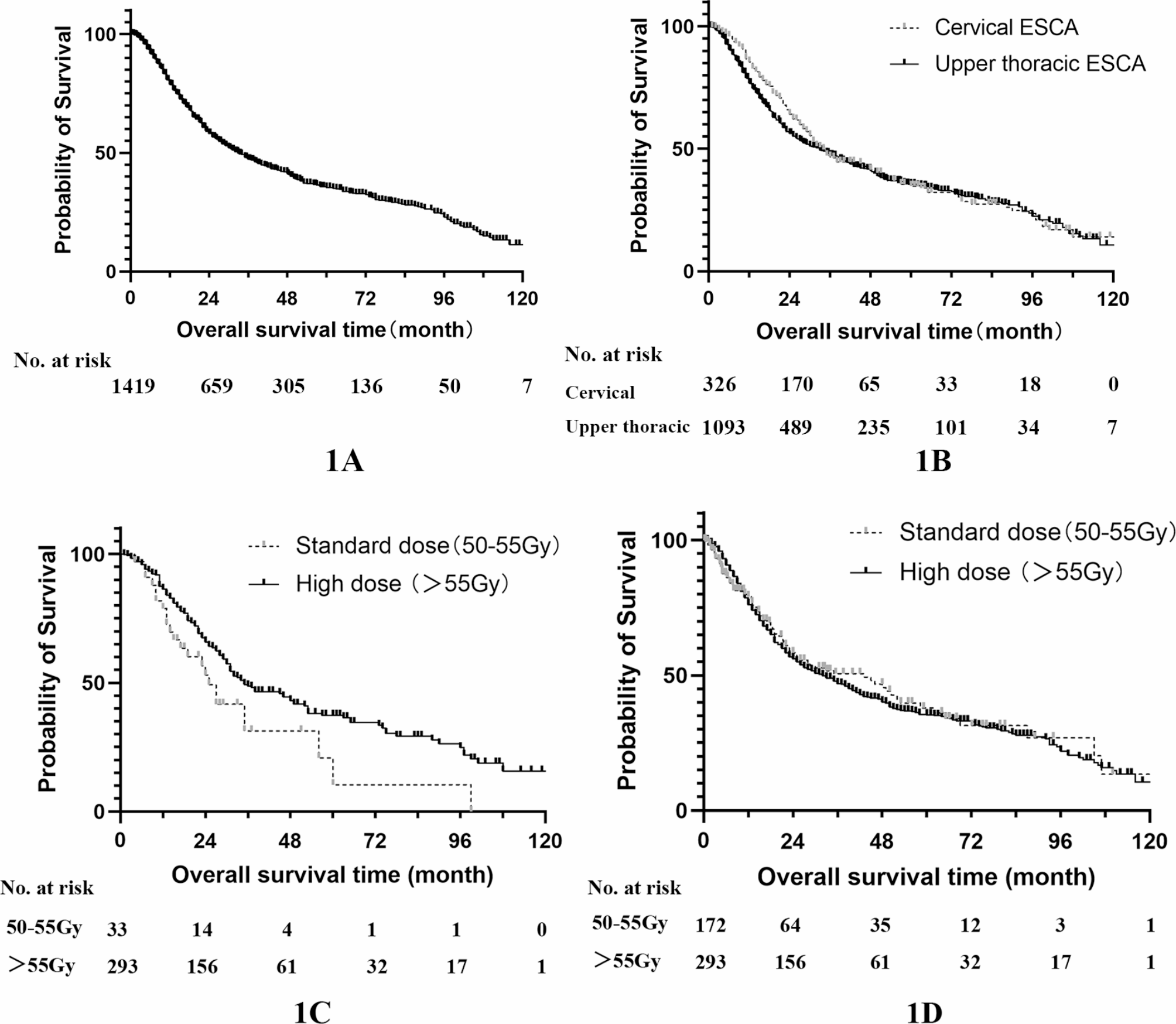
This study gathered real-world data of radical radiotherapy for cervical and upper thoracic ESCA from 6 medical centers in China with the application of 3DCRT/IMRT, exploring the clinical efficacy of radiation dose escalation. The results showed that 3DCRT/IMRT was effective in the treatment of cervical and upper thoracic ESCA, achieving a 3-year OS rate of 47.2% and a 5-year OS rate of 35.3%. The survival outcomes for upper thoracic ESCA were slightly better than those for cervical ESCA, although the difference was not statistically significant. Notably, the 5-year survival rate in this study exceeded that reported in previous two-dimensional radiotherapy studies such as those by Bruce D et al. (3-year OS rates ranged from 25 to 33%) [14] and Shulian W et al. (5-year OS rate was 18.6%) [11], These outcomes were comparable to the data obtained from 3DCRT/IMRT studies, where the 5-year OS rate typically ranged from about 22–40% [8, 21,22,23]. It’s worth highlighting that 78.7% of the patients in this study were diagnosed at stage 3–4, considering the advanced clinical stage of these patients, the survival results in this study were quite promising.
Notably, this study delves into the optimal radiotherapy dose for cervical and upper thoracic ESCA. While the standard radical radiation dose for ESCA is conventionally considered to be 50–50.4 Gy [14], the unique anatomical location and biological characteristics of cervical and upper thoracic ESCA may necessitate different optimal radiotherapy doses compared to other thoracic ESCA cases. Data from the National Cancer Database (NCDB) reveals that 73% of physicians tend to prescribe a radiation dose exceeding 50.4 Gy for cervical ESCA [24], whereas this percentage drops to only 34% for thoracic ESCA [25]. In Asian countries, particularly in China, there is a prevailing trend toward administering higher doses for cervical and upper thoracic ESCA [26, 27], a trend also reflected in this study, where 85.5% of physicians opt for a prescription dose ≥ 55 Gy, with only 14.5% choosing the range of 50–55 Gy. There is a paucity of studies comparing radiotherapy doses in cervical and upper thoracic ESCA, and a dearth of prospective results. The studies conducted by Lachlan J. McDowell and Caineng Cao align with our findings, demonstrating that cervical esophageal cancer patients receiving higher radiotherapy doses (66–70 Gy) exhibited improved survival compared to those receiving conventional doses (50–54 Gy) [19, 28]. Conversely, B. De conducted a review of the National Cancer Database (NCDB) in the United States, which indicated no survival advantage with radiotherapy doses exceeding 50.4 Gy in comparison to doses within the range of 50–50.4 Gy. However, it’s essential to note that the data in this particular study were relatively early, with only a small subset of patients receiving IMRT. Additionally, the baseline characteristics of the patients were not well-balanced. Notably, a more substantial proportion of patients in 50–50.4 Gy group presented with an earlier clinical stage and received chemotherapy compared to >50.4 Gy group. These imbalances may have introduced bias that obscured the impact of high-dose radiotherapy on tumor control [24]. Research for radiation dose escalation in upper thoracic ESCA was even rarer. Given the paucity of high-quality prospective evidence, we embarked on the current study, which stands as the largest investigation to address this question. Our results indicate that, for cervical ESCA, radiation dose>55 Gy outperforms 50–55 Gy, but further dose escalation >63 Gy does not confer a survival advantage. In the case of upper thoracic ESCA, survival outcomes were similar between 50 and 55 Gy and >55 Gy radiotherapy, consistent with the findings observed in the lower two-thirds of the ESCA cohort. However, it is worth noting that >55 Gy radiotherapy was associated with a better ORR. Jiaqi Zhang’s research also suggests that radiation therapy with doses ≥ 60 Gy yields a more favorable Complete Response (CR) and Partial Response (PR) rate [29], aligning with the results of our study. Nevertheless, in the context of upper thoracic ESCA, ORR did not translate into improved survival. This discrepancy may be attributed to the utilization of concurrent chemotherapy, which could potentially mask the local tumor control benefits conferred by radiotherapy.
This study collected data on the impact of different radiotherapy modalities on patients. 3DCRT and IMRTare the two most commonly used radiotherapy techniques today. Previous research has shown that IMRT can provide dosimetric advantages and improvements. These advantages allow for an increased tumor dose while protecting normal tissues [30, 31]. Some studies suggest that IMRT offers significant survival benefits over 3DCRT [32, 33], while others indicate that although IMRT trends towards improved survival, the difference is not statistically significant [34, 35]. Our study showed that the survival advantages of IMRT over 3DCRT did not reach statistical significance. Besides, compared with 3DCRT, IMRT can significantly reduce the probability of radiation pneumonia (P = 0.017) but has no effect on the incidence of radiation esophagitis and myelosuppression (P = 0.328, 0.153). Future studies should balance dose and physical parameters when comparing IMRT and 3DCRT for esophageal cancer.
On the other hand, there is considerable debate regarding the radiotherapy range for ESCA, specifically between ENI and IFI. According to a recent meta-analysis that included 23 studies and 4120 patients, IFI achieved similar survival rates to ENI with significantly reduced side effects [36]. There are few studies comparing ENI and IFI specifically for cervical and upper thoracic esophageal cancer. Jianing Wang’s study showed similar survival times between IFI and ENI. A subgroup analysis based on high or low radiotherapy doses (cut-off: 59.4 Gy) indicated no significant difference in OS between ENI and IFI across different dose groups [37]. Our study results indicate that IFI provides survival outcomes comparable to ENI, suggesting that IFI irradiation may be sufficient for cervical and upper thoracic esophageal cancer. Some studies have shown that some physical parameters, such as primary tumor volume, have prognostic significance for cervical and upper thoracic esophageal cancer [38, 39] Although we included several physical parameters in our study to explore their impact on prognosis, none reached statistical significance in multivariate regression analysis. However, the significant results of primary tumor volume and tumor length in univariate analysis suggest that future research should further explore the interaction between these physical parameters and other clinical variables to establish prognostic models for better diagnostic efficacy.
Chemotherapy stands as one of the most crucial non-surgical treatment modalities for ESCA. The rationale behind combining chemotherapy and radiotherapy lies in its capacity to enhance radiosensitivity through several mechanisms: Chemotherapy can effectively eliminate hypoxic cells, inhibit tumor proliferation, impede sublethal radiation damage repair, ameliorate organ blood supply, and promote reoxygenation [40]. The landmark RTOG 8501 study solidified the role of concurrent chemoradiotherapy, with the cisplatin and 5-fluorouracil (PF) regimen being widely adopted in clinical practice as a first-line recommendation [41]. In China, however, the more prevalent regimen was the combination of paclitaxel and cisplatin (TP). Our study established that the utilization of chemotherapy independently influenced the prognosis for both cervical and upper thoracic ESCA patients. Remarkably, the TP regimen was most commonly administered, which was received by 52.1% patients. Nevertheless, no significant disparity in survival benefits among various chemotherapy regimens, which aligns with the findings from Dashan Ai’s research [42]. The type of chemotherapy regimen (whether single-agent or double-agent), the chemotherapy modality, and the number of chemotherapy cycles (≤ 4 or > 4) did not exhibit a significant impact on OS. Prospective randomized controlled trials and multicenter retrospective analyses have consistently indicated that the efficacy of single-agent chemotherapy does not markedly differ from that of double-agent chemotherapy in the setting of concurrent chemoradiotherapy for ESCA [43, 44]. Consequently, it is suggested that single-agent chemotherapy or a reduction in the number of chemotherapy cycles may be viable options for patients with a compromised general condition who had difficulty tolerating high-intensity chemotherapy regimens.
Recently, programmed cell death protein 1 (PD-1) / programmed death-ligand 1 (PD-L1) immune checkpoint inhibitors have been widely adopted in immunotherapy for multiple malignancies. Nituzumab is an IgG1 monoclonal antibody targeting EGFR, which is commonly applied as a substitution for cetuximab in head and neck malignancy among China, and was utilized in cervical and upper thoracic ESCA in some physicians. An increasing number of evidence indicates that immunotherapy or Nituzumab, along with concurrent chemoradiotherapy, has demonstrated both safety and efficacy in the management of unresectable ESCA [45,46,47,48]. However, this study did not observe a survival benefit associated with immunotherapy or Nituzumab when analyzed using COX univariate analysis. It is important to note that the number of patients receiving immunotherapy or Nituzumab in this study was limited, confounding factors may have existed. Therefore, expanding the sample size is warranted to establish more robust conclusions.
Most studies have shown that with advanced radiotherapy techniques, radiotherapy dose escalation does not significantly increase the probability of treatment-related side effects. Xin Sun’s meta-analysis, which encompassed 10,896 ESCA patients treated with 3DCRT/IMRT, found no increased incidence of grade 3–5 radiation-induced pneumonia, radiation esophagitis, or treatment-related mortality with radiotherapy dose escalation [49]. Similarly, M. Hulshof’s randomized controlled trial (RCT) study indicated that administering higher doses of radiotherapy did not increase the risk of treatment-related side effects when compared to lower doses of radiotherapy [50]. However, the results presented by Y. Xu showed a higher incidence of grade 3 and above radiation-induced pneumonia in the radiotherapy dose escalation group compared to the standard dose group (7.5% vs. 3.1%, P = 0.03) [17]. The results of this study showed that under the condition of 3DCRT/IMRT, high dose radiotherapy did not increase the probability of toxic side effects such as radiation pneumonia and radiation esophagitis. This can be partially explained by the fact that the lung tissue within the target of cervical and upper thoracic ESCA is limited to the region above the azygos vein. As a result, the majority of the lung tissue remains outside the radiation field, and a moderate increase in gross tumor dose does not substantially raise the risk of radiation-induced pneumonia. However, our study does suggest a potential heightened risk of myelosuppression associated with high-dose radiotherapy. Therefore, it is advisable to exercise caution when considering high-dose radiotherapy for patients with a high risk of myelosuppression during chemotherapy.
This study represents the largest investigation of radical radio(chemo)therapy employing 3DCRT/IMRT technology for cervical and upper thoracic ESCA. Given the rarity of this disease, conducting large-scale prospective studies is challenging. This study gathered extensive data from eight medical centers in China, providing a comprehensive representation of Chinese patients with cervical and upper thoracic ESCA with radical radio(chemo)therapy. The outcomes were conducted from a real-world perspective, mainly encompassing considerations of radiotherapy dose escalation, chemotherapy regimens, and associated side effects. While this study was retrospective in nature, the SD group and HD group demonstrated a basic balance in clinical and pathological baseline characteristics, enhancing the objectivity of the results to some extent.
There are, however, some limitations to be acknowledged. Only the radiation dose for the gross tumor was documented, with less detailed information regarding the delineation of target areas like lymphatic drainage regions. Late side effects, including esophageal stenosis, ulcers, and cardiovascular events, were not comprehensively documented. Additionally, due to the absence of recurrence in some patients, progression-free survival could not be analyzed. Moreover, being a retrospective study, it carries inherent potential bias risks, and the research findings would benefit from further validation through prospective studies.


留言 (0)