
記住我



This prospective observational study included 51 patients scheduled for on-pump cardiac surgery with an indication for perioperative TEE. They were included between October 2022 and March 2023 at St Olav’s University Hospital, Trondheim, Norway, and excluded if they were < 18 years old, unwilling to participate, or had clinical contraindications to TEE [19]; poor image quality or arrhythmias were not exclusion criteria. Due to study resources, we included a maximum of one patient daily. Our study did not interfere with standard clinical care. This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Regional Committee for Ethics in Medicine (REK number 2022/345556). All patients provided written informed consent prior to participating. We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist [20] when composing this manuscript.
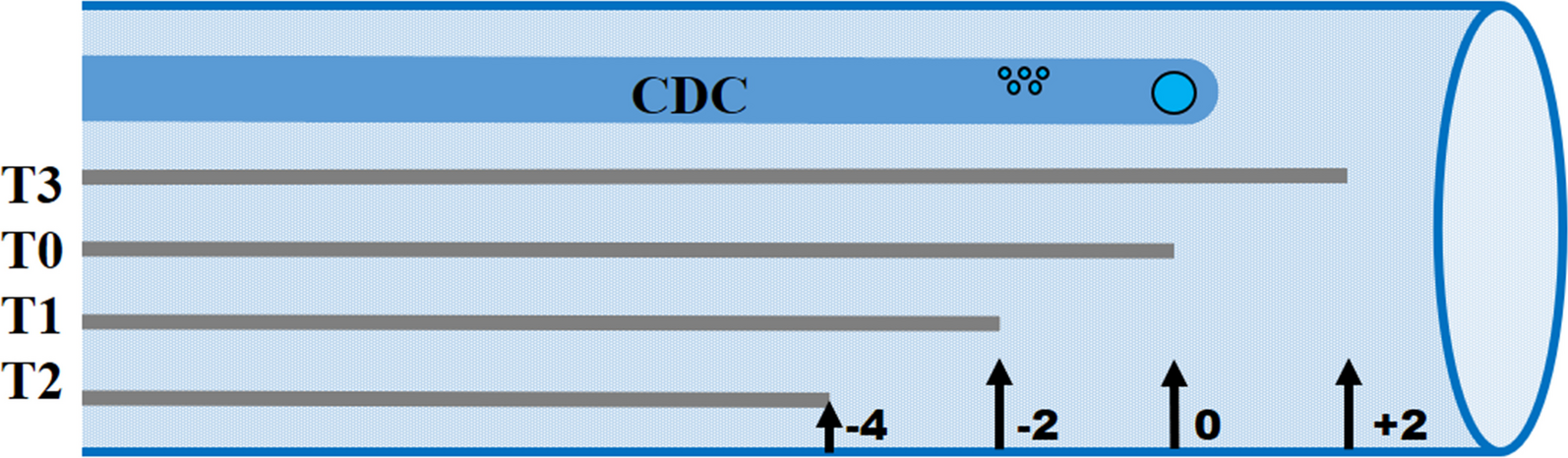
Study designTo assess the various requirements for monitoring, we recorded several sets of hands-on and hands-free images in the operating room (Fig. 1A) as well as in the intensive care unit (ICU) immediately after surgery (Fig. 1B and C).
Fig. 1
Study design. A One set of hands-on images was recorded before cardiopulmonary bypass (CPB) and two sets of hands-free images were recorded when initiating CPB. B One set of hands-free images was recorded every five minutes, and one set of hands-on images was recorded every 20 min. C Triplicate images were taken in rapid succession when the patients were hemodynamically stable in the intensive care unit (ICU). Filled circles, hands-free images; open squares, hands-on images. CPB cardiopulmonary bypass, ICU intensive care unit, MAPSE mitral annular plane systolic excursion
Image acquisitionHands-on images were obtained by retroflecting and turning the probe with the omniplane at 90 degrees to acquire a mid-esophageal two-chamber (2C) view without foreshortening. Then, we used simultaneous biplane imaging (Multi-D®, GE, Healthcare, Horten, Norway) and aligned the secondary sector through the LV apex. Next, we rotated the omniplane angle in the secondary sector to approximately 0 to 30 degrees to acquire an optimized mid-esophageal four-chamber (4C) view. The reason for using biplane imaging from 2C, rather than 4C, was because visualization of the LV apex is often not possible in the 4C using TEE. Finally, we maximized the sector width and increased the temporal resolution to at least 40 frames per second.
The hands-free images were acquired by leaving the tip of the probe passive in the esophagus after acquiring the hands-on images. We used single-plane imaging to compensate for the reduced image quality. The temporal resolution was not adjusted. To allow prolonged hands-free imaging, we secured the probe with a custom-made probe holder (Supplementary Video 1). For consistency, the hands-free images were obtained with a maximized sector width and predefined omniplane rotations (90 degrees for 2C and 30 degrees for 4C) unless stated otherwise. The image was adjusted to include the mitral annulus from at least one wall. To minimize the risk of esophageal trauma, we ensured that the probe tip was always unlocked during prolonged hands-free imaging [21, 22].
Each set of images consisted of 2C and 4C views, providing MAPSE from up to four LV walls. To increase precision, we recorded up to ten heartbeats and measured MAPSE on all available beats. Thus, we reported one measurement of MAPSE as the average MAPSE of up to ten heartbeats for each wall at a specific time point. All images were recorded using a state-of-the-art scanner (E95, GE, Healthcare, Horten, Norway) with a 6VT-D probe (GE, Healthcare, Horten, Norway). A trained researcher with three years of clinical anesthesiology training (J.Y.) recorded all the images.
ICU protocolTo assess hands-free autoMAPSE for continuous monitoring, we monitored each patient for 120 min starting immediately after they arrived at the ICU (Fig. 1B). The TEE-probe remained in situ after surgery. Every five minutes, we recorded a set of hands-free images; each set comprised ten consecutive heartbeats of 2C and 4C views (Fig. 1B).
We also recorded a set of hands-on images every 20 min (Fig. 1B); each set comprised, again, ten consecutive heartbeats of simultaneous biplane images of 2C and 4C views. At each 20-min interval, we recorded the hands-free images before the hands-on images. Later, we compared the automatic measurements from the hands-on images with the preceding hands-free images to assess the effect of small probe adjustments. Outside each scheduled 20-min interval, we adjusted the probe only if the LV was completely displaced from the image. We noted these displacements, recorded a set of hands-free images, and adjusted the probe.
Definitions of monitoring feasibilityTo continuously monitor LV function, MAPSE of the same wall for the same patient must be reassessed over time. To quantify reassessment over time, we first defined hands-free autoMAPSE as feasible if it measured MAPSE from at least one wall at a specific time point (Fig. 1B). We based this criterion on reports showing that MAPSE from any wall reflects global LV function, not the regional LV function of that wall [23,24,25,26]. Then, we defined monitoring feasibility as how often we could reassess the same wall from the same patient during the ICU protocol. If it was ≥ 90% of the total recordings, we categorized monitoring feasibility as excellent. If it was 50–90%, we categorized it as acceptable, and if it was < 50%, we categorized it as poor.
Triplicate imagesTo assess the precision of each method, i.e. hands-on and hands-free image recordings, we recorded a triplicate set of images in the ICU during a period of stable LV function (Fig. 1C). Within a time frame of less than one minute, we assumed stable LV function if the patient had otherwise stable mean arterial pressure, heart rate, and drug infusions. Within this short time frame, we rapidly recorded a triplicate set of hands-on and hands-free images.
Trending abilityTo assess the ability of autoMAPSE to detect changes in manual measurements (trending ability), we recorded images at two different time points where we expected changes in MAPSE. Trending ability for hands-on and hands-free images was assessed differently. For the hands-on images, the first time point was recorded during the clinical echocardiography examination before cardiopulmonary bypass (CPB, Fig. 1A), and the second time point was during the recording of the triplicate images in the ICU (Fig. 1C).
For the trending ability of hands-free images, we used a prolonged recording (approximately 30 s) during the initiation of CPB (Fig. 1A). When initiating CPB, venous return is drained into the extracorporeal circuit, reducing LV preload and MAPSE within seconds. The acquisition of the hands-free images was slightly different during the initiation of CPB; in order to obtain MAPSE from all four walls, we used simultaneous biplane imaging with maximized sector size and temporal resolution of at least 40 frames per second. Like the other hands-free images, the probe’s position was stabilized externally, and the probe tip was kept passive. The first time-point was the average MAPSE of the first three-to-five heartbeats of this prolonged recording, while the second was the average MAPSE of three-to-five heartbeats after full CPB.
Echocardiographic measurementsWe analyzed the images using both autoMAPSE and manual measurements, resulting in four different echocardiographic measurement methods: (1) hands-free autoMAPSE, (2) hands-on autoMAPSE, (3) hands-free manual MAPSE, and (4) hands-on manual MAPSE.
Manual measurements of MAPSEWe manually measured the MAPSE of every wall using calipers directly on B-mode images in EchoPAC software (version 204, GE Healthcare, Horten, Norway). Again, we averaged the MAPSE from ten heartbeats for increased precision. Details regarding the technique for manual measurements of MAPSE using TEE (Fig. 2) have previously been presented by our group [10]. The interobserver variability of this manual method has been previously reported (intraclass correlation of 0.86, bias − 0.9 mm, limits of agreement [LOA] − 4.7 to 3.0 mm) [10]. We rated the image quality of the hands-free images as suboptimal if we could not clearly see the annulus in more than two of the four walls. The images from the ICU protocol were not manually measured (Fig. 1B).
Fig. 2
End-systolic image of mid-esophageal two- and four-chamber views to demonstrate the manual measurements of mitral annular plane systolic excursion (MAPSE) on B-mode images. For each of the four walls, the mitral annulus is identified in end-diastole (open circles) at its the highest position, and in end-systole (solid circles) at its lowest position. MAPSE is the distance between end-diastole and end-systole (yellow brackets). MAPSE, mitral annular plane systolic excursion
Automatic measurement of MAPSE using artificial intelligenceWe used autoMAPSE on all the recorded images, obtaining the MAPSE of each of the four LV walls automatically. AutoMAPSE is a custom-made software we have developed, validated [10, 11], and refined [12] at our institution. The autoMAPSE pipeline comprises a convolutional neuronal network that was trained under supervised learning to detect the mitral annulus in TEE images [12], as well as a set of filtering algorithms for rejecting erroneous measurements (Fig. 3) [10]. The refined version of autoMAPSE used in this present study incorporates spatial and temporal information, which improves the consistency of predicting the frame-to-frame position of the mitral annulus [12]. After detecting the mitral annulus throughout each heartbeat, autoMAPSE measures the distance traveled by the mitral annulus from the highest to the lowest position within each wall and heartbeat [10]. The filtering algorithms rejected the autoMAPSE measurement if (1) the mitral annulus was detected more than 5 mm apart between two frames, (2) the mitral annulus was detected in less than 60% of the frames per heartbeat, and (3) the highest position of the mitral annulus was not detected around the R-wave of the electrocardiogram [10]. The final output is the MAPSE of the two LV walls for each recording, reported in millimeters after averaging all feasible heartbeats for each wall. Further technical details are found elsewhere [10, 12].
Fig. 3
Overview of the pipeline of autoMAPSE. 1 For each frame, the mitral annulus is automatically detected using artificial intelligence, indicated by the red and blue dots. 2 For each cardiac cycle (vertical lines), MAPSE is the distance between the highest and the lowest point. The brackets demonstrate the MAPSE of one cardiac cycle. The longitudinal motion of the mitral annulus is measured for all cardiac cycles for the entire recording. 3 Erroneous measurements (none in the example image) are rejected automatically by the filtering algorithms described in the main text. 4 The final output is the average MAPSE of all cardiac cycles within each wall. AI artificial intelligence, MAPSE mitral annular plane systolic excursion
Statistical analysisTo compare autoMAPSE with manual measurements, we used the outcomes bias, limits of agreement (LOA), the precision of each method, and trending ability. Bias, LOA, and precision were assessed using the triplicate images (Fig. 1C). Because each patient had triplicate measurements from four LV walls, the measurements had a within-patient dependency. Unless adjusted for, this within-patient dependency will cause the LOA to be underestimated [27, 28]. We made this adjustment using the linked replicates model described by Carstensen [28]. This approach modifies the Bland–Altman analysis using a linear mixed model with restricted maximum likelihood, where the fixed effects were measurement method and patient, and the random effects were measurement method-patient interaction and patient-MAPSE interaction [28]. Because the imprecision of manual measurements independently widens the LOA, the utility of autoMAPSE could be falsely rejected [29, 30]. When validating AI in echocardiography, a common solution to this issue is to target the interobserver variability [15,16,17]. Thus, we defined acceptable agreement a priori based on the previously established interobserver variability using the same manual measurement method for MAPSE as ours (LOA − 4.7 to 3.0 mm) [10].
To calculate the precision of each method, we used the residual standard deviation (SD) of each measurement method from the linked replicates model and reported the precision as the least significant change (LSC) using the formula [28, 31]:
$$LSC= \sqrt\times 1.96 \times \frac}$$
In this formula, each measurement was the average MAPSE of ten heartbeats from one LV wall, not the MAPSE of one heartbeat.
We assessed the trending ability using a four-quadrant plot and reported the concordance rate with and without a central exclusion zone of 10% change (0.7 mm) [32]. Using an exclusion zone increases the signal-to-noise ratio, and we adapted the zone of 10% change from validation methods for cardiac output monitors [32]. We defined trending ability as excellent if concordance rates were ≥ 95%, and good if concordance rates were ≥ 80%. Finally, we assessed the significance of each method's change in MAPSE by fitting a linear mixed model for each method. In each model, MAPSE was the dependent variable, time point was the fixed factor, and walls and patients were random factors.
We reported central tendencies as mean (SD) if data were Normally distributed, otherwise as median [interquartile range]. The normality of distributions was assessed by visual inspection of histograms. The threshold for statistical significance was set at P-value < 0.05. Missing data were not replaced. The statistical analysis plan was established a priori. The sample size was decided based on our experience with similar method comparison studies. We used Stata 17.0 (StataCorp LLC) for all statistical analyses.
留言 (0)