Reoperation
Surgical intervention alleviates the mass effect, relieves associated neurological symptoms, decreases the risk of recurrence, and provides for diagnosis and molecular characterization.5 All of these factors are important when discussing the advantages of reoperation. However, despite plentiful data on the morbidity and mortality associated with initial meningioma resection, information on re-resection in recurrent cases still needs to be determined. A recent analysis found that 48% of the reoperation cases experienced at least one complication in their postoperative care. Pre-radiation tumor location and the experience of the neurosurgical team are essential variables in this context [6, 7].
Genomic factors
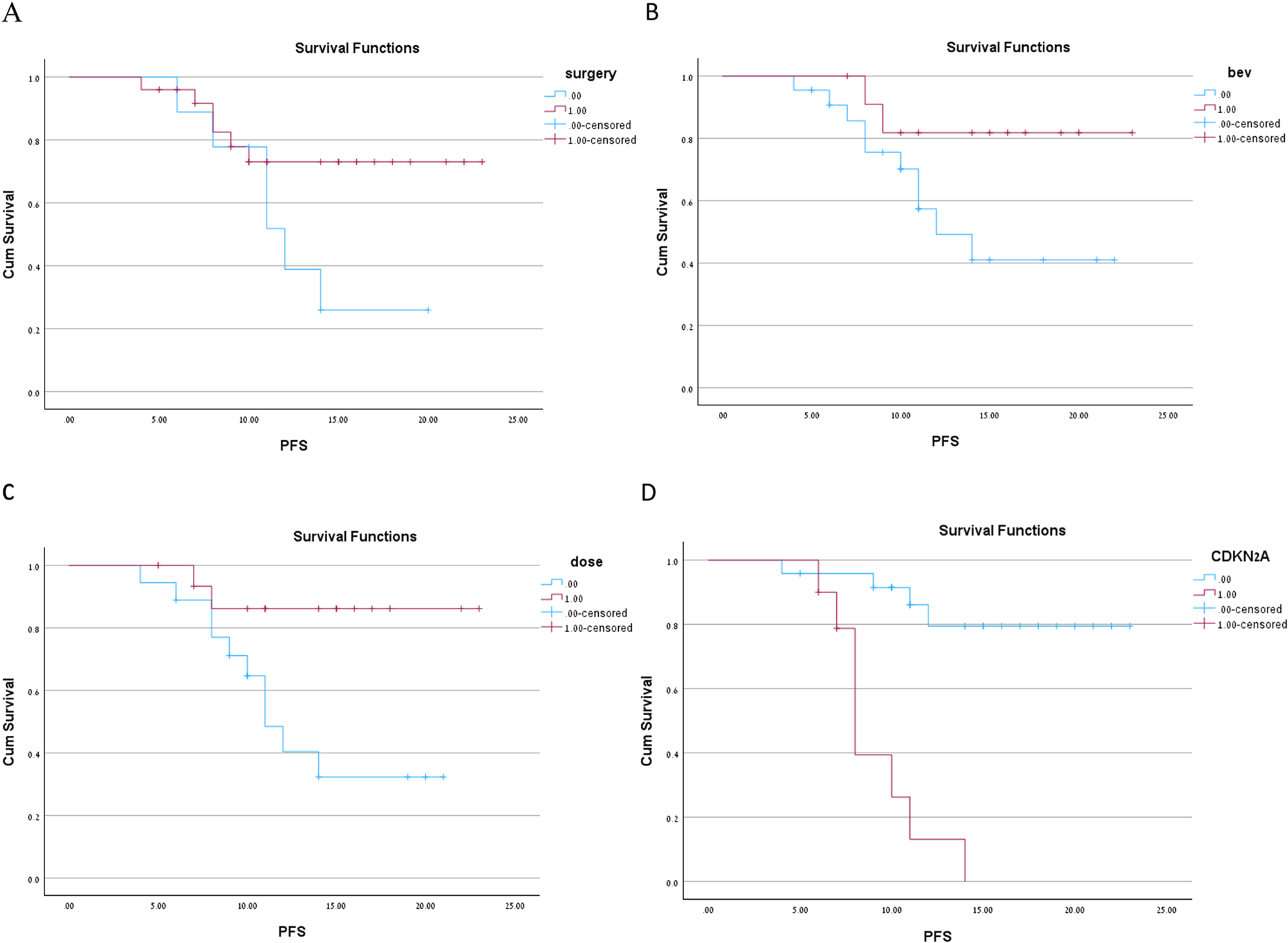
In our cohort, ten patients had CDKN2NA homozygote deletion (more than 50%). With the recent 2021 update of the WHO Classification of Central Nervous System Tumors, homozygous deletions of CDKN2A/B are sufficient to classify meningiomas as CNS WHO grade 3 tumors regardless of histological grading [3]. Meningiomas harboring homozygous deletions of CDKN2A/B are characterized by high recurrence rates independent of WHO grade, DNA methylation class, sex, age, and tumor location [4]. Additionally, heterozygous loss, mutations, and promoter methylation of CDKN2A were strongly associated with recurrent meningiomas and a high Ki-67 index [8]. Physiologically, the proteins encoded by CDKN2A/B halt the cell cycle; consequently, homozygous loss leads to dysregulated cell cycle progression and uncontrolled proliferation [8]. In our cohort, a strong relationship was observed between disease recurrence after 2nd RT and CDKN2a Del. Anaplastic meningioma with CDKN2A loss has a poor prognosis, even in re-radiation.
Dose regiment and bevacizumab treatment
The optimal RT approach for grade 3 meningioma in the recurrent setting remains controversial regarding clinical target volume (CTV) margins and dose prescription. Regarding dosage regimens for in-field recurrence, data on hypofractionation treatment and stereotactic radiosurgery exist, primarily relating to atypical rather than anaplastic meningioma.
The dose-response relationship is more established in anaplastic meningioma, as evidenced by publications in the adjuvant setting. Pontoriero et al. demonstrated that in 16 patients who received 72.5 Gy EQD2, treated with a combination of IMRT and radiosurgery, a 3-year PFS of 75% in sub-totally resected or recurrent grade 2 meningioma [9]. Lee et al., In a cohort of 21 patients who received IMRT to a median GTV dose of 66 Gy (range, 63–69 Gy), reported 3- and 5-year PFS rates of 88.4% and 73.5%. With a mixed photon/proton technique, [10] Chan et al. escalated doses to 68.4 to 72 Gy and found that 5 of the six patients with grade 2 or 3 meningioma achieved long-term local control at a mean follow-up of 145 months [11]. Moreover, most recently, Zhen et al. concluded that the dose-escalation cohort (≥ 66 Gy equivalent dose) improves local control and PFS (HR-0.42) [10].
Dose escalation above 50 Gy (BED), for example, 40 Gy in 10 fractions or 32.5 Gy in 5 fractions, appears crucial for improving progression-free survival at the cost of a high RN rate.
Concomitant RT with BEV in anaplastic glioma is a rare practice. This practice is an extrapolation from managing recurrent high-grade gliomas, particularly the 1205 RTOG trial, which showed improved progression-regression-free survival with the combination of RT and BEV versus BEV alone [12].
Our data showed improvement in ln progression-free survival with the use of BEV. The group with the best oncology results was the group for which both a higher dose was given and a Bevacizumab concomitant treatment with no progression after one year of follow-up.
In addition, an interesting observation was the decreased incidence of RNs using BEV.
With Second RT, one of the significant side effects is RN, which has been reported to rise to 25% for cumulative EQD2 > 130 Gy using an α/β ratio of 2 Gy for a normal healthy brain. The use of BEV has been shown to improve radiation necrosis. A recent meta-analysis reported that radiographic responses were recorded in 84.7% of patients, and clinical improvement was observed in 91% [13].
One limitation of Bevacizumab is its side effects and the chance of increasing surgical complications [14]. In our cohort, most of the patients who received concomitant Bevacizumab did not undergo a second surgery, so perhaps increasing the dose with concomitant Bevacizumab can be more relevant for patients for whom second surgery is not possible.
Strengths and limitations
Our study has several limitations. The rarity of this presentation limited Our sample size. Additionally, the retrospective nature of this study identified only patients with complete clinical and dosimetric data, potentially introducing record bias. The small sample size limited our ability to perform multivariable analysis. Nevertheless, the strength of our study lies in collecting data from multiple hospitals, with thorough reviews of surgical reports and plans. All histopathological data underwent review, and genomic analyses were performed to classify anaplastic meningioma according to the WHO 2021 classification.


留言 (0)