
記住我
Dear Editor,
Steatocystoma multiplex is a rare disorder characterised by the development of hamartomatous malformations at the pilosebaceous duct junction.1 We present the first documented case of steatocystoma managed successfully with percutaneous sclerotherapy using polidocanol.
A 24-year-old male patient presented with a 6-year history of multiple asymptomatic cysts on the anterior aspect of the neck [Figure 1]. These cysts ranged in size from 0.5 to 2 cm, were firm in consistency, and extruded oily-yellow fluid upon puncture. There was no family history. These cysts significantly impacted the patient’s quality of life.

Export to PPT
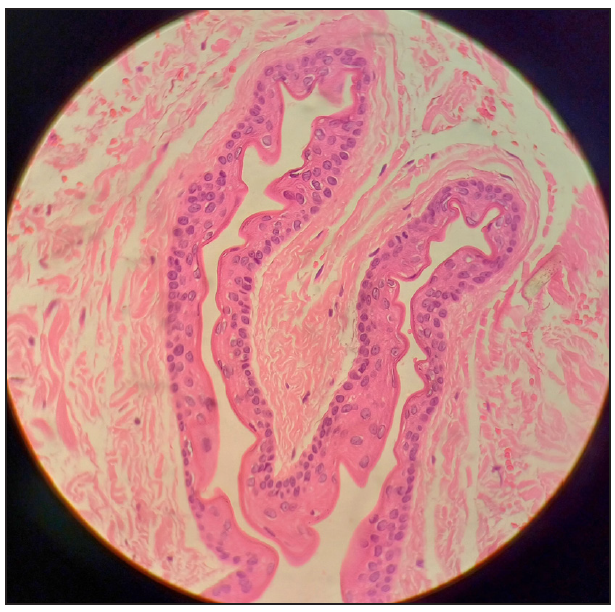
An excisional biopsy revealed a thin-walled dermal cyst with a sebaceous gland in the cyst wall, confirming the diagnosis of steatocystoma multiplex [Figure 2].
Export to PPT
Various treatment modalities, including excision, radiofrequency-surgery, laser, and cryotherapy, were discussed with the patient. However, due to concerns regarding scarring and pigmentary changes following surgery and cryotherapy respectively, and a desire for a less invasive approach, the patient opted for percutaneous sclerotherapy using polidocanol.
The area was anesthetised with topical EMLA (eutectic mixture of local anaesthetics) application for 1 hour. Cyst contents were aspirated, and a gentle refilling of each cyst was performed to inject approximately 0.1 mL of 3% polidocanol solution (1:1 with saline) per cyst. Following sclerotherapy, the patient reported minimal local pain which resolved without the need for analgesics. At 4-week follow-up, there was a notable reduction of cyst size and complete resolution of a few of the cysts. However, slight hyperpigmentation was seen on the skin overlying the cysts. Another subsequent session of polidocanol sclerotherapy was conducted for persistent cysts.
Our patient experienced a remarkable reduction in lesion size of most lesions [Figure 3]. No recurrence or rebound increase in size of lesions has been noted at a 3 month follow up visit.

Export to PPT
Steatocystoma multiplex typically exhibits an autosomal dominant inheritance pattern, although sporadic cases, as observed in our patient, can occur. The condition is associated with mutations in the keratin 17 gene (K17) with onset at puberty likely triggered by hormonal influences.2 Lesions most commonly manifest on the chest, abdomen, upper arms, armpits, and face.
Surgical interventions, such as excision, radiofrequency surgery, and laser carry the risk of scarring. Cryotherapy, although effective, may lead to pigmentary changes. Percutaneous sclerotherapy with polidocanol presents a promising alternative, especially for managing a larger number of lesions that are difficult to surgically excise.
Polidocanol, a detergent sclerosant agent, has been utilised safely for sclerotherapy in various indications, including digital mucinous cysts with minimal side effects.3,4 However, we could not find previous literature on the use of sclerotherapy or polidocanol in the treatment of steatocystoma multiplex. The recommended maximum dosage of polidocanol per session is 2 mg/kg body weight. In treating telangiectatic leg veins, the mechanism of action has been proposed to be protein theft denaturation of endothelial walls.5 In our case, a similar denaturation and damage to the cyst wall leading to a visible reduction in cyst size, could be the proposed mechanism of action. In cases where polidocanol is unavailable, alternative agents such as 1% sodium tetradecyl sulphate could be considered.
After two sessions of percutaneous sclerotherapy, our patient experienced a significant reduction in lesion size. The treatment was well tolerated with minimal side effects. Long-term follow-up is needed to assess recurrence, acknowledging that existing therapies also frequently encounter recurrences.
留言 (0)