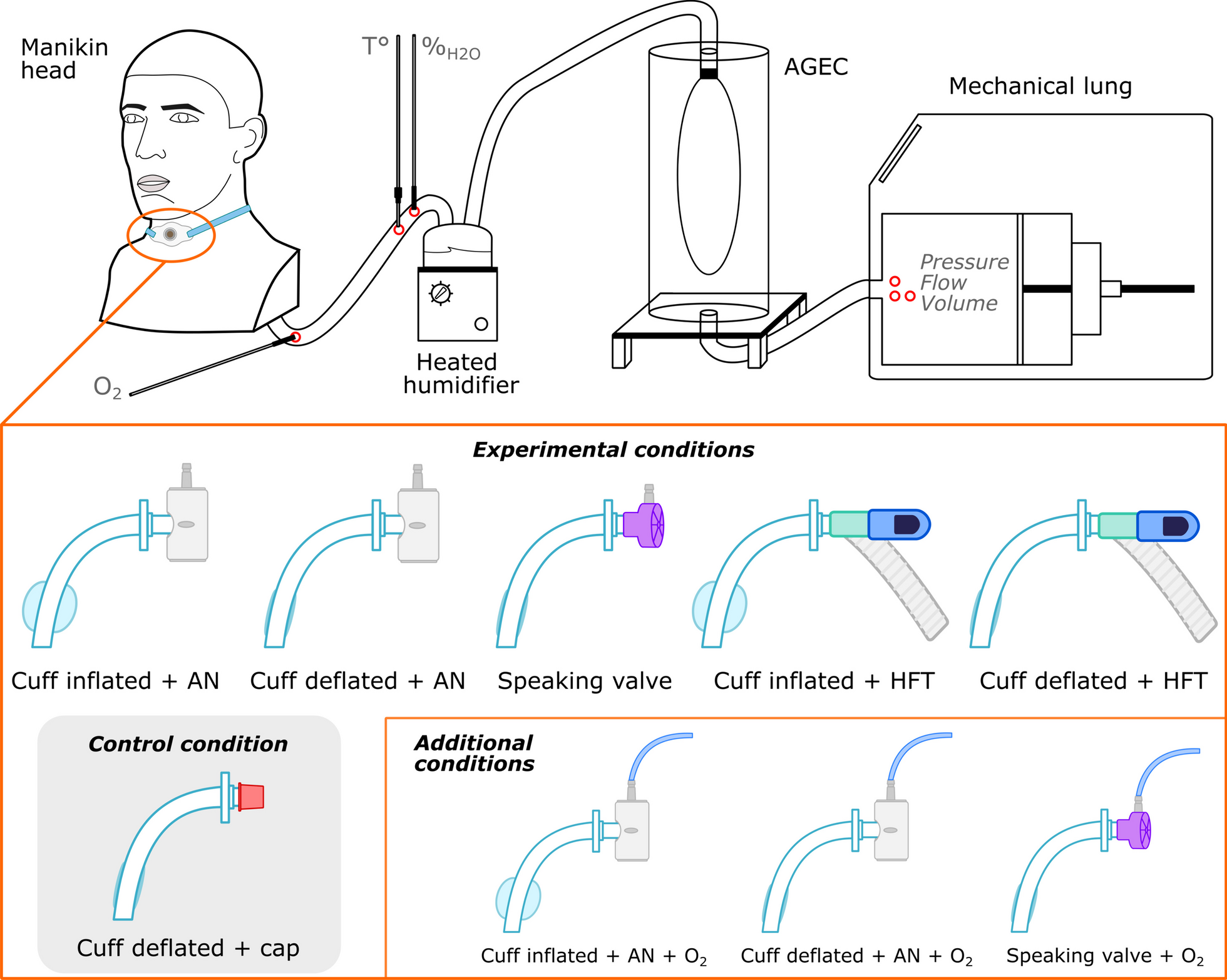
This bench study provided the following observations: (i) in the normal and restrictive models, conditions with an inflated cuff led to a slight increase in ventilatory work compared to the capping condition which is the last step on the decannulation pathway [15]. However, in the obstructive model, ventilatory work was minimally increased by the cuff deflated conditions. (ii) Adding HFT to a cuff-inflated tracheostomy tube increased PEEPtot by up to 1 cmH2O compared to the capping condition. (iii) Across all pulmonary models, the inflated cuff resulted in a reduction in VT by up to − 57 mL per breath.
In our experimental conditions, the observed results strengthen the rationale for cuff deflation. The differences observed on the WOB compared to cannula capping, although sometimes statistically significant, appear clinically minimal and may not discourage cuff deflation considering the other benefits (e.g., improved swallowing or phonation) expected. The only exception was noted in the obstructive lung model, with an increase in WOB occurring with cuff deflation. One explanation could be that the decrease in expiratory resistance while the cuff is inflated in such circumstance might be beneficial for patients with obstructive diseases [16, 17]. However, it is important to note that our model does not replicate vocal cords and their physiological impact on patient respiratory mechanics. In addition, numerous clinical arguments support cuff deflation and the use of the speaking valve to facilitate expectoration, swallowing, and lung recruitment [1, 2, 7, 9,10,11,12].
Interestingly, the use of HFT did not produce the expected effects on WOB or the generation of PEEPtot. The clinical hypotheses were that HFT could serve as a substitute for mechanical ventilation by reducing WOB, maintaining PEEP effects, and increasing VT [18, 19]. However, our results do not corroborate these hypotheses, with minimal PEEP effects (+ 1 cmH2O at best) and decreased VT. Nevertheless, our results indicate that HFT provides the best humidification and the highest temperature, while the speaking valve significantly reduces relative humidity. These findings are further accentuated when oxygen is added. Indeed, the mechanism of oxygen administration on the speaking valve traps oxygen behind the one-way membrane and exacerbates the drying of inspired gases. These results are confirmed by the differences in FiO2 found for the same flow rate, with FiO2 of 46% 95% CI (42.5–49.5) for 2 L/min of O2.
Our study had several limitations, including the lack of air warming and humidification typically provided by the upper airway mucosa, notably the nasal turbinates. This could have potentially affected our findings related to relative humidity in conditions where the cuff was deflated. In addition, our model did not incorporate vocal cords, which precluded us from considering the permeability of a patient's upper airways in our analysis. We also did not compare the different existing tracheostomy tube models or the possibility of incorporating fenestrated tubes to facilitate phonation. Given that our results indicated minimal clinical differences between the most challenging scenario (cannula capping) and the other conditions tested, we would expect that the subtle variations inherent to different tracheostomy tube models would likely have little impact on patient outcomes. Last, the minimal variability in the WOB across different tracheostomy modalities could be attributed to the inspiratory effort being specifically calibrated for each lung model. If the respiratory effort settings on our models were more adaptive, a greater variability in WOB might have been anticipated depending on the conditions. Although the controlled conditions of our experimental model enhance the reliability of our findings, the lack of variability could limit how directly they can be applied to real-world clinical settings. Notably, some statistical differences we observed, particularly in the WOB, are likely to have limited clinical significance. Hence, these results should be cautiously interpreted and may need adaptation for actual clinical environments, considering factors beyond our experimental scope.
Our results support the use of conditions that involve cuff deflation. We also noted that intermediate modalities, such as using an artificial nose or a speaking valve with the cuff deflated, yielded results that were very close to, if not indistinguishable from, those observed with cannula capping. Considering the risk of airway dryness, the reduction in the number of days before decannulation, and in the absence of contraindications (glottic control disorders and upper airway obstruction), the choice between capping and speaking valve may look trivial and should be more discussed among the healthcare staff.
In conclusion, our innovative model allows us to provide arguments for cuff deflation. The differences between intermediate conditions and capping are minimal and encourage clinicians to reduce the number of steps before attempting capping. The results of this bench study need to be validated with clinical data.




留言 (0)