In this study, hypovolemia, PEEP and autotransfusion were important determinants of recirculation. The alterations were comparable to other well-known factors, such as ECMO circuit flow and intravascular cannula distance. There were large variations in both recirculation and hemodynamics, supporting previous studies that report difficulties in measuring recirculation correctly (1). All findings support the notions that 1) recirculation is a multifactorial phenomenon and might increase with and without changes in drainage pressure, as well as with or without hemodynamic changes and 2) that recirculation is ultimately determined by how circulatory and respiratory physiology, as well as ECMO circuit configuration, affect blood supply to the ECMO drainage cannula [18].
Hypovolemia and autotransfusion
A likely explanation for recirculation during hypovolemia is that a lower circulating blood volume leads to IVC collapsibility, a partial occlusion of the drainage cannula side holes and drainage through the cannula tip only. The result is a functionally shorter distance between the return cannula and the drainage cannula, ultimately leading to increased recirculation. It follows from the Poiseuille equation on flow resistance that with cannula sideholes open, blood mainly drains through the proximal side holes, not the cannula tip. Thus, the draining point within the IVC may vary several centimeters solely due to IVC collapsibility [19]. In addition, hypovolemia and reduced IVC inflow probably cause more blood to be directed through the ECMO drainage cannula without passing through the patient's circulatory system and thus increases RF even with all cannula sideholes open [18, 20]. Our study suggests that recirculation increases during hypovolemia and, importantly, may do so without increasingly negative drainage pressure or cannula chattering.
PEEP
A likely explanation for the large variations in recirculation during high PEEP is related to heart–lung interactions, as cyclic variations in intrathoracic and intra-abdominal pressure lead to alterations in venous supply to the IVC drainage cannula throughout the respiratory cycle [1]. These cyclic variations highlight that accurate estimation of recirculation requires a representative blood sample obtained throughout the whole respiratory cycle. This source of error may partially explain the lack of consistency in recirculation measurements in general. Specifically, high PEEP leads to increased CVP followed by an increase in IVC diameter and improved drainage from all cannula holes. Occasionally, the variations were visually apparent as alternating blood color in the drainage cannula [21]. Our study suggests that recirculation increases during high PEEP and, in contrast to recirculation during hypovolemia, may do so with less negative drainage pressure.
ECMO circuit flow
Recirculation increased during high ECMO circuit flow. Increasing ECMO pump speed leads to increasingly negative drainage pressure, IVC wall collapsibility, occlusion of the drainage cannula sideholes, drainage through the cannula tip only and likely to a functionally shorter intravascular cannula distance as described above. In addition, increased outflow from the return cannula is directed towards the drainage cannula. PaO2 was unaltered, indicating that oxygen delivery remained adequate despite increased recirculation [12].
Cannula distance
Intravascular cannula position, distance and configuration are important determinants of recirculation, but there are no clear recommendations on the ideal position or separation between the drainage cannula and the return cannula [1, 10, 18, 20, 22]. Several cannulation strategies have been proposed, including reverse ECMO flow direction (atrio-femoral or femoro-femoral), x-configurations [23], dual lumen cannula, cannulas with expanding net baskets that prevent vessel walls from collapsing around the cannula [19], right ventricular cannula [24] and pulmonary artery return cannula. All have their benefits and disadvantages, but none have so far proven superior efficiency [25].
In clinical practice, maximizing the distance between the two cannulas is widely used to reduce the possibility of recirculation [1]. However, withdrawing the drainage cannula into a smaller blood vessel may lead to cannula sidehole occlusion and a functionally shorter distance between the cannulas as described above, paradoxically not reducing recirculation.
In addition, a drainage cannula in the lower IVC mainly draws blood from the lower body, allowing poorly oxygenated blood from the SVC to enter the heart without circulating through the ECMO circuit. In the upper IVC position, blood from the SVC, IVC, and hepatic vein is probably more uniformly drained. Thus, the supply of venous blood at the drainage site appears to be more important than cannula tip proximity per se, and altogether these mechanisms may limit how far the drainage cannula may be withdrawn [18, 22]. Our data suggest that retracting the cannula too far may not reduce recirculation as effectively as expected.
Limitations
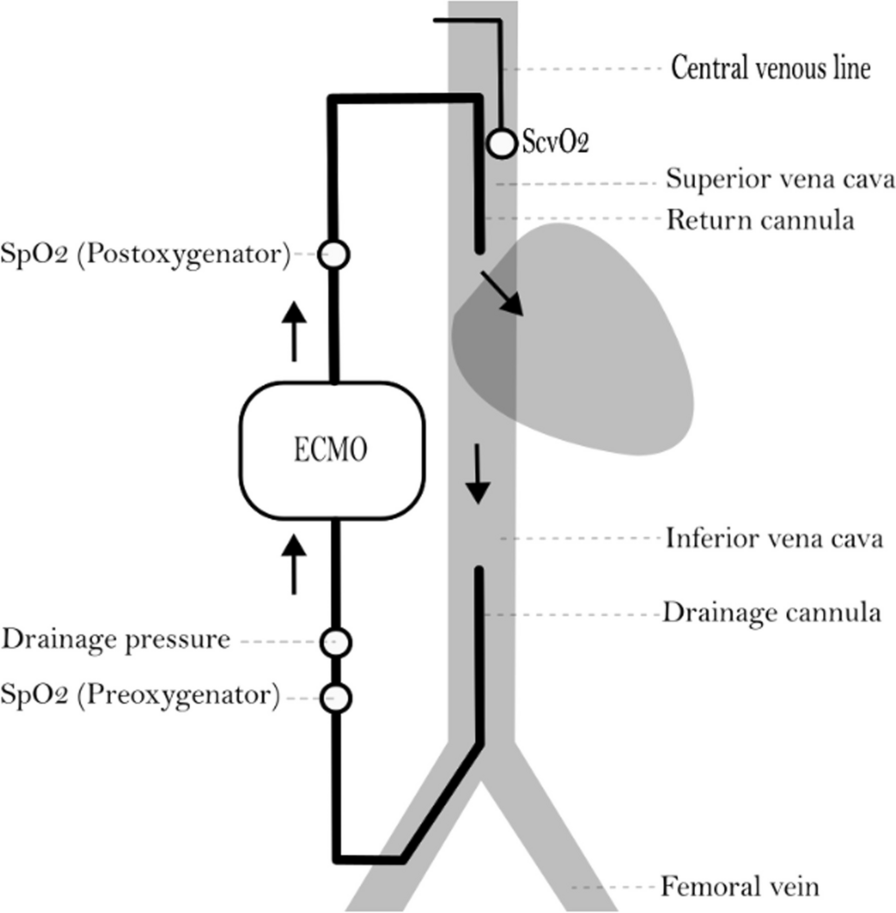
The most important limitation in this study is the CVL method to estimate recirculation. The CVL method is clinically applicable, but not always accurate as true ScvO2 is difficult to obtain in patients on VV ECMO [26]. First, because oxygen saturation in the SVC and the IVC vary substantially. Second, because the blood sample from the CVL may be partially mixed with oxygenated blood from the ECMO return cannula. Hence, ScvO2 obtained from the CVL may be falsely elevated, leading the RF equation to be negative if ScvO2 is higher than the SpreoxyO2. However, the trends we report are consistent and indicate methodological robustness regardless of absolute values and measuring method.
There are several other ways to measure the RF. A practical approach is to compare SpreoxyO2 and SpO2. Increasing SpreoxyO2 and concomitantly decreasing SpO2 are early indicators of recirculation [1]. Other methods include using systemic arterial blood gas analysis to indicate or exclude significant recirculation [27, 28]. These methods, however, do not provide quantification of the RF. Quantitative RF measuring methods are based on ScvO2, thermodilution, lithium dilution, ultrasound dilution, oxygen content and/or sweep gas adjustments [1, 10, 11, 29].
Other limitations include the small number of animals and possible interactions between the interventions. Future studies should confirm our findings with other measuring methods and investigate different cannula types, sizes and configurations.




留言 (0)