
記住我

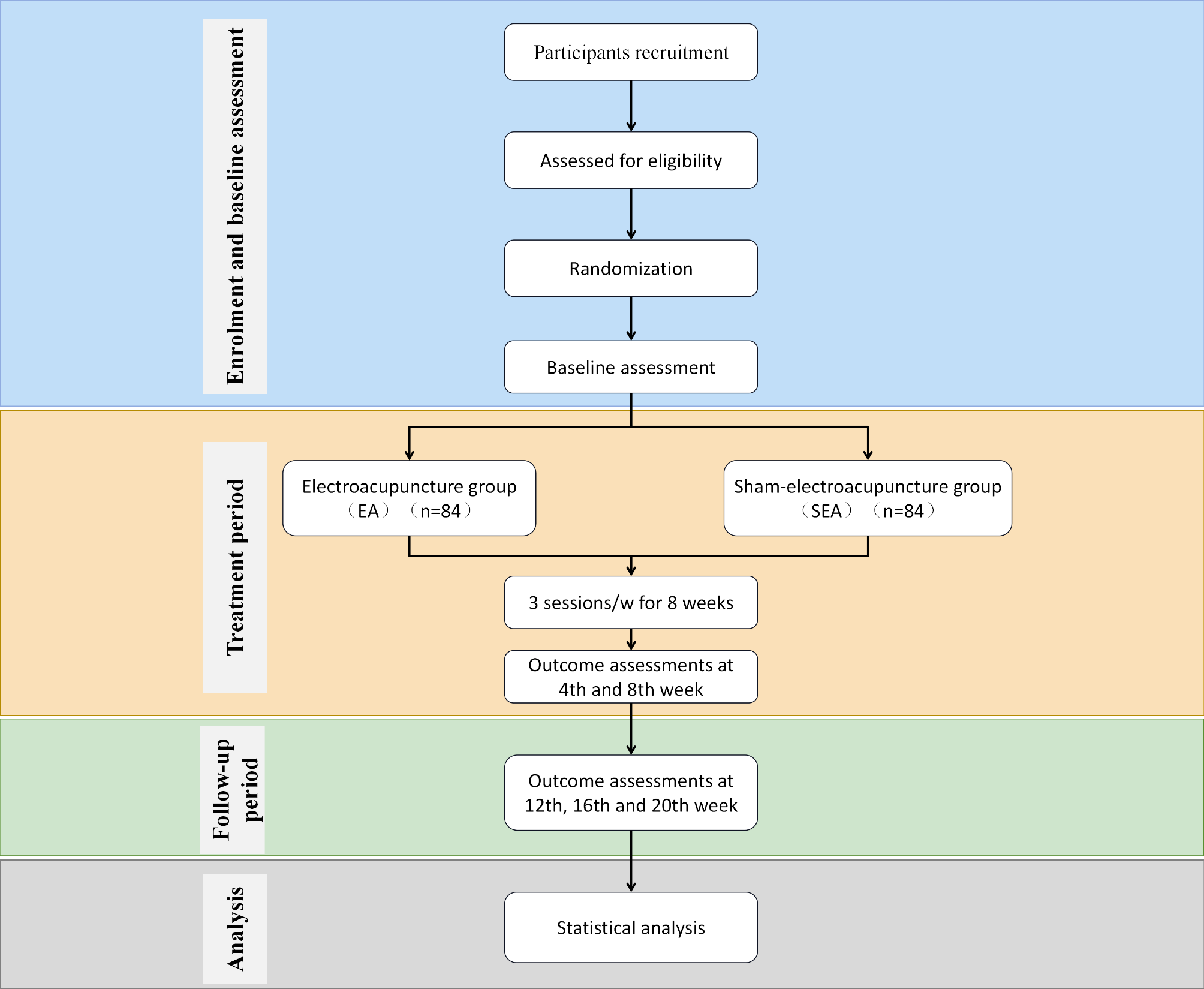

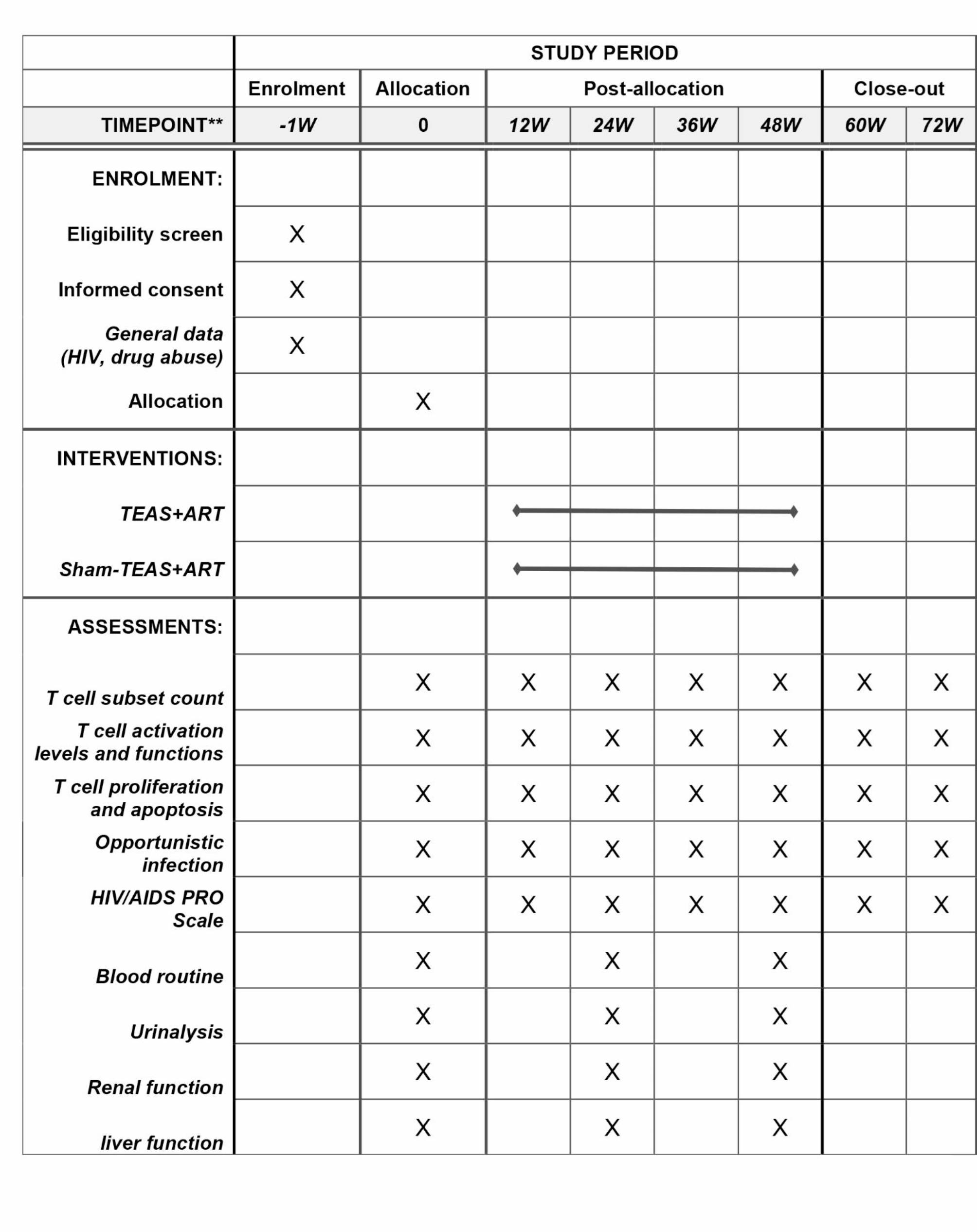


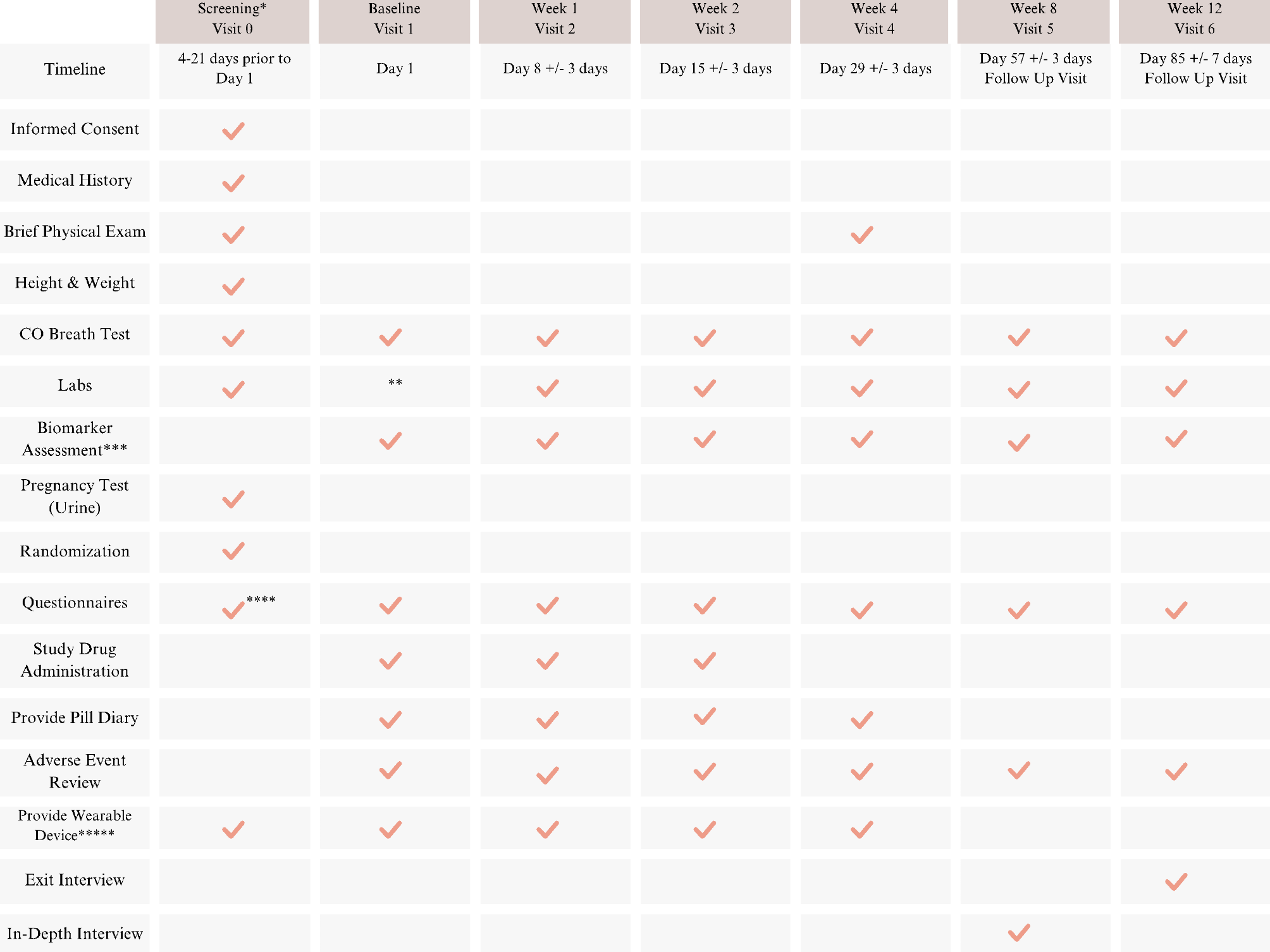
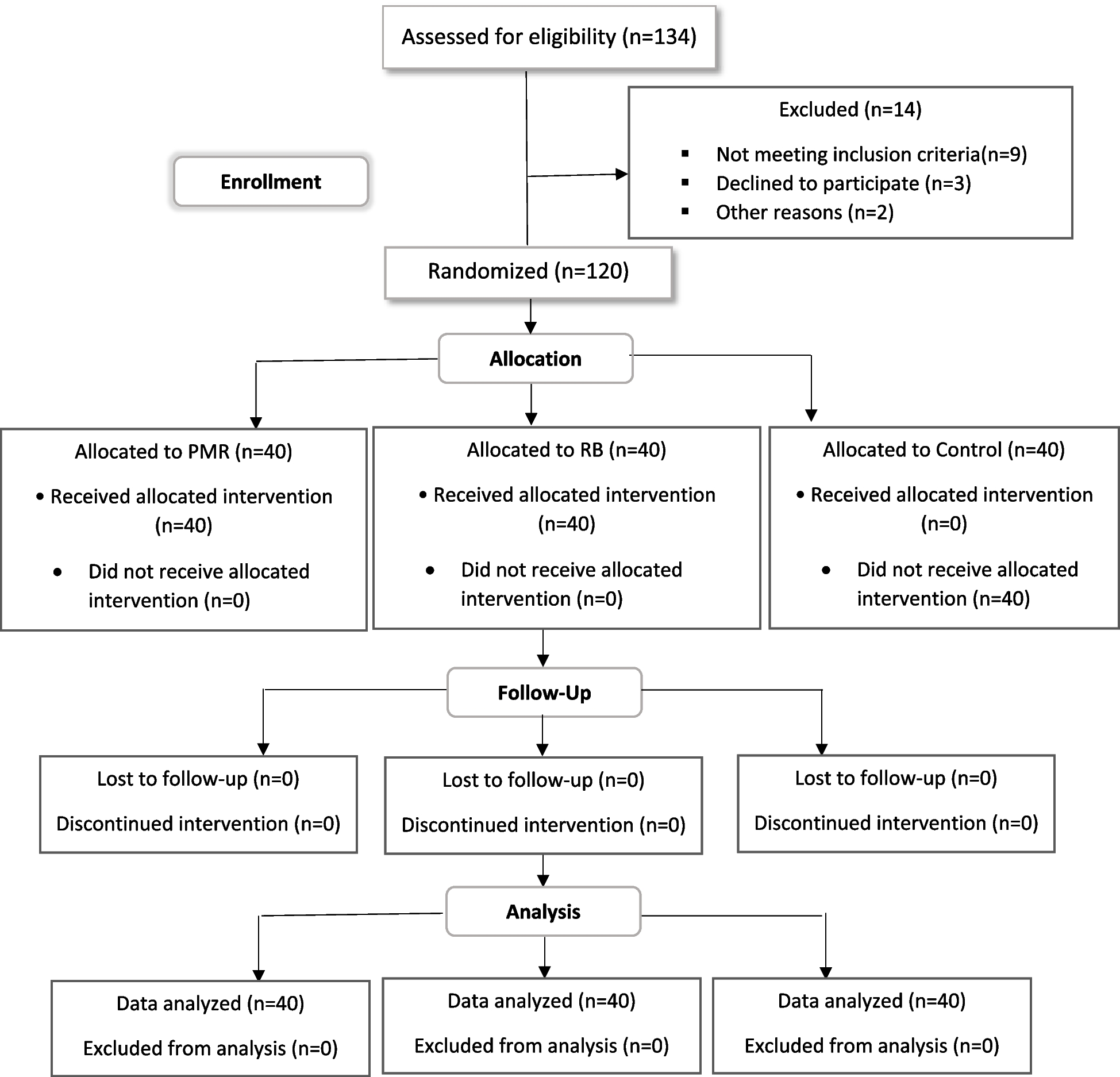
This is a two-center, randomized, non-acupoint controlled, single-blind clinical trial designed to demonstrate the efficacy of TEAS in improving INR among HIV/AIDS combined with ATS abusers. The study will be conducted at the Deyang Women’s Drug Rehabilitation Center and Ziyang Men’s Drug Rehabilitation Center in Sichuan, China, with drug users from all over the country. Patients who simultaneously satisfy ATS abuse and HIV immunological non-response will be included in our study and randomly divided into TEAS group and sham-TEAS group in a 1:1 ratio. The total observation period for this study will span 73 weeks, consisting of a 1-week baseline period, a 48-week treatment period, and a 12-week follow-up period. The study protocol follows the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) [34]. The SPIRIT schedule is shown in Fig. 1, and the flowchart is shown in Fig. 2.
Fig. 1 Fig. 2
Fig. 2 Diagnostic criteriaATS abuse
Diagnostic criteriaATS abuseAccording to the diagnostic criteria for ATS abuse withdrawal in the Diagnostic Manual of the American Psychiatric Association (DSM-5). [35]
1.Criterion A: The cessation of or reduction in prolonged use of amphetamine-type substances.
2.Criterion B: Dysphoric mood and at least two of the following physiological changes, developing within a few hours to several days after Criterion A: Fatigue; Vivid, unpleasant dreams; Insomnia or hypersomnia; Increased appetite; Psychomotor agitation or retardation.
3.Criterion C: The symptoms in Criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
4.Criterion D: The symptoms are not attributable to another medical condition or better explained by another mental disorder.
HIV immunological non-responseReferring to the diagnostic criteria for INR in previous relevant studies [16, 36].
1.CD4 + T lymphocyte count < 200 cells/µL in patients who have been receiving antiretroviral therapy (ART) for more than 1 year but less than 2 years.
2.CD4 + T lymphocyte count < 350 cells/µL in patients who have been receiving ART for more than 2 years.
3.After a prolonged period of treatment (e.g., 4–7 years), if the CD4 + T lymphocyte count does not exceed a specific threshold (e.g., > 350 cells/µL or 500 cells/µL) and HIV-RNA remains below the detection limit.
Inclusion criteria 1.The study includes individuals between the ages of 18 and 65, irrespective of gender.
2.Participants should have a history of previous ATS abuse and meet the diagnostic criteria for ATS withdrawal.
3.HIV patients should have received standard ART for a minimum duration of 1 year.
4.Participants should meet the diagnostic criteria for INR.
5.Following treatment, the viral load should be consistently controlled at a level below 50 copies/mL for at least 1 year.
6.All participants are required to provide voluntary informed consent by signing a consent form.
Exclusion criteria 1.Presence of uncontrolled serious opportunistic infections.
2.Coexistence of other serious organic diseases, such as tumors, cardiovascular diseases, cirrhosis, or mental illnesses, such as schizophrenia.
3.Participation in other clinical trials within the past 3 months.
4.Receipt of treatment other than the ART regimen within the past 1 month.
5.Coexistence of liver and kidney dysfunction.
Participants who meet the inclusion criteria but satisfy any of the above conditions will be excluded from the study.
Sample sizeAccording to relevant literature, the standard deviation of CD4 + T cell count in INR patients receiving ART is reported to be 137.77 [37]. This study is designed as a superiority trial, according to the sample size formula [38], α = 0.05, β = 0.2, unilateral test. The minimum effect size is set at 50 [39]. The sample size of n = 47 is initially determined. However, considering a 20% potential dropout rate, we have decided to collect 57 patients per group.
RecruitmentRecruitment of participants is scheduled to commence in October 2023 and is expected to be completed by September 2024. Due to the poor compliance of HIV patients with combined ATS abuse receiving ART therapy, we have decided to select the drug rehabilitation center as the research site. All HIV-infected patients in the center will receive or are currently receiving ART treatment. We will publicly recruit potential participants through posters, public lectures, and survey questionnaires.
Randomization and allocation concealmentStratified block randomization will be implemented in this study to ensure a balanced allocation of subjects across study centers. The randomization process involved dividing eligible subjects into two groups, namely the TEAS group and the sham-TEAS group, in a 1:1 ratio. We will use a computer system to generate a random sequence before starting to recruit patients. The randomization plan will be managed and maintained by a third-party randomization team, independent of the study investigators. The randomization scheme will be securely enclosed in a sealed opaque envelope with a unique code. The envelope will be handed over to the recruiting researcher. At the time of subject enrollment, the envelope corresponding to the subject’s assigned number will be opened to reveal the group allocation information.
BlindingIn this experiment, a blinding method will be employed for the participants to ensure they are unaware of the type of TEAS. However, due to the nature of the TEAS treatment, it is not possible to blind the acupuncture doctor. Nevertheless, the blinding assessment will be followed, and efficacy evaluation, as well as statistical analysis, will be conducted by third-party individuals who are not involved in the trial, achieving separation of research, evaluation, and statistics. To facilitate the blind evaluation process, the acupoints or non-acupoints will be labeled as A1, A2, B1, and B2 in the Case Report Form. The specific acupoints or non-acupoints will not be mentioned in the tables to further ensure blinding during the evaluation process.
InterventionsARTBoth groups of patients refer to the ART treatment scheme recommended in the 2021 Chinese HIV/AIDS Diagnosis and Treatment Guide [40].
TEAS and sham-TEASTEAS operation: Before treatment, the patients will be instructed to empty their bladder and lie flat on the bed. The TEAS electrode patch will be applied to the corresponding acupoint. The selection of acupoints is based on previous research [36, 41,42,43]. Detailed information about acupoint location is shown in Table 1; Fig. 3. The current intensity will begin at 0, and each button press will increase the intensity by 1 mA. The intensity of stimulation will be adjusted to a range of 15–25 mA, based on the patient’s maximum tolerance. The stimulation frequency will be set at 2/100Hz, with a density wave alternating every 3 s. The operation will be performed by two qualified Traditional Chinese Medicine practitioners trained in acupuncture techniques. TEAS recommends replacing a set of acupoint stimuli every three months. Based on the duration of this research experiment, it is suggested to alternate between two sets of acupoints. The left and right acupoints will be used alternatively, with only one side acupoint used during each treatment session.
Sham-TEAS operation: Before treatment, the patient will be informed to empty the bladder and lie flat on the bed. The electrode patch will be applied to the corresponding non-acupoint skin, and detailed information about acupoint positions is shown in Tables 1and Fig. 3. The current intensity does not exceed 5 mA and only produces a slight sensation under non-acupoint conditions to ensure psychological comfort and simulate the treatment experience. Two sets of acupoints are used alternately, with only one acupoint used during each treatment period. The operation will be carried out by two qualified doctors who have received acupuncture technical training.
Table 1 Non-acupoints and acupoints were used in the trialFig. 3
Location of acupoints and non-acupoints
Treatment time and observation periodART takes medication according to the prescribed treatment plan. Each acupoint receives 30 min of TEAS treatment, three times a week. The total observation period for this study will span 73 weeks, consisting of a 1-week baseline period, a 48-week treatment period, and a 24-week follow-up period.
Outcome measuresPrimary outcome measurementCD4 + T cell count: It is a crucial indicator for assessing the immune function recovery in individuals with HIV [44]. It holds significant importance in understanding the immune status and disease progression, determining disease staging, evaluating treatment effectiveness, and identifying potential complications in HIV-infected patients [40].
Secondary outcome measurementEfficiency of immune reconstitutionThe evaluation criteria for assessing the efficiency of immune reconstitution are outlined in the Chinese Medicine Diagnosis and Treatment Plan for AIDS (Adults) (2016 Edition), developed by experts organized by the China Administration of Traditional Chinese Medicine and the China Health and Family Planning Commission.
1.Effective: An increase in CD4 + T cell count of ≥ 50/µl or ≥ 30% compared to the baseline.
2.Stable: CD4 + T cell count shows an increase or decrease of less than 50/µl or less than 30% compared to the baseline.
3.Invalid: A decrease in CD4 + T cell count of ≥ 50/µl or ≥ 30% compared to the baseline.
T cell subset
1.CD4+/CD8+: The CD4+/CD8 + ratio is a crucial indicator of immune status that reflects the activation level of T cells. It holds significant importance in predicting the risk of CD4 cell depletion in HIV patients undergoing ART [45].
2.CD4 + CD45RA + and CD4 + CD45RO+: Following ART treatment, the early-stage immune reconstitution primarily involves the expansion of peripheral memory CD4 + T cells, while the later stage relies on the replenishment of naïve CD4 + T cells. Therefore, the quantification of CD4 + CD45RA + and CD4 + CD45RO + subsets is highly relevant for assessing the reconstruction of immune function [46].
T cell activation levels and functions
1.CD4 + CD28+: CD28 is a critical receptor on T lymphocytes that plays a vital role in their activation. Research has indicated a significant reduction in both the number and percentage of CD4 + CD28 + cells in individuals infected with HIV-1 compared to the general population [47].
2.CD4 + CD38 + and CD8 + CD38+: The expression levels of CD4 + CD38 + and CD8 + CD38 + molecules serve as crucial indicators reflecting the level of immune activation in the body [48, 49].
T cell proliferation and apoptosis
1.CD4 + ki67+, CD8 + ki67+: Ki67 is a non-histone protein found in the nucleus that serves as an important marker of cell proliferation. The expression of Ki67 indicates the presence of cells in the proliferative stage [50].
2.JC mitochondrial membrane potential detection/CD4+, JC mitochondrial membrane potential detection/CD8+: reflect the apoptosis rate of CD4 + T cells and CD8 + T cells.
Opportunistic infectionAccording to the Chinese AIDS Diagnosis and Treatment Guidelines (2021 Edition), the diagnosis of all opportunistic infections will be confirmed based on clinical manifestations and relevant auxiliary examinations. This diagnostic process involves the collaboration of two or more attending physicians.
HIV/AIDS PRO scaleThe HIV/AIDS PRO Scale will be used as a tool to evaluate the quality of life and health status of HIV/AIDS patients.
Data managementResearchers will be required to complete CRF in a timely, accurate, complete, standardized, and truthful manner. To establish a database, EpiData2.1 software will be utilized. Two well-trained data entry personnel perform parallel double entry of the data from the CRF table. After the parallel double entry is completed, the EpiData function is employed to compare and verify the consistency of the double entry. In cases where inconsistencies are identified during the comparison, manual verification will be conducted to compare and correct the data concerning the CRF data on an individual basis. Once the data verification process is completed, it will be submitted to the project team for review. The data administrator then will announce the locking of the data and securely store the password. The finalized data will be subsequently transferred to the statistical department for further statistical analysis.
Statistical analysisStatistical analysis will utilize SPSS 25.0 software. A significance level of P < 0.05 will be considered statistically significant for assessing differences. Continuous variables will be described using mean ± standard deviation, median, P25, P75, maximum, and minimum values. Categorical variables will be presented as percentages. Compare two groups of demographic data and other pre-treatment efficacy evaluation indicators between groups to measure comparability. Group t-tests are used for metric data that conform to a normal distribution, while nonparametric tests (Wilcoxon Test) are used if not. If there are significant differences in age, gender, disease type, or other relevant factors between the two groups before the experiment, or if there are significant factors that influence efficacy, these variables should be considered as covariates. In such cases, covariance analysis or logistic regression analysis will be performed. Primary per-protocol (PP) and intention-to-treat (ITT) analyses will be utilized for the main and overall indicators. We will use multiple imputations to process missing data.
Interim analysesThere will be no interim analysis.
Quality controlTo ensure the progression of the research, a clinical training meeting will be conducted prior to the clinical trial. This meeting will focus on training the project implementation plan and various standard operating procedures. All methods of TEAS will be recorded on video to maintain consistency in operation. Furthermore, all acupuncturists involved in the study will possess valid licenses and a minimum of 2 years of clinical practice experience in acupuncture. To ensure data and material security, all research documents (such as screening tables, CRF, and treatment records) and treatment materials will be stored in locked storage units at restricted study locations. Weekly checks of the CRF and records of acupuncture treatments will be conducted at each research site. Additionally, a quality control review will be performed every 3 months at each site, generating a comprehensive report on the research process’s overall quality. Regular meetings among the primary researchers will be held to discuss and address any issues that arise during the observation period.
Patient and public involvementThe development, outcome measures, study design, recruitment, and implementation of this study did not incorporate patient priorities, experiences, or preferences. The results will not be shared with the study participants. Moreover, the burden of intervention will not be assessed by trial participants. The findings of this study will be disseminated to the study participants exclusively through our hospital’s website. We will keep the personal information of any participants confidential.
Trial statusThis study is currently in the recruitment stage. Since December 2023, the participants have exhibited remarkable motivation, and the recruitment process has proceeded seamlessly.
留言 (0)