
記住我


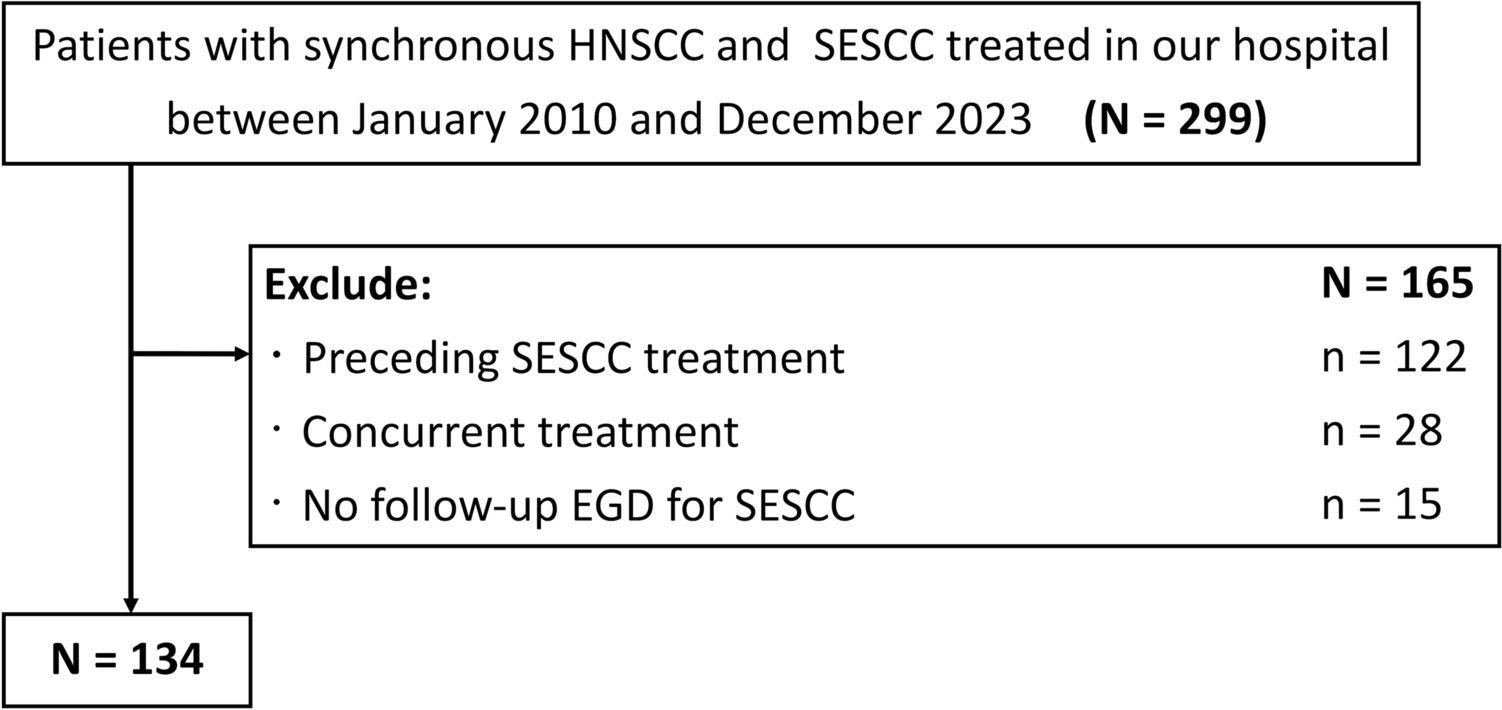
Between January 2006 and December 2015, 2027 patients underwent esophageal ER at 64 hospitals and were confirmed as having pT1a-MM with LVI or pT1b or deeper ESCC (Fig. 1). Of them, 1139 met the initial criteria, of which 472 met the secondary criteria and were analyzed in this study. Of the 472 patients, 192 underwent surgery, and 280 received CRT. The background characteristics of the 472 patients are shown in Table 1. Their median age was 65 years (range, 37–80 years); performance status was 0–1 in all patients; and the preoperative diagnosis was T1a-epithelial/lamina propria mucosa in 118 (25.0%) patients, T1a-MM/T1b-submucosa1 (SM1) in 282 (59.7%) patients, T1b-SM2 in 65 (13.7%) patients, and unknown in 7 (1.5%) patients. Endoscopic mucosal resection was performed in 48 (10.1%) patients, and endoscopic submucosal dissection was performed in 424 (89.9%) patients. The median follow-up period was 7.05 (range, 0.19–15.25) years. The follow-up rates at 5 years and 10 years were 94.1% (91.3% for surgery and 96.1% for CRT) and 36.8% (31.2% for surgery and 41.3% for CRT), respectively.
Fig. 1
Study flowchart. a Some patients were excluded for one or more reasons
Table 1 Background characteristics of eligible patientsPropensity score matchingA 1:1 propensity score-matched analysis of 472 patients was performed, with 160 patients selected from the additional surgery group and 160 from the additional CRT group. Baseline characteristics of the surgery and CRT groups are shown in Table 2, with their ratios before and after matching. After propensity score matching, age, body mass index, lymphatic invasion, venous invasion, and tumor circumference were adjusted. The radiation dose in the 160 patients in the CRT group was 40–41.4 Gy in 138 patients (86.2%) and 42–50.4 Gy in 22 patients (13.8%). The chemotherapy dose per course was cisplatin 70 mg/m2, fluorouracil 2,800 mg/m2 in 153 patients (95.6%), and cisplatin 75 mg/m2, fluorouracil 4,000 mg/m2 in 7 patients (4.4%). Of the 160 patients in the surgery group, 56 underwent open surgery, and 104 underwent thoracoscopic surgery.
Table 2 Baseline characteristics of the surgery and CRT groups before and after propensity score matchingSurvival analysisFigure 2 shows OS and RFS in the surgery and CRT groups. The OS did not differ between the surgery and CRT groups (hazard ratio, 0.887; 95% CI 0.542–1.453; P = 0.635). The 5-year OS was 89.1% (95% CI, 84.3–94.1%) and 90.0% (95% CI 85.5–94.8%) in the surgery and CRT groups, respectively. The RFS also did not differ between the surgery and CRT groups (hazard ratio, 1.036; 95% CI 0.662–1.623; P = 0.876). The 5-year RFS was 83.7% (95% CI, 78.1%−89.8%) and 86.6% (95% CI 81.4–91.2%) in the surgery and CRT groups, respectively. Supplementary Fig. 1 shows CSS and MFS in the surgery and CRT groups. Similarly, CSS and MFS did not differ between the surgery and CRT groups. The 5-year EFS in the CRT group was 90% (95% CI 0.855–0.948).
Fig. 2
Overall survival and relapse-free survival in the surgery and CRT groups. a Overall survival. b Relapse-free survival
Figure 3 shows OS and RFS for the low-risk and high-risk patients in the surgery and CRT groups. The hazard ratio was calculated as the ratio of CRT to surgery. In the low-risk group, the CRT group had better OS and RFS than the surgery group, but not significantly (hazard ratio, 0.556; 95% CI 0.266–1.159; P = 0.112, and hazard ratio, 0.657; 95% CI 0.339–1.277; P = 0.213, respectively). Conversely, in the high-risk group, the surgery group had better OS and RFS, but not significantly (hazard ratio, 1.412; 95% CI 0.707–2.825; P = 0.326, and hazard ratio, 1.497; 95% CI 0.791–2.833; P = 0.212, respectively). In the CRT group, OS and RFS were significantly worse in the high-risk group than in the low-risk group (hazard ratio, 2.208; 95% CI 1.096–4.444, P = 0.023 and hazard ratio, 2.141; 95% CI 1.172–3.906, P = 0.011).
Fig. 3
Overall survival and relapse-free survival in the surgery and CRT group divided into two subgroups (low-risk group and high-risk group). a Overall survival. b Relapse-free survival
Supplementary Table 1 shows OS and RFS divided into five categories according to depth and LVI: pT1a-MM with LVI, pT1b-SM1 without LVI, pT1b-SM1 with LVI, pT1b-SM2 without LVI, and pT1b-SM1 with LVI. There were no significant differences in OS and RFS between surgery and CRT in any category. In the low-risk group, hazard ratios of OS were 0.329, 0.541, and 1.102 in pT1a-MM with LVI, pT1b-SM1 without LVI, and pT1b-SM2 without LVI, respectively. OS of pT1a-MM with LVI was slightly better than pT1b without LVI. However, the results for these five subdivided categories are only informative data due to the small sample size.
Table 3 shows the recurrence patterns and periods in all patients, low-risk patients, and high-risk patients. In the surgery group, no esophageal recurrence was observed, and all 15 (9.4%) metastatic recurrences were observed within 5 years. The latest metastatic recurrence in the CRT group was observed 7.6 years after ER. In the CRT group, esophageal and metastatic recurrences were observed even after 5 years. In the CRT high-risk group, nine patients (13.4%) had esophageal or metastatic recurrence after 5 years.
Table 3 Recurrence patterns and periods in the surgery and CRT groupsIn the CRT group, 138 patients received 40–41.4 Gy of radiotherapy (low-RT dose) and 24 patients received 45–50.4 Gy (high-RT dose). Death from any cause during the observation period was 27 (19.5%) in patients who received low-RT dose and 7 (31.8%) in patients who received high-RT dose. Death from esophageal cancer was 12 (8.7%) in patients who received low-RT dose and 4 (18.2%) in patients who received high-RT dose.
Adverse eventsAEs in the surgery and CRT groups are shown in Table 4 for the patients selected after matching. The major early AEs in the surgery group were anastomotic leakage, recurrent laryngeal nerve palsy, and lung infection. The major early AEs in the CRT group were anorexia and fatigue. In the surgery group, one patient died of a lung infection on postoperative day 87. The major delayed AEs in the surgery group were ileus and gastrointestinal stenosis. In the surgery group, one patient died of ileus 10.2 years after surgery. In the CRT group, there were few delayed AEs more than 30 days after treatment completion.
Table 4 Adverse events of the surgery and CRT groups
留言 (0)