Our study presents an overview of BD and GIBD incidence over time and the current treatment landscape for the Japanese working-age population and their families captured in the JMDC Claims Database. Accordingly, a scaling algorithm was applied where appropriate to reflect the age and gender structure of the general Japanese population.
With over 30,000 patients, the JMDC database included a significantly higher number of patients with BD in FY2021 than the 20,035 people who received medical care for BD in 2014, according to the Ministry of Health, Labour, and Welfare [21]. These discrepancies can possibly be attributed to the inclusion of suspected or mild cases in the database. GIBD was the most common subtype (14%) detected among patients with BD during FY2021. Surprisingly, during this time, more than half of newly diagnosed patients presented with GI involvement (1797 out of 3396 patients). In Japan, a substantially high proportion of GIBD has been reported in the past. Although prevalence and incidence rates vary considerably between studies (12–50%) [14], caution should be exercised when comparing and interpreting the data in terms of timing (study conduct and observation period), source of data collection (e.g., registry, database vs. individual hospital/institution), patient characteristics (e.g., age, sex, disease onset), and geographical aspects. The data may also vary due to different and evolving diagnostic criteria applied, distinct clinical disciplines involved (e.g., gastroenterology, rheumatology), or misdiagnosis (i.e., lack of consideration of differential diagnoses such as Crohn’s disease or ulcerative colitis).
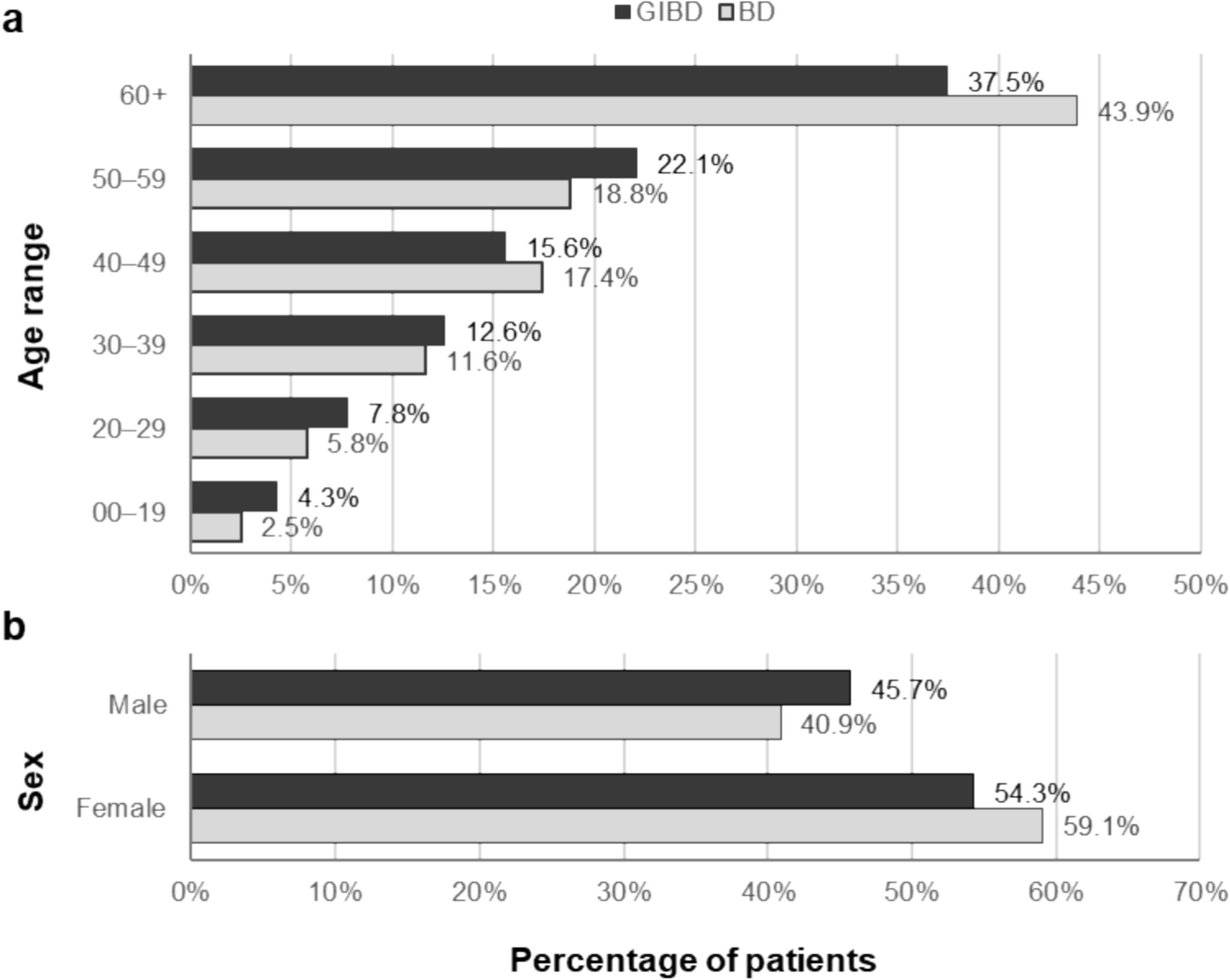
Slightly more female patients diagnosed with BD and GIBD were captured in the JMDC Claims Database, which was in accordance with other studies in Japanese and Korean populations [22, 23]. Further evidence from other Asian cohorts (from Türkiye and China) showed a more similar proportion of male and female patients with BD and GIBD, with a slightly higher proportion of males in the Chinese study [24, 25].
As described in previous studies, the frequency of patients with GI involvement reported in the JMDC Claims Database is higher than that of other regions from East Asia. Although countries such as Türkiye or Korea have a generally high BD incidence, only a small proportion of patients were reported to present GI lesions [2, 14]. In contrast, in other cohorts from Russia, the US, or the UK, which are known to have a lower BD incidence, a larger proportion of GIBD cases was observed [2, 14]. However, these data must be interpreted with caution, considering the different regional diagnostic criteria, and the possibility of misdiagnoses due to the lack of endoscopic assessments [14].
While GIBD might not be the most common BD subtype in other regions, an increasing trend in the presence of GI manifestations has been described in other Japanese and Korean studies. Research by Soejima and colleagues, who analyzed the clinical clusters contributing to the evolution of BD in Japan between 1991 and 2014, was based on data from a hospital-based regional BD registry as well as the Japanese national BD registry [7]. In this study, an increase in GI involvement in BD was observed, particularly after 2010 [7]. A similar trend regarding GI manifestations was also found in a Korean study, which analyzed a large hospital-based patient BD registry with data gathered between 1983 and 2012 [26]. Due to the similarities in the genetic backgrounds and previous diagnostic criteria in these countries [27], it is possible that at least some factors contributing to the prevalence of GI involvement in patients from East Asia are environmental. Interestingly, the adoption of a westernized lifestyle is believed to play a role in the recent expansion of other inflammatory bowel diseases in both Japan and Korea [28], which could also contribute to the predominance of GIBD.
In contrast, BD and overall GIBD incidence (including both confirmed and suspected GIBD cases) were shown to slightly decrease (annual rates of − 5% and − 1.7%, respectively) between FY2017 and FY2021, although this decline was more prominent for confirmed GIBD cases (− 15%). Changes in GIBD diagnostic parameters and therapeutic guidelines from the Japanese society for BD in 2020 [19] could be one of the key factors influencing this outcome, as the use of the proposed diagnostic algorithm is likely to help exclude false positives. These may also explain the discrepancies observed between the suspected and confirmed GIBD cases, with the latter being potentially underestimated. Moreover, improved hygiene in Japan, particularly during the SARS-CoV-2 pandemic, may have impacted GIBD occurrence. An alternative explanation is that GIBD was potentially underdiagnosed during the SARS-CoV-2 pandemic, due to restricted access to care. Interestingly, although both the SARS-CoV-2 virus and the COVID-19 vaccines have the potential to lead to systemic vasculitis, no events of BD post-infection or vaccination have been described [29]. The potential connection between SARS-CoV-2 (especially for the pre-Omicron viral variants) and the development of some autoimmune diseases, including ulcerative colitis, has been documented; whereas, other syndromes, such as Crohn’s disease, seem to be less likely to occur after a COVID-19 infection [30]. Other reports have shown minimal disease flares upon COVID-19 vaccination for some inflammatory and rheumatic diseases [31,32,33].
The extended use of TNFαi for BD treatment, as well as for other diseases (e.g., Crohn’s disease or ulcerative colitis), may have impacted the management of BD and its evolution. TNFαi administration increased both for BD and GIBD between FY2017 and FY2021 (annual rates of + 5.6% and + 8.1%, respectively). In particular, during FY2021, adalimumab use was slightly higher than infliximab, which could be due to infliximab being approved at a later timepoint than adalimumab for this indication [12, 16,17,18,19]. Compared with other subtypes, treatment with TNFαi biologics was highest for GIBD (48%), although it was observed that TNFαi were mainly prescribed to patients with confirmed GIBD, while they were less frequently used to treat suspected GIBD cases. A differential diagnosis of GIBD is complex due to similarities with other disorders, such as inflammatory bowel syndrome, Crohn’s disease, and ulcerative colitis [34], as well as simple ulcers in the GI tract, but a correct diagnosis is essential to ensure access to and maximum benefit from appropriate therapies [10].
Aside from the BD subtype, another aspect that was shown to influence the use of TNFαi was the medication previously used. TNFαi treatment for GIBD was often initiated in the third-line setting (in 42% of cases), which suggests that patients who receive TNFαi may be heavily pre-treated. In addition, only 12–18% of patients received TNFαi monotherapy, while the majority was administered TNFαi in combination with GCs, 5-ASA, and/or other immunomodulators. The information captured in the JMDC Claims database reflects the use of several immunomodulators, including AZA, mercaptopurine hydrate, MTX, and ciclosporin A. While thiopurines are widely employed to manage GIBD, with their use being recommended by the Japanese BD guidelines for patients who are dependent on GCs, or for those in whom GCs and/or TNFαi are ineffective, the efficacy of MTX remains unclear, and their use as monotherapy is not advised [19, 35]. Physicians’ specialization might influence immunomodulator administration, with MTX being more commonly prescribed among rheumatologists and AZA among GI specialists.
Given the secondary effects of long-term GC use and the promising efficacy results observed with TNFαi and other biologics, these agents could potentially become a GC-sparing therapy [12]. In accordance with this, a retrospective study based on patients with ulcerative colitis captured in the JMDC Claims Database showed a decrease in the use of GCs between 2006 and 2016, as treatment with biologics increased, although inappropriate use of GCs (such as long-term regimens) still persisted [36]. A recent study demonstrated that TNFαi monotherapy, or a TNFαi in combination with reduced GC doses, showed better potential for GIBD management in terms of GI ulcer healing and relative to GC monotherapy [37]. In this study, GC use also showed a decrease between FY2017 and FY2021 for patients with GIBD, which could be attributable to the introduction of biologic agents. The initial dosage remained stable over the study period (14 mg or 15 mg prednisolone, administered for a duration of 28–34 days ± 3 days). However, the lack of information related to the GC dosage over time limits the conclusions, notably about the tapering effect, and would need additional exploration [37]. Currently, although early introduction of TNFαi is encouraged in the Japanese BD guidelines [19], GIBD treatment in Japan still relies heavily on GCs, followed by immunomodulators and TNFαi.
Reimbursement access and the costs associated with TNFαi treatment may also affect the timing of biologic use in Japan, with TNFαi only available at earlier treatment stages for severe BD cases. Reimbursement benefits were also suggested to affect biologic use in Korea [38]. Moreover, the treatment patterns between 2011 and 2014 in Korea, as described by Han and colleagues, were similar to those in Japan, with GCs being the main therapeutic option (in 53.2% of patients), followed by immunomodulators (35.6%) and TNFαi biologics (4.7%) [38].
Treatment duration and AEs were also recorded in the JMDC Claims database. High adherence to TNFαi regimens was observed (around 80% after 3 years); however, a large proportion of patients experienced severe AEs (40%), especially related to infections. Previous systematic reviews have already identified increased vulnerability to infections as one of the main complications associated with TNFαi treatment [39,40,41,42]. Another complication, which is related to the severity of BD and is among the main causes of morbidity and mortality, is the appearance of intestinal perforations [14, 15]. In this study, intestinal perforations were observed in 2% of patients with GIBD receiving TNFαi biologics. This shows an important decline compared to the incidence reported in earlier studies, where these occurred in up to 13–25% of patients with GIBD [15, 43, 44]. The inclusion of BD treatments other than TNFαi, such as high-dose GCs, may have contributed to the risk of developing perforations in previous research [10]. In addition, differences in the patient population recruited across studies, and their predisposition to suffer intestinal perforations, could have also affected these results.
Surprisingly, in contrast to the high proportion of patients experiencing severe AEs, only 4.3% of patients with GIBD discontinued TNFαi treatment per year. The high retention rate suggests that, aside from a high efficacy, AEs associated with TNFαi use may generally be manageable [41, 42]. Nonetheless, further analyses comprising not only the working-age population and their families, but the general population, are needed to better understand the long-term AE profile of TNFαi and other biologic agents.
It is important to address the unresolved unmet need for the small group of patients that discontinue TNFαi treatment, but who could potentially benefit from other biologic agents or alternative treatments. Previous research has identified several clinical variables as predictors for GIBD prognosis. Variables such as younger age at diagnosis, history of surgery, and lack of initial response to medication, among others, have been linked to a poor prognosis [45]. Although these factors need to be further studied to fully understand their predictive power, they may be helpful tools for a more personalized and effective care, which could especially help subgroups of patients with these unmet needs. A more complete understanding of the genetic predisposition underlying GIBD, including HLA-B51 and other genetic factors, as well as investigation of emerging treatments for GIBD management, which may involve different targets aside from TNF-α, will also contribute to achieving these goals.
Some limitations are to be considered when interpreting the JMDC data, as only patients who visit hospitals or clinics and are covered by company health insurance are captured in the dataset. Since Japanese employees tend to remain insured with the same health insurance company for several years, which assigns them a personal ID, they can be followed over various time periods, even if they are treated by different medical facilities [46, 47].
Age and sex are included in the database, but it only comprises the working-age population and their families, i.e., the elderly population (60–75 years of age) is drastically underrepresented (≤ 3% vs. ~ 9–10% for younger age groups), which is important given that the overall Japanese population is aging. Accordingly, no comparative analyses, e.g., on drug use in elderly versus younger patients with BD, can be carried out with the necessary robustness based on the JMDC data, even if these are of scientific interest. Furthermore, direct comparisons with other studies and more representative populations may need to be interpreted with caution.
Another known limitation of the JMDC is the lack of information on disease severity, extension of inflammation and treatment outcome [46]. Accordingly, this study was not designed to analyze corresponding time trends related to any of these.
Furthermore, many AEs may not be captured in the database, and may, therefore, be underrepresented. In addition, patients with multiple comorbidities, including disorders that may also respond to TNFαi treatment, have the potential to be classified under another diagnosis and, therefore, not captured in this analysis.
Surgery rates have not been assessed in this manuscript due to limited data on whether patients have been followed and recorded from their first surgery, and whether they had subsequent surgeries.
Furthermore, it should be noted that the JMDC database collects data from Diagnosis Procedure Combination (DPC) and non-DPC hospitals nationwide, and the given dataset does not allow for sufficiently accurate analyses by geographical regions and prefectures [20].
In conclusion, while BD and GIBD prevalence slightly increased in Japan between 2017 and 2021, incidence declined, which was particularly notable for confirmed GIBD cases. In parallel, the use of TNFαi biologics for BD and GIBD management increased over the same period in Japan. This change in BD treatment patterns, along with the Japanese diagnostic criteria adjustment in 2020, may have impacted the observed decrease in GIBD incidence. Further studies are needed to better understand the effectiveness of TNFαi biologics to treat GIBD as well as other BD subtypes, and to help achieve a more personalized treatment approach. These strategies may improve the availability of TNFαi biologics in Japan, potentially replacing the long-term use of GCs, which are often still administered as the initial therapeutic option for BD management.



留言 (0)