
記住我
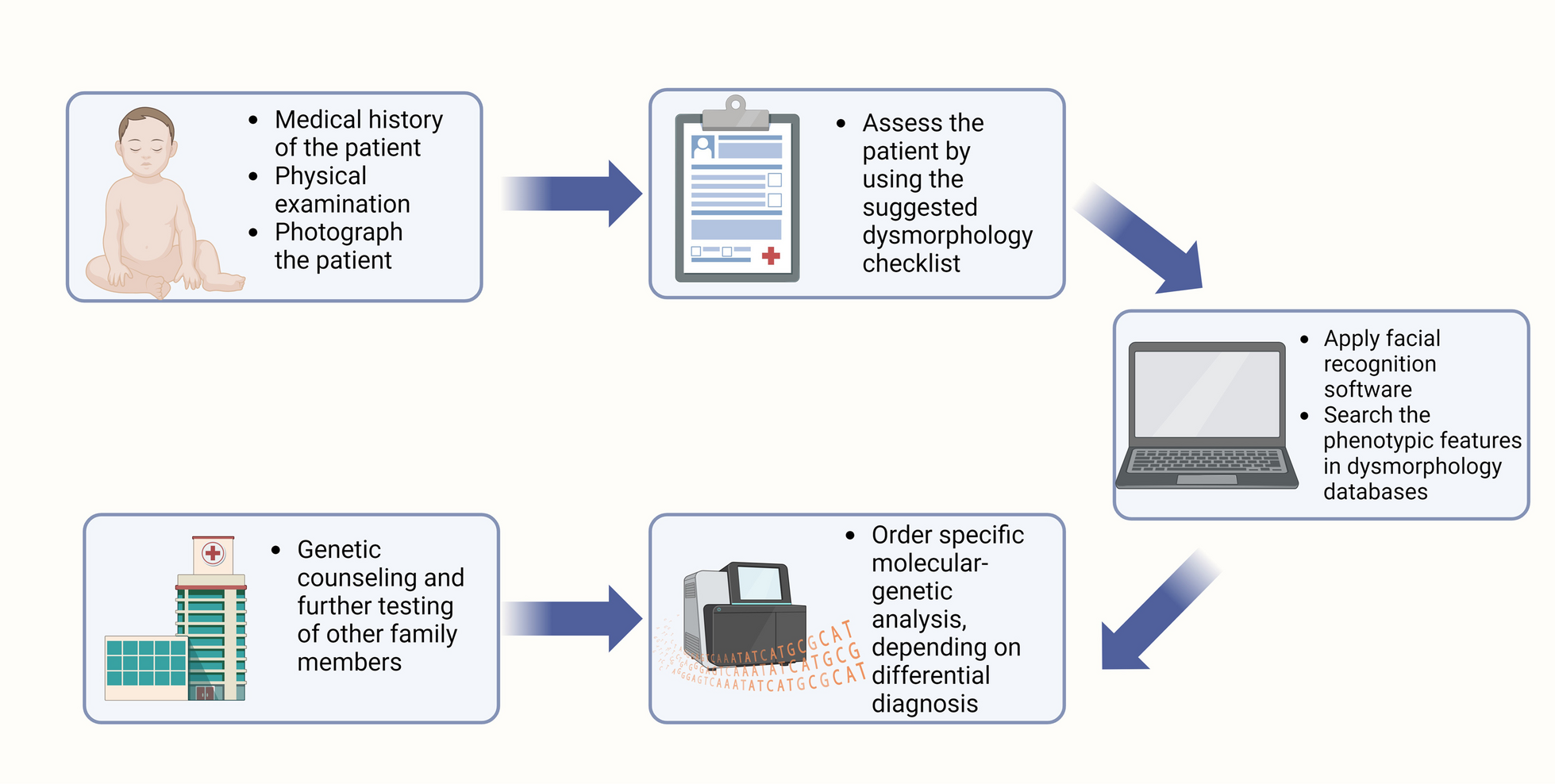
The four steps of the suggested algorithm are listed below (Fig. 1):
Fig. 1
A step-by-step cost-efficient algorithm for diagnosing children with dysmorphic features, based on our current experience. Created in Biorender
First step: medical history of the patient, physical examination by using a dysmorphology checklistThe ability to correctly diagnose a syndrome rests on a thorough medical history and a physical examination of the patient. It is important to investigate the medical history of the mother during the pregnancy in order to exclude a teratogenic factor in the etiology of the patient’s condition. The family history, the mechanism of birth, any complications after that, and the postnatal development of the child are all important in order to explore the medical history of the patient in order to rule out any environmental factors. The training and experience of the dysmorphologist, who performs the physical examination, are essential in the process of determining the patient's genetic condition because one symptom could be a phenotypic sign of an underlying genetic syndrome [2, 3]. For example, micrognathia, together with a cleft palate and glossoptosis, comprise the so-called Pierre Robin sequence. This could be an isolated finding. However, in 18–30% of all cases, this sequence is part of the clinical presentation of Stickler’s syndrome [8]. As patients with Stickler syndrome may have vision and hearing problems, it is important to recognize this underlying condition in order to provide immediate medical care [8].
In order to address different aspects of the phenotype, we have developed a dysmorphology checklist (Suppl. Table 1). It provides a systematic approach when working with patients with malformations and reduces the chance of overlooking a certain phenotypic feature of the patient. The dysmorphology checklist is an effective tool that provides a good organization of the physical examination of patients with dysmorphic features. It is divided into different sections, each corresponding to certain body parts. The listed dysmorphic features are some of the most common. However, there are many other phenotypic features which could be present in the patient and could be filled in additionally by the examiner. The dysmorphology checklist improves the precision of the terminology used to describe specific clinical characteristics, as sometimes the exact terms can be difficult to remember. Therefore, the use of the suggested checklist would be a good addition to everyday practice. Additionally, it is essential to document the patient's physical and behavioral phenotypes because they may be entered into various dysmorphology databases in the next steps.
Second step: search for a matching diagnosis in dysmorphology databases based on the phenotype and apply facial recognition softwareSearching through databases with information on genes and phenotypes may be very useful when counseling individuals with specific dysmorphic traits and challenging genetic disorders to diagnose. There are several genetic databases that may be helpful, and some of them can be accessed for free, while others require payment in order to search them [9, 10]. Comprehensive information regarding multiple rare disorders and the corresponding genes can be found at Online Mendelian Inheritance in Man (OMIM) [11] and ORPHA.NET [12]. They are both freely accessible. Other computer applications can be used to enter the patient's phenotypic characteristics and look for an appropriate diagnosis. These include London Medical Database [13], POSSUM [14], PHENOMIZER [15], PubCaseFinder [16], Monarch Initiative [17], and FaceBase [18].The first two on the list, though, demand a subscription. The requirement for a full description of the patient's phenotype, which can occasionally be difficult even for highly skilled clinical geneticists, is one of the drawbacks of such programs. Therefore, any bias in the diagnosing process might be eliminated by using face recognition software. Face2Gene, created by Facial Dysmorphology Novel Analysis (FDNA Inc., Boston, Massachusetts, USA), is one of the most well-known face recognition programs [19]. All users have free access to it, but they must confirm that they are employed in the health care sector [10]. Face2Gene analyzes the uploaded photographs of patients with dysmorphic characteristics using a two-dimensional approach. It begins by detecting facial landmarks, then moves on to detecting facial subregions (Fig. 2). It uses a deep convolutional neural network to obtain information for the specific traits in the different subregions and integrates all the data in order to create the so-called gestalt or face [9, 10]. Face2Gene was demonstrated in a clinical setting to be highly efficient. The program successfully suggested the diagnosis of Cornelia de Lange as a first prediction in 83.7% of 49 patients with pathogenic variants in genes associated with this syndrome [20, 21]. Other research teams also found the program to be effective and highly useful for daily practice [9, 22, 23]. Therefore, it is important to take a photograph of the patient after they or their parents have provided consent and upload it to such specific dysmorphology programs. Also, this photograph could be attached to the patient’s file and later be helpful for the clinician to re-examine the observed dysmorphic features. The use of 3D facial photographs for morphological study is also becoming increasingly popular [24]. Moreover, the photograph could be used to discuss the clinical case with fellow dysmorphologists. The face recognition software cannot replace the highly experienced clinical dysmorphologist, but it could support the clinician by enhancing diagnostic capacity.
Fig. 2
A flow chart illustrating the application of Face2Gene in the clinical practice
Third step: ordering the molecular-genetic analysisAdvances in genetic technology are having a major impact on modern medical practice. Current molecular-genetic testing, which is now widely available, has transformed the detection of genetic diseases, including syndromes presenting with dysmorphic features [25]. There is not a single genetic test that can rule out every potential cause of genetic diseases, though. One test may be more appropriate than another, depending on the type of dysmorphic traits present and the differential diagnosis. As a result, it is critical to suggest the best test in order to save both time and resources, as in certain countries, patients are responsible for paying for this type of testing [6, 7]. The ordering dysmorphologist must therefore be informed of the diagnostic resolution, advantages, and disadvantages of the particular molecular-genetic tests in order to select the most appropriate test and reduce the need for additional testing (Table 1). Cytogenetic analysis, fluorescent in situ hybridization (FISH), and array—comparative genomic hybridization (array—CGH) can all be used for the detection of numerical and structural chromosomal aberrations [26, 27]. However, ordering cytogenetic analysis would be the most cost-effective initial choice of testing if there are specific phenotypic symptoms of a numerical chromosomal disorder, such as Patau syndrome, as it is typically caused by full trisomy 13 [28]. In the case of a suspected microdeletion or microduplication syndrome, the first choice of testing should be array—CGH as it detects such small aberrations in all 46 chromosomes, unlike FISH, which searches for aberrations in particular regions and might require further testing for other chromosomal regions. As for sequencing, targeted sequencing is the most cost-efficient choice, and in the case of phenotypic features of a certain single gene disorder, it should be the primary choice [29]. Whole-genome sequencing is recommended by the ACMGG as the first tier of testing for children with ID and dysmorphic features [4]. However, they are expensive tests, which limits their utilization in some countries [6, 7, 21].
Table 1 Characteristics of the today’s most frequently used genetic testsFourth step: genetic counseling and further testingThe process of medical genetic counseling has been defined as a “process of helping people understand and adapt to the medical, psychological, and familial implications of genetic contributions to disease” [30]. The genetic counselor is expected to give further details about the disorder itself, the type of inheritance, the risk of occurrence, management, and prevention of the disorder during the genetic counseling session [30]. Additionally, the medical genetic counselor should help the patients cope emotionally with the upsetting news. This has led to the definition of genetic counseling as a form of psychotherapy [31, 32].
Due to the higher diagnostic yield of the molecular-genetic tests, the number of people who suffer from rare diseases has increased [33]. More noninfectious diseases, such as genetic disorders, are predicted to cause deaths in the near future, especially in some African regions [34]. This emphasizes the significance of identifying the dysmorphic traits associated with different genetic disorders. As a large portion of the affected patients are minors, it also highlights the necessity of defining criteria for carrier testing and ethical standards [35]. The clinician should postpone testing of children who are at risk of developing a late-onset genetic condition, such as siblings, in accordance with the current recommendations until the children are capable of giving consent in an informed manner [35].
A case example from our clinical practiceOur patient was a 12-year-old boy, born per C section after a second pregnancy. He was referred to us because of a delay in his neuropsychological development. Additional symptoms were obesity, hypertension, interseptal defect, mitral valve dysplasia, bilateral inguinal cryptorchidism, leukoma of the right eye, and bilateral exophthalmos. By applying the suggested dysmorphology checklist, the following dysmorphic features were described: downslanting palpebral fissures, highly arched eyebrows, sparse lateral eyebrows, prominent eyelashes, strabismus, wide nasal bridge, broad nasal tip, and long philtrum. A frontal photograph, together with the phenotypic features of the patient, was uploaded to Face2Gene. The first suggested syndrome was Kabuki syndrome (Fig. 3). Targeted sequencing of the KMT2D and KDM6A genes showed a heterozygous pathogenic variant c.12028delT in the KMT2D gene, thus confirming the Kabuki syndrome.
Fig. 3
A case study example of a patient with Kabuki syndrome, whose picture was uploaded and analyzed by Face2Gene software
留言 (0)