
記住我


To investigate the potentially causal associations between lipid-lowering drug classes and sarcopenia, we carried out a drug target MR study. In order to ensure the reliability of genetic variants as instrumental variables (IVs), three fundamental conditions in MR analysis must be satisfied. Firstly, the IVs should exhibit robust and consistent associations with the targeted exposure; secondly, these IVs must not be correlated with any potential confounders that could bias the exposure or outcome; and lastly, the IVs should exclusively influence the outcome through their direct impact on the exposure, while avoiding alternative pathways or external influences [13]. The data utilized in the present study were obtained from publicly accessible repositories. Ethical approval and informed consent were previously acquired in the original genome-wide association study (GWAS).
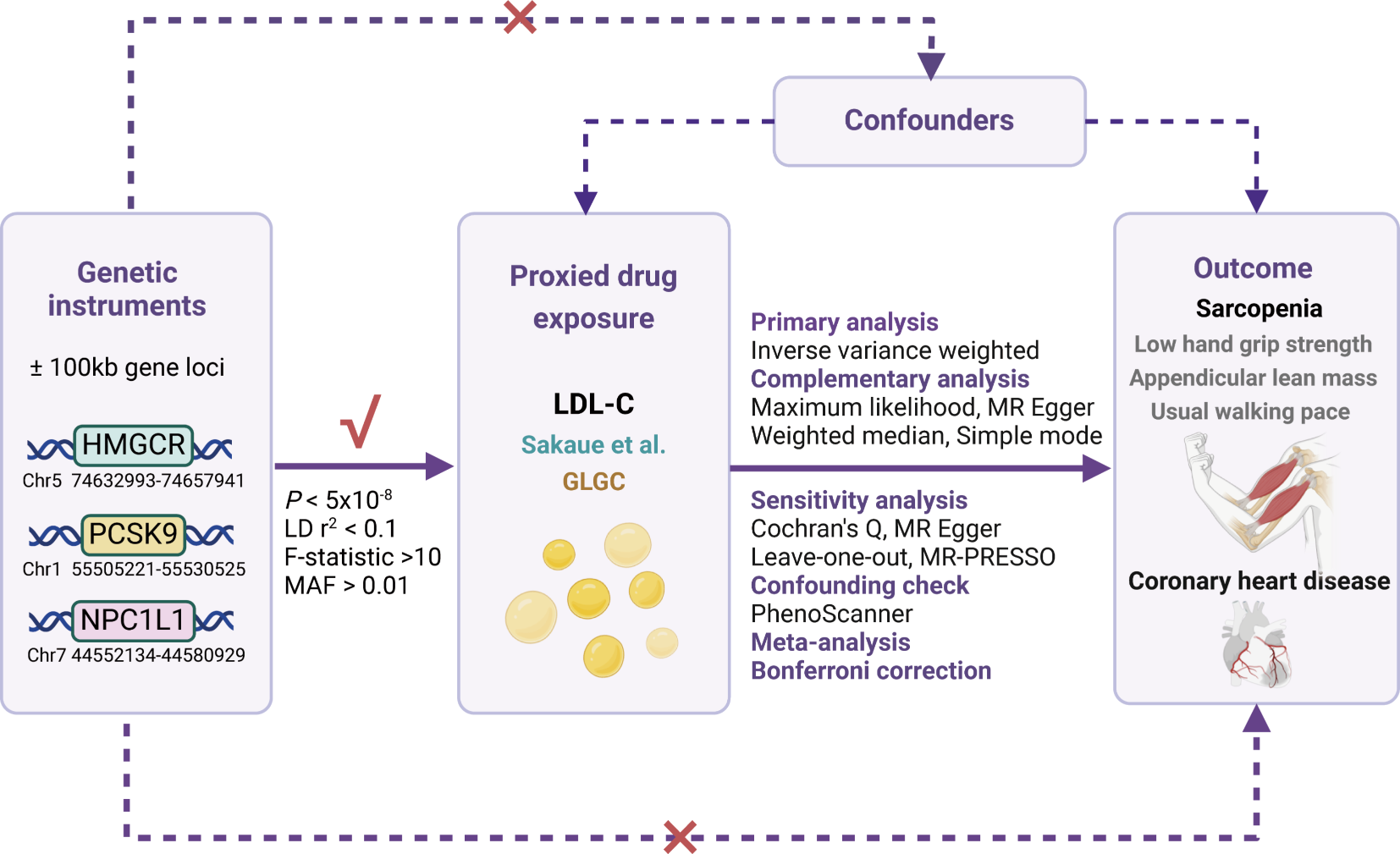
Selection of IVs for lipid-lowering drug effectThe primary MR analysis leveraged summary-level dataset on LDL-C to proxy lipid-lowering drug exposure from a GWAS conducted by Sakaue et al., encompassing 416,487 individuals, primarily of European ancestry (343,621 Europeans and 72,866 East Asians). The dataset included 19,037,976 single nucleotide polymorphisms (SNPs) predominantly sourced from the UK Biobank [14]. To proxy the LDL-C lowering effects of HMGCR, PCSK9, and NCP1L1 inhibitions, we identified IVs based on the following criteria. These IVs were strategically selected SNPs located within a range of ± 100 kb from the genetic loci of HMGCR (Chromosome 5, 74,632,993–74,657,941), PCSK9 (Chromosome 1, 55,505,221–55,530,525), and NCP1L1 (Chromosome 7, 44,552,134–44,580,929) genes, exhibiting a statistically significant association with LDL-C levels (P < 5 × 10− 8) (Fig. 1 displays the overview of the study). In order to mitigate potential biases resulting from strong linkage disequilibrium (LD), we implemented an LD threshold of r2 < 0.1. The minimum minor allele frequency threshold of IVs was set as > 0.01. All SNPs designated as IVs in this study possessed a minimum F-statistic of 10 to counteract the potential influence of weak genetic instruments. Finally, a total of 9, 20, and 2 SNPs within the HMGCR, PCSK9, and NPC1L1 gene regions were selected, respectively. Additionally, for further validation, we utilized another summary-level GWAS dataset on LDL-C levels sourced from the Global Lipids Genetics Consortium (GLGC), encompassing 173,082 individuals of European ancestry with 2,437,752 SNPs [15]. We repeated the process outlined above to derive IVs to proxy the inhibitions of HMGCR, PCSK9, and NCP1L1 genes. A total of 2, 10, and 2 SNPs associated with LDL-C lowering within the HMGCR, PCSK9, and NPC1L1 gene regions were selected, respectively. Since both the primary and validation MR analyses included 2 SNPs to proxy NPC1L1 gene inhibition, we conducted an additional analysis with an LD threshold of r2 < 0.3 to enhance the robustness of our results. This led to the identification of 4 SNPs from the Sakaue et al. dataset and 3 SNPs from the GLGC dataset for subsequent causal estimations. Detailed information of IVs from LDL-C datasets is presented in the Supplementary Table S1-2.
Fig. 1
Study design overview. HMGCR, 3-hydroxy-3-methylglutaryl coenzyme A reductase; PCSK9, proprotein convertase subtilisin/kexin type 9; NPC1L1, Niemann-Pick C1-like 1; Chr, chromosome; LD, linkage disequilibrium; MAF, minor allele frequency; LDL-C, low-density lipoprotein cholesterol; GLGC, Global Lipids Genetics Consortium; MR-PRESSO, Mendelian randomization pleiotropy residual sum and outlier
Source of outcomesIn our present MR analysis, according to the diagnostic recommendation of sarcopenia provided by the European Working Group on Sarcopenia in Older People (EWGSOP), we considered three sarcopenia-related traits as the outcomes, namely the low hand grip strength (60 years and older), appendicular lean mass, and usual walking pace. The summary-level GWAS dataset for low hand grip strength was sourced from the study conducted by Jones et al., encompassing data from 256,523 European participants with 9,336,415 SNPs across 22 cohorts [16]. The low hand grip strength was defined as grip strength < 30 kg for males and < 20 kg for females, which was measured using a hydraulic hand dynamometer in accordance with the diagnostic recommendation of EWGSOP. The GWAS dataset for appendicular lean mass was extracted from Pei et al.'s study, which included 450,243 European participants and 18,071,518 SNPs [17]. Appendicular lean mass representing the quantity of muscle, was defined as the summation of fat-free mass of arms and legs measured through bioelectrical impedance analysis. Appendicular lean mass raw values for all eligible participants were adjusted by appendicular fat mass, age, age squared, assessment center, and genotyping array. Appendicular lean mass is widely-recognized as a reliable metric for the approximation of muscle mass quantity in sarcopenia research [18]. According to the diagnostic guidelines proposed by EWGSOP, appendicular lean mass values below 20 kg for males and 15 kg for females are indicative of sarcopenia [19]. The GWAS dataset for usual walking pace, serving as an indicator of muscle function, was obtained from the European participants utilizing a linear model encompassing self-reported data of walking speed including slow (less than 3 miles per hour), steady (ranging from 3 to 4 miles per hour), and brisk (over 4 miles per hour) paces. The cut-off speed lower than 0.8 m per second (equivalent to 1.79 miles per hour) is advised by EWGSOP as an indicator of severe sarcopenia [19]. This dataset consisted of genetic information from 459,915 individuals and comprised a total of 9,851,867 SNPs.
Moreover, we additionally used a GWAS dataset on coronary heart disease (CHD) [20] from the European ancestry as the positive control, demonstrating the effectiveness of proxied LDL-C lowering through drug target genes inhibitions in MR analysis. A summary of the GWAS datasets utilized in the study is presented in Supplementary Table S3.
Data analysis and statisticsAfter harmonizing the selected IVs with the datasets of sarcopenia-related traits and excepting palindromic SNPs with intermediate allele frequencies, a drug target MR analysis was performed. We primarily employed the inverse-variance weighted (IVW) method, which has been widely recognized as the most powerful approach in MR analysis [21], to investigate the potential causative links between proxied LDL-C lowering drug exposure and sarcopenia-related traits. When there was heterogeneity among IVs, the IVW-multiplicative random effects model may be used. Otherwise, IVW-fixed effects model would be applied. Additionally, we incorporated several complementary methods, including MR Egger, weighted median, maximum likelihood, and simple mode. MR Egger is suitable for causal estimation when pleiotropy among IVs is present. Weighted median infers the causality by considering the weights of SNP-specific estimates, ensuring robustness in case of limited number of valid IVs. Maximum likelihood estimation addresses bias stemming from sample overlap, while simple mode offers unweighted mode of the empirical density function of causal estimates [22, 23]. All statistical computations were conducted using the “TwoSampleMR” (Version 0.5.7) and “MRInstruments” (Version 0.3.2) packages within RStudio (Version 2023.06.0). For each standard deviation decrease in LDL-C levels, the odds ratio (OR) indicates the risk of categorical outcomes (low hand grip strength, usual walking pace), while the beta coefficient quantifies the number of standard deviation changes of the continuous outcome (appendicular lean mass in kilogram). After applying the Bonferroni multiple testing correction for genetically proxied drug exposure and sarcopenia-related traits, we established a significance threshold for a P-value below 5.56 × 10− 3 (P = 0.05/9) to indicate significant evidence of a causal association.
Sensitivity analysisTo gauge the degree of heterogeneity within the IVs, we employed Cochran’s Q test. MR Egger regression was used to test the possibility of horizontal pleiotropy among the IVs [24]. Heterogeneity and pleiotropy were taken into account with a P-value below 0.05. The online tool PhenoScanner was used to thoroughly examine all IVs, ensuring that all selected IVs for MR analysis were not associated with confounding factors (such as smoking, alcohol use, physical activity, body weight, body mass index, etc.). No SNP was removed in this step. To minimize the potential influence of each SNP on the overall results, the MR pleiotropy residual sum and outlier (MR-PRESSO) as well as leave-one-out analysis was utilized to identify potential outliers among the IVs [24, 25]. In instances where an SNP outlier was detected via MR-PRESSO or leave-one-out, the outlier should be excluded. The MR analysis may be subsequently reiterated to derive the ultimate robust outcomes. The detailed information of excluded SNPs is presented in Supplementary Table S4.
As the outcome GWAS datasets of appendicular lean mass and usual walking pace were predominantly sourced from participants of the UK Biobank, we took into account the influence of sample overlap when conducting MR analysis using LDL-C from the GWAS of Sakaue et al. to proxy lipid-lowering drug exposure. To ensure the reliability of the results, we utilized the “mrSampleOverlap” (Version 0.1.1) package within RStudio to estimate the bias caused by sample overlap and the probability of Type 1 error [26].
Meta-analysisAdditionally, to provide a more comprehensive interpretation of the above findings. we conducted a meta-analysis by merging the IVW causal estimates using LDL-C from Sakaue et al., as well as GLGC to proxy the lipid-lowering drug exposure of HMGCR, PCSK9, and NCP1L1 inhibitions on sarcopenia-related traits through the Review Manager software (Version 5.3).
留言 (0)