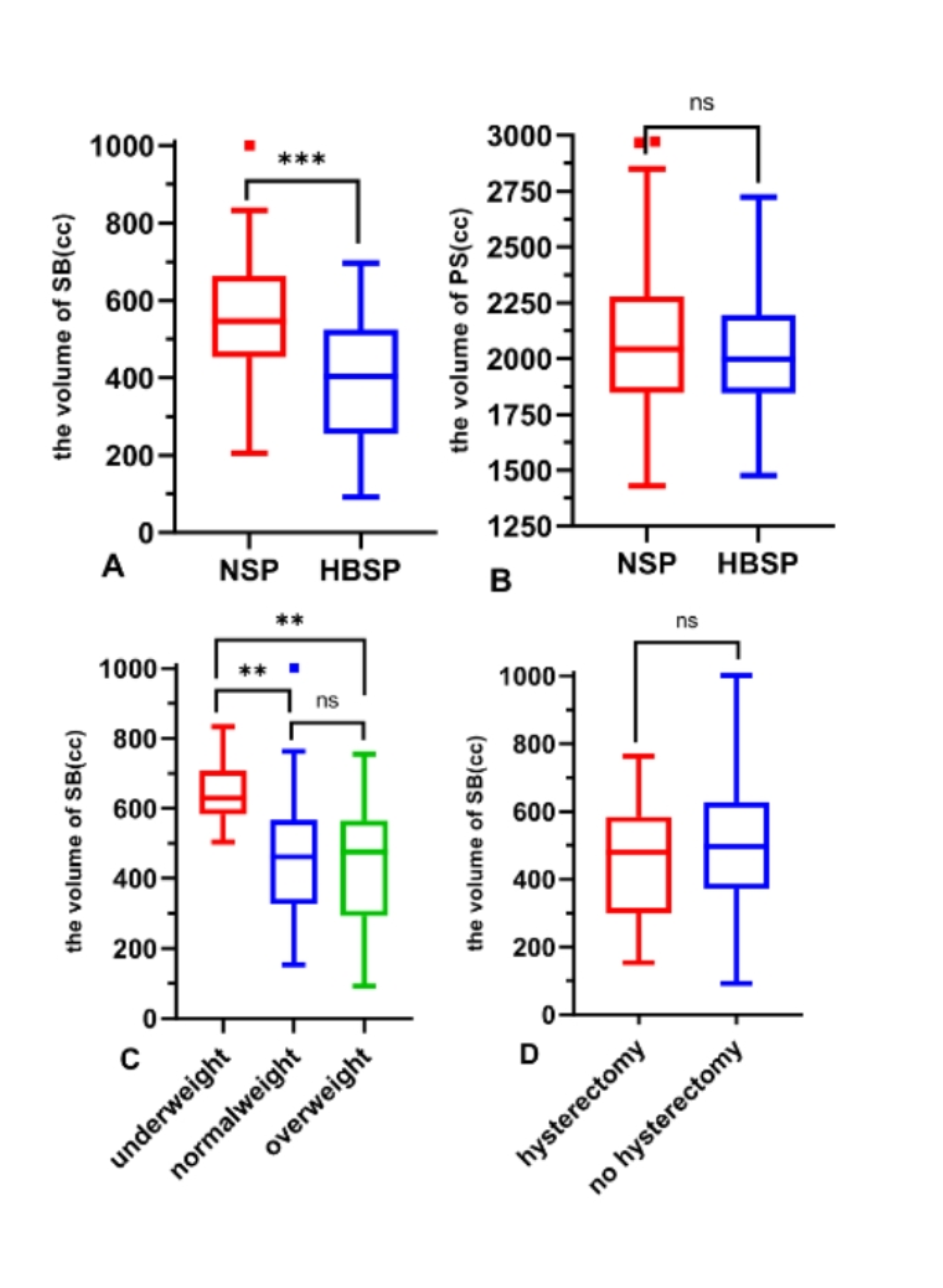
IMRT stands as the primary modality for treating gynecological tumors, offering superior protection for the SB compared to three-dimensional conformal radiation therapy (3D-CRT) [16]. Despite its advantages, the SB remains a limiting organ in terms of radiation dosage during pelvic tumor radiotherapy, posing a challenge for ROs. Our study uncovered that assuming a supine position with elevated buttocks can effectively diminish the volume of SB within the pelvic cavity compared to the standard supine position. In the elevated buttocks position, the average bowel volume is significantly lower than in the normal position. As a result, the irradiated volume of SB also decreased in contrast to the normal position. Noteworthy reductions were observed at each 5 Gy interval (P < 0.05). This study introduces an innovative approach to minimize the irradiated volume of the bowel in the pelvic region across a range of radiation doses.
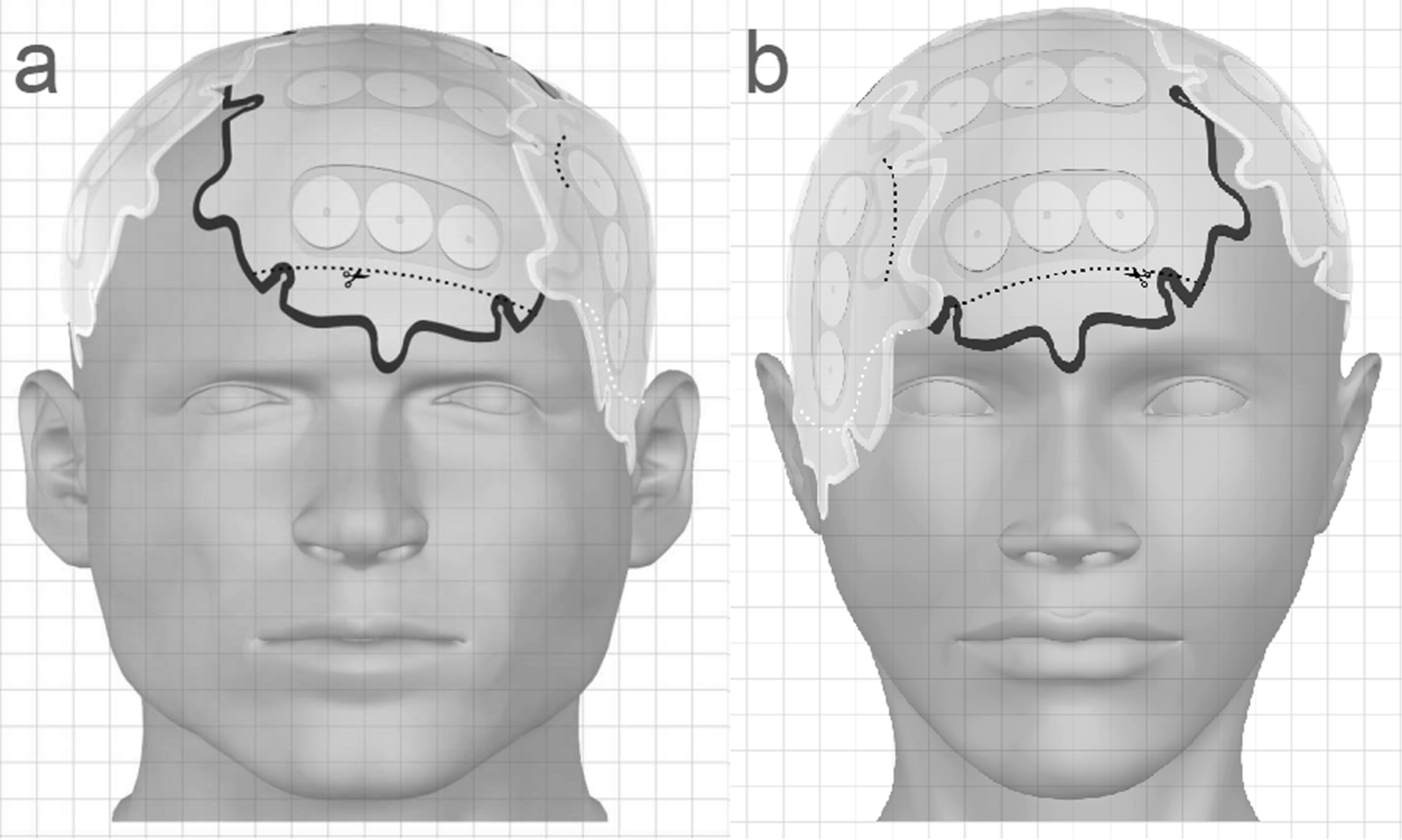
In our study, we harnessed the force of gravity to displace the SB from the pelvic cavity. In the NSP, as patients sat on the therapist’s treatment bed, their pelvic cavity occupied the lowest level in the body, causing the SB to be compressed within the pelvic cavity due to the gravitational effect. To address this issue, patients were instructed to raise their buttocks, elevating the pelvic cavity to a higher position within the body and causing the SB to shift into the upper abdomen. To ensure that the SB remained in its elevated position, a solid foam pad was placed under the sacral tail. The results of our study validated the effectiveness of this approach.
In the realm of radiotherapy, there is a persistent endeavor among ROs to minimize the presence of the SB within the pelvic cavity [8, 10, 17], particularly considering that this area typically receives the highest radiation dose. This objective is paramount in preventing adverse effects associated with high doses of radiation in the pelvic region. However, the current methods employed to achieve this goal, such as invasive techniques and the use of belly boards in prone positions, come with inherent limitations, including discomfort and setup errors. Previous studies have suggested that adopting prone positions with belly boards can effectively reduce the volume of the SB within the treatment field [18,19,20]. For instance, in a study by Olofsen-van Acht et al. [19], it was observed that employing prone positions resulted in a noteworthy 64% reduction in the volume of irradiated SB compared to supine positions. It is essential to recognize that this conclusion was drawn based on the use of orthogonal radiographs, which may not provide accurate estimations of SB volume.
In contrast, conflicting conclusions have been presented in other studies. For example, a study involving rectal cancer patients reported that the median volume of SB in the prone position was higher within the longitudinal PTV extension, measuring 983.5 cm³, compared to the supine position, which measured 806.0 cm³ (p < 0.005) [20]. Martin J et al. [7] also found that the prone position led to a reduction in the volume of SB exposed to high doses of radiation but increased the volume of SB exposed to low doses (≤ 50% isodose). These findings raised concerns regarding setup errors and reproducibility.
In the study conducted by Koeck et al., the utilization of IMRT in conjunction with a prone position was found to effectively reduce the radiation dose received by the SB. However, their findings revealed no significant difference in the mean volume of the SB between the prone and supine positions, with mean volumes of 662.29 ± 189.60 cc and 652.08 ± 163.17 cc, respectively [6]. Similarly, the study conducted by Kim et al. produced analogous results, indicating no statistically significant difference in SB volumes between the prone and supine positions. The mean volumes were 489 ± 211 cc and 521 ± 226 cc, respectively [17]. Notably, all patients included in these studies were diagnosed with rectal cancer, and the irradiated field was relatively smaller compared to that of gynecological tumors. Conversely, Weiss et al. found that while the difference in SB volumes between the supine and prone positions was minimal, the supine position demonstrated better protection for organs at risk, such as the liver and kidneys [21].
The findings from various studies exploring the impact of prone versus supine positions on the irradiated volume of the SB have yielded inconsistent results. Some studies reported a notable decrease in the irradiated SB volume [18], while others did not observe such a significant reduction [22]. This variability might be attributed to discrepancies in the definition of the SB, with some studies delineating individual SB loops and others outlining the perineal cavity. Another factor contributing to these disparities is the potential difference in the volume of the perineal cavity between the prone position with a belly board and the supine position. In the prone position, the perineal cavity volume can be larger [23], leading to the actual SB in the pelvic region moving forward and away from the irradiated zone. Additionally, the placement of the belly board [22] may influence the results. Researchers have explored alternative non-invasive methods to reduce the SB volume within the treatment area. For instance, Muren LP and Nijkamp J et al. [24] discovered that by combining bladder distension with the use of a belly board, the average volume of the SB can be significantly reduced. In clinical practice, it is customary for patients undergoing pelvic tumor radiotherapy to be advised to consume oral fluids and avoid urination before treatment, aiming for bladder distension. The bladder volume significantly influences the size of the SB within the pelvic region, displaying a negative correlation, as supported by our findings in patients positioned supine. We observed a linear correlation coefficient (R) of -0.411 and a P-value of 0.008, indicating a statistically significant negative correlation. However, bladder distension may induce discomfort and a strong urge to urinate, potentially causing involuntary body movements during treatment. Kim TH et al. [25] acknowledged that this approach carries the potential for increased discomfort and setup errors, requiring absolute patient cooperation. While their study demonstrated a 10% reduction in the average volume of the SB, decreasing from 396 cc to 214 cc using different combined methods, it’s noteworthy that their study specifically focused on rectal cancer patients. In our study, in the HBSP group, we observed no significant correlation between the volume of the SB and the bladder volume, as indicated by a linear correlation coefficient (R) of -0.286 and a P-value of 0.091. We hypothesized that the difference between the two groups lies in the HBSP, where gravitational forces may shift the SB from the pelvic cavity to the upper abdomen. Consequently, the SB is no longer in close proximity to the bladder. Based on these findings, we can conclude that patients with pelvic tumors undergoing radiotherapy in the high buttocks supine position may not necessarily need to retain urine to distend the bladder. Patients can maintain a natural position during radiotherapy, potentially reducing setup errors and minimizing body movement during treatment, thereby helping to decrease significant inter-fractional errors.
Various factors can impact the volume of the SB in the pelvic region, including BMI and surgical procedures. In our study, we meticulously considered these factors and categorized patients into three groups. Our findings affirm the correlation between BMI and the volume of SB in the pelvic region, with underweight patients exhibiting a larger volume. This phenomenon may be attributed to enteritis and inflammation in the perineal area, resulting in reduced absorption and a smaller volume of the great omentum, subsequently leading to weaker peristaltic movement. The influence of surgery in our study was relatively constrained, diverging from prior research. This discrepancy could be attributed to advancements in surgical techniques that effectively minimize bleeding and harm to the peritoneum.
Our study is subject to certain limitations that warrant acknowledgment. Owing to financial constraints, all patients underwent treatment in a single position, thereby restricting our capacity to compare two positions within the same patient. A more informative approach would have involved assessing two plans in two positions, allowing us to examine the optimal placement of the solid foam and determine the degree to which patients should raise their buttocks. Additionally, implementing the HBSP demands effective cooperation between patients and radiation therapists; therefore, an auxiliary device should be designed to better assist patients during the procedure.


留言 (0)