
記住我



The drugs were analyzed using RP-HPLC. The retention time was found to be 3.3 min and 5.1 min for DEX and MOX respectively in the combination setup (Fig. 1). For the individual drugs, the retention time was 4.2 min for both (Supplementary Fig S2 and S3). The drug concentration in the dilutions prepared from the stock was quantified using the developed method. The standard graph plotted was later used to analyze the drug loading and in vitro release profile (Supplementary data Fig S4).
Fig. 1
HPLC chromatogram for MOX (3.3 min) and DEX (5.1 min) at 239 nm wavelength, run in 50:50 acetonitrile: buffer
During the stability analysis, it was noticed that MOX was relatively stable with less than 10% degradation observed in 30 days. Gradual degradation was observed in the DEX sample (Fig. 2A). While the degradation was comparatively more pronounced when DEX was placed in combination with MOX with 35% degraded by day 30 (Fig. 2B). This is probably due to interaction between the drugs in liquid phase. The PLGA matrix has a protective effect on the drugs from preventing degradation inside the implant. The degradation is initated only on exposure to the buffer [34]. This protective effect ensures the stability of the drugs within the implant as it remains inside the PLGA matrix. The aquoues humor turnover is 1-1.5% of the volume per minute, thus there is a complete turnover of of the aqueous humor for about every 100 min [35]. The release from the implant is in controlled and sustained manner and once it releases from the implant, it will be cleared in less than a day inside the eye. Additionally, we are also investigating potential drug-drug interactions. Though there is some interaction between the drugs but degradation of DEX in first 24 to 48 h of interaction with MOX is negligible. The stability studies were conducted for a period of 30 days was guided by the recommendations provided in the All India Ophthalmological Society (AIOS) guidelines, specifying application of antibiotics for 2 weeks and anti-inflammatory drugs for 4 to 6 weeks. Given that moxifloxacin release was completed around 22 days and considering the stability of the drugs within the implant, a 30-day stability study period was observed.
Fig. 2
Stability profile of DEX (A) and MOX (B) individually and in combination in phosphate buffer of pH 7.4 kept at 37℃, analysed for a period of 30 days using RP-HPLC
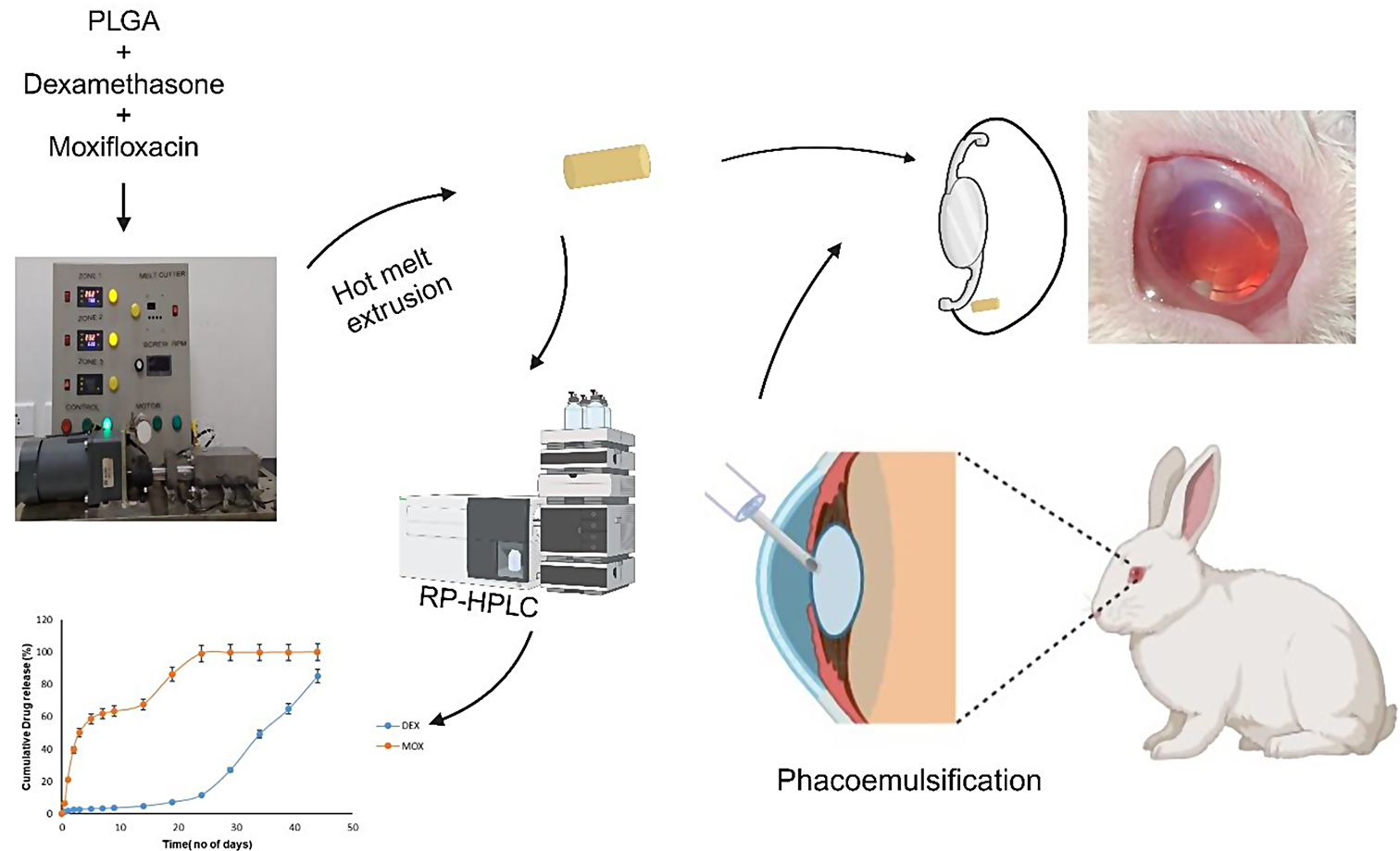
Implant preparation and characterizationThe implants were prepared using a single screw hot melt extruder by setting the heating to a temperature above the glass transition temperature of PLGA (Fig. 3A&B) [36]. Hot-melt extrusion emerges as a viable approach in crafting biodegradable implants, proving its effectiveness through its continuous and industrial-friendly process. Its distinct advantage lies in eliminating the requirement for solvents or water, setting it apart from methods reliant on solvents [37]. One of the limitations faced while using the extruder was the inconstistency in the size of the filament obtained. In order to achieve consistent drug loading with minimal variation, we maintained a constant weight, enabling us to attain the desired level of drug loading (Table 2).
Table 2 Dimensions and weight of implantFig. 3
The custom made single screw hot melt extruder (A-side view), (B-front view)
The filament was chopped to obtain implants weighing 1.6 mg each (Fig. 4). The combination implant had 270.3 ± 23 µg of DEX and 153.4 ± 12 µg of MOX per implant. DEX individual implant contained 268.8 ± 9 µg of the drug per implant and MOX individual implant contained 143.3 ± 2 µg of the drug per implant. The variation in drug loading among the three batches of prepared implant was found to be 3.1% for DEX and 8.4% for MOX.
Fig. 4
Implants- Plain PLGA(left) and DEX-MOX PLGA (right)
The amount of drug to be used for the preparation of implant was calculated based on the total drug utilised during the post-operative care while using eye drops, drug loading in established ocular implants and works by Yan et al., and Chennamaneni et al. While calculating the amount of drug utilized with eye drops, one drop was considered as 50 µl, and the values of 1% and 5% of the total drug used were taken, as these are considered indicative of the bioavailability of the drug upon application of eye drops. Yan et al. [17] developed a hydrogel system incorporated with DEX, MOX and Genistein and Chennamaneni et al. [20]developed an implant by compression of DEX loaded PLGA microparticles. Both studies have highlighted the use of approximately 100–300 µg of DEX and 200 µg of MOX in developing drug delivery systems intended for insertion into the capsular bag to manage post-cataract surgery complications though in vivo studies were not conducted in the work by Yan et al. Despite the lower quantity of drugs loaded into the implant in our study compared to the quantities reported in previous research, our findings indicate a notable therapeutic effect. Notably, the amount of DEX integrated into PLGA implant Surodex is significantly less than what was utilized in our study, but it is essential to acknowledge that the drug release profile of Surodex lasts only for 7 days [38].
XRD patterns were generated for DEX (Fig. 5), MOX (Fig. 6), PLGA (Fig. 7), and a combination of drug-loaded PLGA implants (Fig. 8) to understand the crystallinity of the developed product. The sharp peaks observed in the XRD patterns of DEX and MOX shows the crystalline nature of the two while the lack of the same in the XRD pattern of PLGA tells its amorphous nature. Characteristic broad peaks of amorphous nature were obtained on analysis of the drug loaded implant. This infers that the drugs are homogenously dispersed within the polymeric matrix.
Fig. 5
XRD of DEX showing sharp peaks indicating the crystalline nature of the drug
Fig. 6
XRD of MOX showing sharp peaks indicating the crystalline nature of the drug
Fig. 7
XRD of PLGA showing broad peaks indicating the amorphous nature of the polymer
Fig. 8
XRD of combination implant. The image shows broad peaks indicating amorphous nature, from which it can be inferred that the polymer masks the characteristic peaks of the drugs DEX and MOX and the drugs are uniformly distributed throughout the implant
Figure 9 shows the SEM image of the dual drug loaded implant. In Fig. 10 it can be observed that the surface turns more uneven over the course of the study. PLGA is a bulk eroding polymer [39], and the eroded areas seen on the surface show the degradation of the polymer. The primary mechanism behind drug release in PLGA polymer stems from a dual process involving the infiltration of water into its matrix and the gradual erosion of the bulk due to the hydrolysis of co-polymer chains [22]. On exposure to the aqueous medium, the water enters the system and initiates the degradation. The breakdown of PLGA into lactic and glycolic acid which resultes in the creation of an acidic environment, intensifying the autocatalyzing nature of the PLGA polymer [40]. When the drug is exposed to the penetrating water it either dissolves/diffuses out of the polymer matrix [41]. As the duration of exposure to the aqueous medium increases, the degradation is higher, as evidenced by the increased porosity observed on the implant.
Fig. 9
SEM image of the implant showing the implant length of 1.093 mm
Fig. 10
SEM image of the implant in phosphate buffer (pH 7.4) Row 1 left to right day − 0,7,21. Row 2 left to right- day28, 35,42. There is a gradual degradation as time passes when implant is placed in the buffer which can be observed in the increase in surface unevenness and porosity within the implant
In vitro drug releaseThe in vitro release profile is as shown in Fig. 11. It was observed that MOX was released at a faster pace than DEX in the combination implant. There was a release of about 22% of MOX in 24 h while for DEX it was 2%. A similar trend was observed for the individual drug implants (Supplementary data Figs S5 and S6). There was not much variation in the release profile of the drugs from the implant when loaded individually and in combination. According to the AIOS guidelines, for the first fifteen days antibiotic should be administered with an anti-inflammatory drug, and next fifteen days only an anti-inflammatory drug should be administered through eye drops [6, 31]. We obtained a similar release trend of the drugs from the developed implant.
Fig. 11
Release profile of DEX and MOX in combination implant when kept in phosphate buffer of pH 7.4 at 37℃. MOX releases at a faster pace and completes the release in about 20 days, while a lag is observed in the release of DEX in the first 15 days and the release extends to over a month
The PLGA polymer is used as the matrix. It is a biocompatible, biodegradable, and provides a method for controlled drug release for various time intervals [26]. Variations in the lactic acid: glycolic acid ratio, the molecular weight of the polymer, and the type of end group can help manipulate the drug release kinetics [20, 21]. DEX follows a triphasic release from PLGA implant which involves small burst release in the first 24 h which was about 2% which amounts to approximately 2 µg in this study, then a lag phase for about 15 days and then drug release increases from 3rd week onwards (Fig. 11). The initial burst release can be attributed to the loosely adhrerd DEX on the surface of the implant which is uncoated by the polymer matrix that can be easily released on exposure to water [42]. After the initial burst release in the first 24 h, the lag phase is noticed in the release of DEX which is approximately 12% of the total drug. This could be due to the hydrophobic nature of both the polymer and the drug which limits the exposure of drug to the buffer [25]. After the lag phase, a substantial increase in the release of DEX is noticed upto the completion of the drug release. This is because by this time there is sufficient degradation of the polymer and improved uptake of buffer into the matrix allowing the dissolution of the drug. Eye drops contains 1% DEX, each drop is considered 50 µl [43] and bioavailability of the drug on topical application is 1–5% [10]. In the first 24 h, the calculated amount of therapeutic drug (eye drop application 6 times a day) reaching the site of targeted tissue will be around 0.3–1.5 µg. In first 15 days, about 12% release of DEX occurced from the implant as observed in the in vitro studies. The drug quantities released from implant in this 15 days is within the cumulative amount of 1–5% bioavailability when eye drops are used for the same duration which is between 4.5 and 22.5 µg. From this we can conclude that there is no significant impact of the lag phase in the recovery of the rabbit. This triphasic release of DEX from PLGA implant has been reported for the intravitreal imlant Ozurdex [28, 42]. The difference in the release profile of DEX between the developed implant and Ozurdex can be attributed to its composition. The composition ratio of drug to polymer in Ozurdex consists of 60% DEX, 30% acid-terminated and 10% ester-terminated 50:50 PLGA (7-17KDa) [44]. However, in the fabricated implant, the ratio is approximately 17% DEX, 9% moxifloxacin (MOX) and 74% ester-terminated 50:50 PLGA (65-95KDa). The polymer drug ratio can also affects the release profile and the use of lower molecular weight and acid terminated PLGA increases the rate of degradation of the polymer [25]. Thereby, there is a shorter lag time and the release is completed faster in Ozurdex with the release being completed in about 30 days. The fabricated implant used in this study has higher molecular weight of PLGA and encapsulated much lesser amount of drug, leading to an increased lag time and longer release period. The release of DEX from the prepared implant is independent of the presence of MOX and a similar trend is observed in the release profile of the DEX only implant. The similar type of release was observed with thin film strip of PLGA encapsulated with DEX wound around the optic of IOL [19]. The faster release of MOX as noticed in the in vitro release profile may be because of the pronounced osmotic effect due to its hydrophilic nature [21].
In vivo studyRabbits eyes were chosen as a model for this study condering the various anatomical similarities between human eye and rabbit eyes [45]. A total of 12 rabbit eyes underwent cataract surgery and out of this four of them received the dual drug loaded implant. The implant was inserted into the capsular bag after the placement of the IOL (Fig. 12). The slit-lamp observations revealed that there was no significant anterior chamber reaction in all groups for the majority of the study period. But we had observed a small anterior chamber reaction on day 1 after surgery which was there in almost all operated eyes but was resolved in the subsequent days. No displacement of the IOL was observed. It was difficult to spot the implant during the weekly observations, probably due to the reduction in size, degradation of polymer and increased transparency of the implant due to release of drugs. The implant was in the capsular bag inferiorly in most cases (Figs. 13 and 14). In one case in the test group, the implant had stuck to the center of the bag while in another case it had migrated to the anterior chamber. IOP measurement were taken every week post surgery (Table 3). An increased IOP was observed in the test group during the period of study which may be due to high DEX concentration in the eye as observed in the in vitro release profile. Ocular hypertension or elevation of IOP due to application of steroids have been reported to be dosage and time dependent [46, 47]. Concerning the elevated IOP, glaucoma due to the long-term use of steroids is a known complication [48]. This can be managed by making adjustments to the steroid load during implant preparation. Insertion of the implant in the capsular bag will allow the bidirectional flow of drugs, increase the drug availability to the local tissues and the sustained drug release will turn improve the clinical outcome [49]. As the implant is biodegradable, the insertion of the implant during surgery helps to combine surgery and treatment without the need for surgical removal of the implant once the drug reservoir is exhausted [50].
Fig. 12
Implant insertion and positiong in the eye during surgery– left to right- Insertion, Position adjustment, Post adjustment in the capsular bag
Fig. 13
Implant in the capsular bag of the eye after surgery on day 1
Fig. 14
Operated eye at 6 weeks– from left to right- Normal control, Positive control, Sham control, Test. The implant can residue can be seen in the test sample behind the iris
Table 3 IOP measurements in rabbitHistopathologyAfter the observation period, the eyes of the rabbits from all groups were enucleated and taken for histopathology studies. On gross examination of the operated eye under the microscope, it was observed that the cornea was clear, the iris was normal, capsular bag was intact and IOL was in the capsular bag. The histopathology results are based on the report given by the pathologist. There was no gross histopathological variation observed in the samples of unoperated eyes. No significant pathology was observed in samples of the normal control group. Focal edema and a few chronic inflammatory cells were observed in the cornea of the samples from the sham control group. Edema and mild chronic inflammation of the cornea were observed in the samples of the positive control group. In the test group, the cornea was normal. Edema and mild chronic inflammation in the iris and the ciliary body was observed. One sample of the test group showed congested blood vessels in the choroid. The retina appeared normal with no significant pathology. Any other differences seen in the images are artifactual, and occurred during the preparation process of the specimens. The results revealed the biocompatibility of the implant at the site of insertion (Fig. 15). Images of the cornea, ciliary body and retina of all the samples are given in the supplementary data (Supplimentary data FigS7 a, b and c).
Fig. 15
Histology of ocular tissues of right eye at 6 weeks (A) Cornea, (B) Iris and ciliary body, (C) Retina. No significant pathology was observed between the various study groups (Scale bar − 100 μm)
留言 (0)