Study design
This prospective study employed a correlation and concordance analysis approach, aiming to assess the reliability of non-invasive methods for measuring CO in critically ill patients. Conducted at Fundación Valle del Lili in Cali, Colombia, a tertiary care center renowned for its expertise in critical care and advanced diagnostic capabilities.
Population and sample
A non-probabilistic quota sampling method was employed to determine the sample size, enrolling 49 critically ill patients aged 18 years and above, who required invasive CO measurement during their ICU stay. Invasive monitoring systems such as Swan-Ganz catheters, PiCCO and EV-1000 systems were utilized for CO measurement. Patients with active arrhythmias, severe mitral or aortic valve disease, pregnancy, or inadequate acoustic window for carotid Doppler assessment were excluded from the study.
Operational aspects
Eligible patients underwent evaluation in the ICU, where an external observer recorded general data and CO measurements obtained via invasive methods. Following this, an independent observer, blinded by the invasive CO results, conducted the US assessments. These measurements were carried out by three US experienced physicians with varying levels of expertise including an emergency medicine resident, a junior emergency physician, and an emergency physician specializing in intensive care and radiology. Each patient was examined by one of the three physicians.
The measurements were performed at predetermined times during the patients’ ICU stay, after invasive CO measurements were conducted. All patients underwent both echocardiography and carotid ultrasound measurements. Each ultrasound measurement was taken as an average of 3 to 5 consecutive heartbeats.
Utilizing a high-frequency linear transducer, the common carotid artery (CCA) was identified bilaterally in both transverse and longitudinal planes using grayscale ultrasound. Subsequently, spectral waveforms of blood flow velocity within the proximal CCA were captured using pulse wave Doppler, with precise placement of the sample volume approximately 1–2 cm below the carotid bulb. Doppler angle adjustment was optimized to approach 0 °. The obtained variables included carotid artery diameter, systo-diastolic time average peak (TAP) velocities, systolic TAP velocities, systo-diastolic flow, and systolic flow.
For the estimation of cardiac output through echocardiography, a phased-array transducer was employed. The parasternal long-axis window was utilized to measure the LVOT diameter, and the apical five-chamber view was employed to capture the VTI of blood flow through the LVOT using pulse wave Doppler. LVOT VTI measurements were conducted both with and without angle correction.
Statistical analysis
An exploratory analysis of the data was conducted, along with an assessment of data quality through a randomized probabilistic sampling of 10% of the records to ensure consistency and accuracy. Univariate analysis was employed to assess the distribution of numerical variables using the Shapiro–Wilk test, with results summarized as mean ± standard deviation (SD) or median ± interquartile ranges (IQR) as appropriate. Categorical variables were presented as absolute numbers (n) and relative frequencies (%).
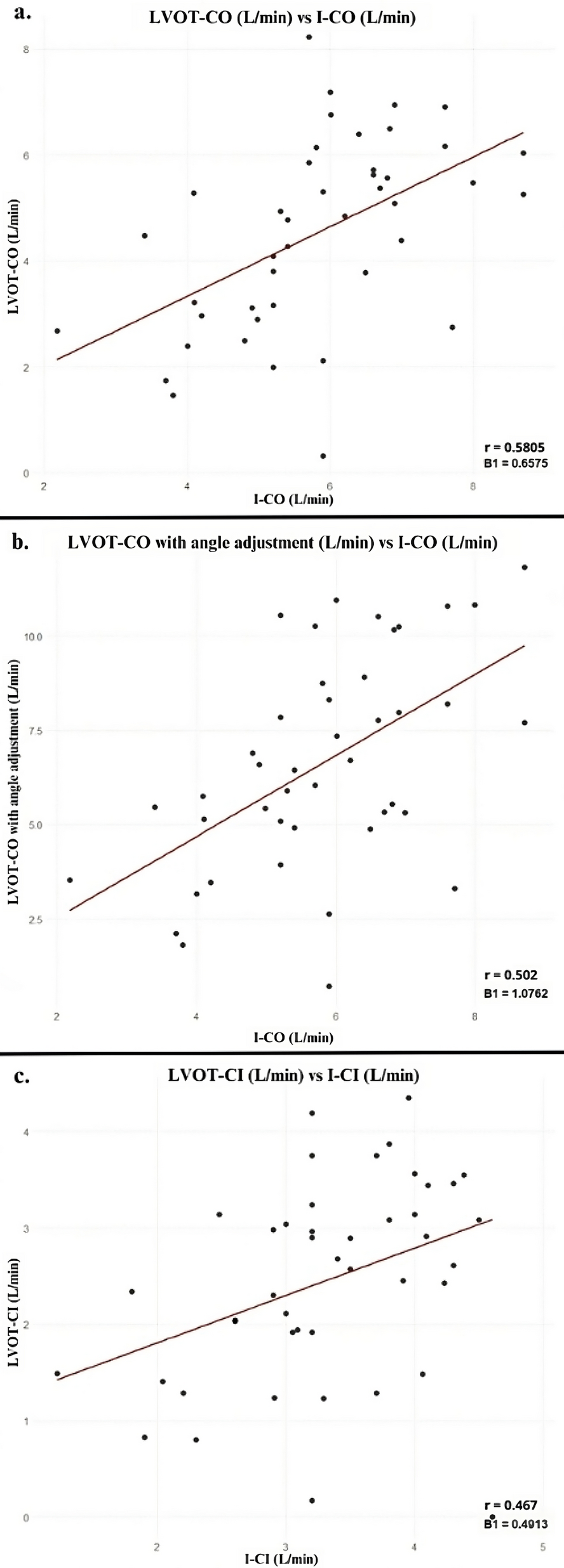
The comparison between right and left carotid Doppler ultrasound measurements was conducted using the Wilcoxon signed-rank test. Correlation analysis between CO, cardiac index (CI), and systo-diastolic flow obtained via echocardiography and carotid Doppler ultrasound was performed using the Spearman coefficient, with all invasive CO measurement as the reference standard for comparison. Correlation coefficients falling within the ranges of 0.00–0.09 were considered negligible, 0.10–0.39 weak, 0.40–0.69 moderate, 0.70–0.89 strong, and 0.90–1.00 very strong [21].
Concordance analysis between CO and CI was assessed using the intraclass correlation coefficient (ICC), with all invasive CO measurement serving as the reference standard. ICC values below 0.5 indicated poor reliability, those between 0.5 and 0.75 indicated moderate reliability, those between 0.75 and 0.9 indicated good reliability, and those exceeding 0.90 indicate excellent reliability [22].
Statistical significance was defined as a p-value < 0.05. All statistical analyses were performed using Stata version 14 (StataCorp LP, College Station, TX).
Ethical considerations
Approval for this study was obtained from the ethics committee of Fundación Valle del Lili, adhering to international recommendations regarding research involving human subjects, including compliance with the Nuremberg Code, the Helsinki Declaration, and the guidelines of the CIOMS. Patient confidentiality was rigorously maintained and individuals were afforded the right to decline participation without any repercussions on their medical treatment.



留言 (0)