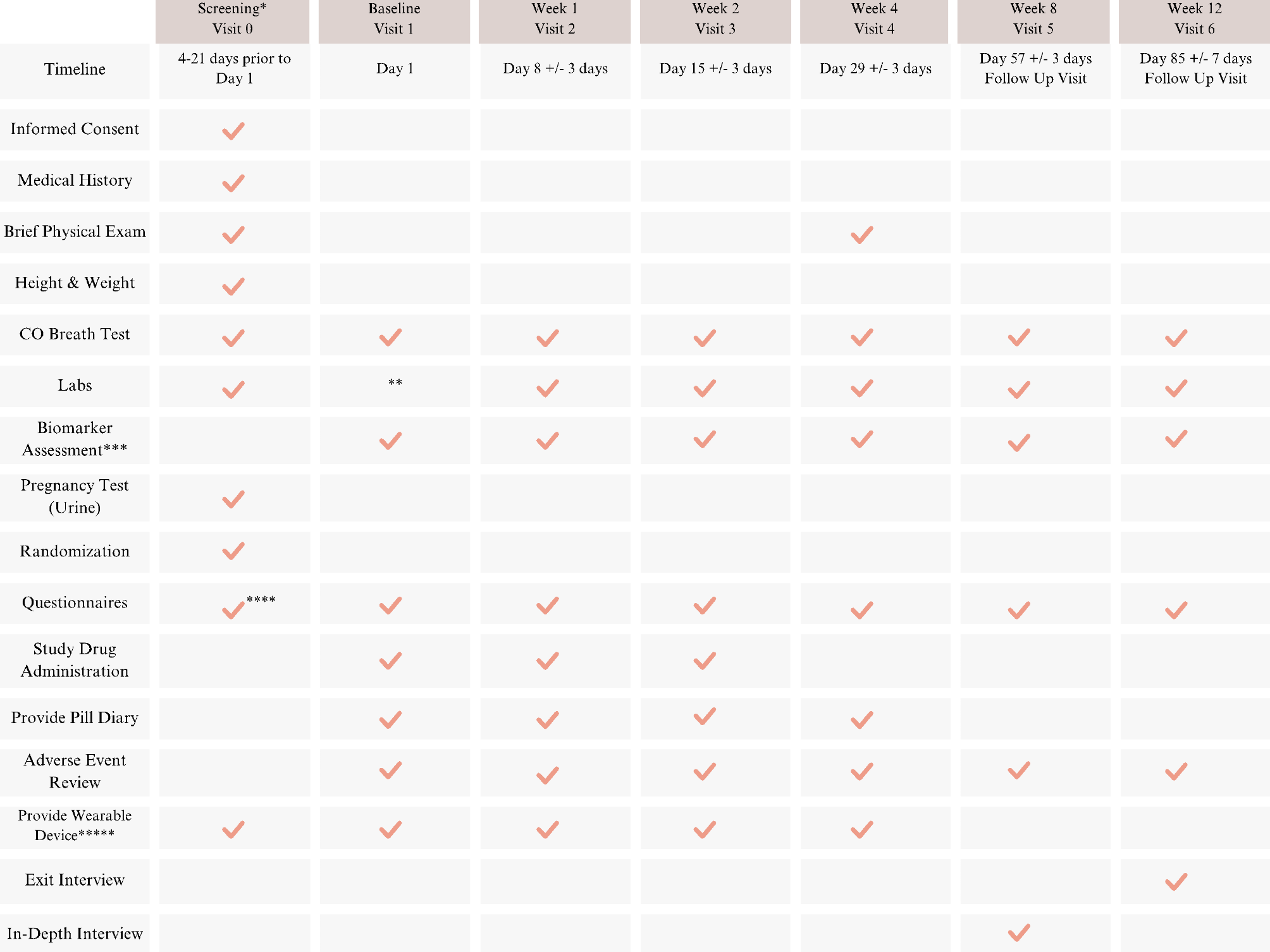
Outcomes were assessed at three time points: at baseline before randomization (week 0), during the intervention (week 6), and after the intervention (week 12). All outcomes were compared between assessment points and between groups. The primary outcome was physical performance, which was measured with the Short Physical Performance Battery (SPPB). The secondary outcomes were sleep efficiency, measured by an ActiGraph GT9X+ (ActiGraph in America) device, and quality of life, measured with the Quality of Life in Alzheimer’s Disease (QOL-AD) questionnaire. An objective method was selected to measure sleep quality because people with cognitive impairment typically have different degrees of cognitive impairment, and subjective scales, such as the Pittsburgh Sleep Quality Index (PSQI), cannot reflect the real sleep conditions of patients.
The Short Physical Performance Battery (SPPB) is one of the most commonly used assessment tools to measure comprehensive physical ability and can effectively quantify mobility among older adults, including their daily living ability, degree of physical weakness, prediction of fall risk, and sports ability [22]. The evaluation includes three sections: balance testing (in a parallel, semi-tandem, and tandem position for 10 s), walking speed (4 m), and standing up from a chair (sit-to-stand five times). Each test is evaluated separately. The overall SPPB score ranges from 0 to 12, and a higher score implies a greater physical functional performance.
ActiGraph is a wearable device used to record physical activity and sleep data. The device leverages recent advancements in science and technology to measure sleep with high sensitivity, comprehensive recording parameters, and a long monitoring time. Changes in sleep stages are accompanied by alterations in body movements, allowing the patient’s sleep state to be indirectly calculated by analyzing the activity parameters. Therefore, ActiGraph is a useful tool for measuring sleep quality. As early as 2007, the American Academy of Sleep Medicine (AASM) recommended using wearable devices as an auxiliary method for sleep evaluation [23]. Recently, more studies have utilized wearable devices to track sleep, verifying their use for the collection of objective sleep data in older adults with cognitive disorders [24]. This study used the ActiGraph GT9X+, which features a three-axis accelerometer, a gyroscope, a magnetometer, data filtering technology, and Bluetooth Smart technology to provide information on sleep latency, total sleep time, and sleep efficiency, as well as real-time participant data feedback. When collecting data, the sampling interval of the accelerometer was set to 60 s, and the sampling frequency was set to 30 Hz. ActiLife 6 software was used to analyze the data.
The QOL-AD was developed by Logsdon and colleagues at the University of Washington, United States [25], and Hu et al. translated and revised the scale to Chinese [26]. The scale includes 13 items, and each item is scored with a 4-point Likert scale, with 1 indicating ‘poor’ and 4 indicating ‘excellent’. The total score ranges from 13 to 52 points, and a higher score indicates a better quality of life. The scale can be evaluated by patients or caregivers; regardless of the evaluation method, the scale has good reliability and validity, with a Cronbach’s alpha ranging from 0.83 to 0.90. Many studies have used this tool to evaluate the quality of life of patients with cognitive impairment.
Data collection
The research team contacted the director of the nursing home and obtained permission to conduct the study after explaining the details of the protocol. The participants who met the eligibility criteria provided informed consent. Finally, participants were randomly divided into (i) a TC group, (ii) a CE group, or (iii) a waitlist control group with no intervention. All participants provided demographic data at baseline. They completed the SPPB and QOL-AD and wore an ActiGraph device for 72 h at three time points (0, 6, and 12 weeks).
Ethical considerations
The Institutional Review Board of Kobe University approved this study (approval number: 940), which was registered in the University Hospital Medical Information Network (UMIN) Center (registration number: UMIN000042051). Informed written consent was obtained from all participants. Codes were used to replace real names to ensure privacy. The data were locked and will be destroyed 3 years after the end of the study.
Data analysis
The data were entered and checked in two ways. For missing data, if the missing data accounted for less than one-third of the total data, the average of the available data was used to replace the missing data; if the missing data accounted for over one-third of the total data, they were omitted. Data were analyzed with SPSS version 26.0 (IBM Corporation). Baseline socio-demographic and clinical characteristics are presented with descriptive statistics. The feasibility measures were compared between the groups with one-way ANOVA, t-test, and Chi-square or Fisher’s exact tests. To account for missing values and correlation between repeated measurements, generalized estimating equations (GEEs) were used to compare the primary and secondary outcomes. The baseline measurement, time (the number of weeks from baseline), group (control group, TC group, or CE group), and group-by-time interaction were used as covariates. The group interaction, indicating the difference in a given outcome between interventions over time, was the primary measure of the intervention effect.
Missing values of quantitative data were not replaced because GEE analysis accommodates missing data under the assumption that they are missing at random [27]. Missing values for the SPPB, sleep efficiency, and the QOL-AD were managed by multiple imputations (SPSS PROC), given that these observations would otherwise be omitted from the logistic regression analysis.
This study used valid questionnaires and exercise interventions validated by international organizations. The study protocol was standardized, and the physiotherapist, research assistants, and assessors were trained to ensure consistency. Furthermore, the measurement instruments were valid and reliable, and all data were carefully checked immediately after collection. Finally, throughout the study, the research team regularly met to assess the study’s progress and ensure that it strictly followed the protocol.





留言 (0)