
記住我




The study was performed on eighteen 8–10-week-old Norwegian Landrace piglets, weight 27 ± 4 kg. The experiments were performed at Hedenstierna Laboratory, Uppsala University, Sweden.
The experiment was approved by Uppsala University’s Animal Ethics Committee (C 155/14 and 5.8.18-08592/2019). All animals were handled according to the guidelines of the Swedish Board of Agriculture and the European Convention on Animal Care. The study was reported in adherence to the Animal Research: Reporting of In Vivo Experiments (ARRIVE 2.0) guidelines [18, 19].
Anaesthesia and preparationAnaesthesia was induced by an intramuscular injection of a mixture of tiletamine–zolazepam 6 mg/kg and xylazine 2.2 mg/kg. Thereafter, anaesthesia was intravenously maintained by a continuous infusion of sodium pentobarbital 8 mg/kg/h and morphine 0.26 mg/kg/h dissolved in 2.5% glucose. Rocuronium bromide 1–3 mg/kg/h was infused continuously. This dose is to prevent shivering and not to give a total muscular block. The piglets were able to trigger in the ventilator or make small movements. If signs of insufficient anaesthesia were observed by movement, increasing heart rate or blood pressure, anaesthesia was immediately deepened by a bolus injection of ketamine and with a subsequent increase of infusion rate. Ringer’s acetate solution was administered at 1 ml/kg/h, resulting in a total fluid administration rate of approximately 10 ml/kg/h.
A tracheotomy was performed. The animals were mechanically ventilated throughout the experiment (Servo-I, Maquet, Stockholm, Sweden) with initial settings of respiratory rate 25/min, inspired oxygen fraction 0.3 and peak end expiratory pressure (PEEP) was set to 5 cmH2O. Tidal volume was approximately 8–10 ml/kg which at baseline yielded an arterial partial pressure of carbon dioxide (paCO2) of 4.5–5.5 kPa. Respiratory rate was adjusted to keep paCO2 at baseline level.
A central venous catheter (CVC) and a 13.5 Fr dialysis catheter (CDC) (Hemo-Cath SDL136E, MedCOMP, Harleysville, PA, USA) were inserted through the right external jugular vein (EJV) into the SCV. The tip is tapered with venous holes approximately 2 cm from the arterial holes.
A cervical artery was catheterized for pressure monitoring and blood sampling. A 7 Fr Swan-Ganz catheter was inserted in the pulmonary artery from the left EJV for monitoring. A urinary catheter was introduced via a bladder incision.
DialysisThe CRRT machine (MultiFiltrate, Fresenius Medical, Stockholm, Sweden) was prepared with a priming kit (multiFiltrate Ci-Ca® CVVHD 1000) with integrated polysulfone filter membrane (Ultraflux® AV 1000S) with a 1.8m2 surface area.
CRRT was started with continuous venovenous haemodialysis (CVVHD) settings and kept throughout the experiment: blood flow 60 ml/min (approximately 2.2 ml/kg/h), dialysate flow 1200 ml/h, citrate target 4 mmol/L, post-filter ionized calcium level 0.25–0.34 mmol/L, ultrafiltration 0 ml/min.
ProtocolThe pigs were anaesthetized as stated above. At the beginning of the preparation, an infusion of vancomycin, 4.55 mg/ml, was started in a peripheral vein at 9 mg/kg for 30 min and thereafter reduced to 3 mg/kg/h throughout the rest of the experiment. The vancomycin infusion rate after 30 min was 17 ± 2.6 ml/h. Gentamicin, 10 mg/ml, was infused with 3 mg/kg for 30 min and thereafter reduced to 1.5 mg/kg/h. The gentamicin infusion rate after 30 min was 3.8 ± 0.6 ml/h. The dose regimens were calculated to reach steady state. When the infusion rate was lowered, the infusions were moved to the CVC.
CRRT was started, followed by a 30-min stabilization period to ensure that the venous access and dialysis circuits were functioning adequately.
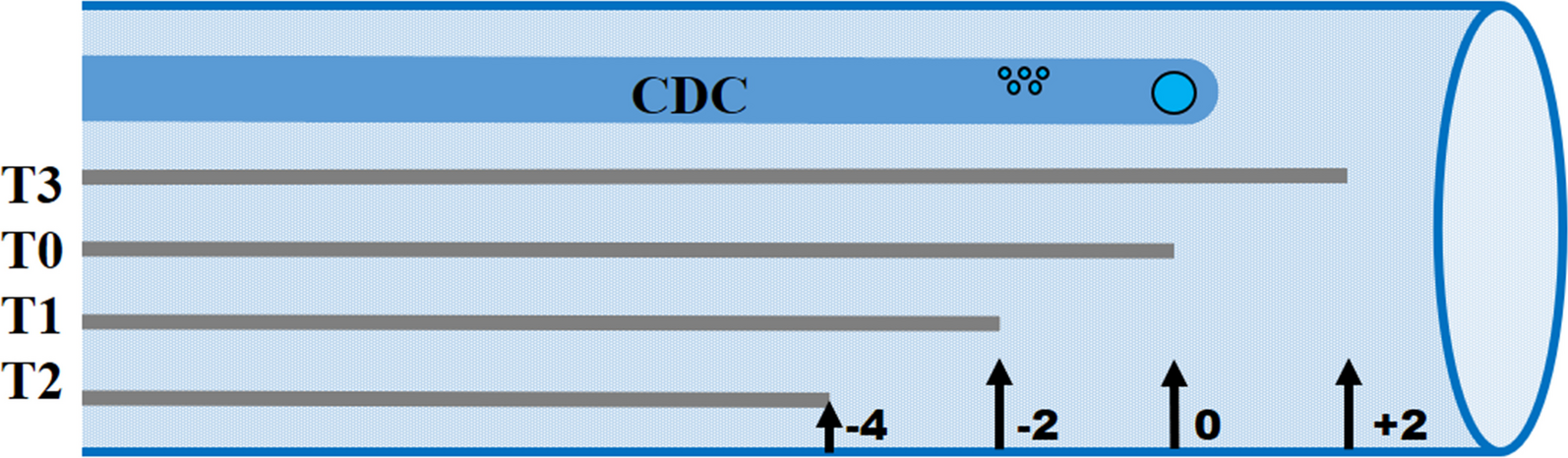
The tips of the CVC and CDC were placed in close proximity to each other with the tip of the CDC 2 cm cranially from the atrio-caval junction. The position was confirmed using fluoroscopy. After 1 h and 20 min of antibiotics infusion (T0), concentration samples of gentamicin and vancomycin were taken from dialysate and blood via the arterial line. After blood sampling, the tip of the CVC was withdrawn 2 cm cranially and the new position was again confirmed using fluoroscopy. After approximately 30 min (T1), concentration samples of gentamicin and vancomycin were taken from blood and dialysate. The procedure was repeated with the CVC tip 4 cm cranially from the start position (T2) and, lastly, 2 cm caudally from the start position (T3) (Fig. 1).
Fig. 1
Central dialysis catheter (CDC) and central venous catheter (CVC) tip positions. The CDC has the outflow port, i.e., venous, at the tip of the catheter and inflow holes, i.e., arterial, at approximately 2 cm cranially from the tip. Each grey line represents the same catheter placed in four different positions. The CVC tip was placed in different positions in relation to the CDC tip from caudal, i.e., proximal to the heart, to cranial, i.e., distal to the heart at each position, marked with black arrows, antibiotic concentration samples were taken in blood and dialysate and dialysate clearance was calculated. Sampling started at 0 cm (T0) and the CVC was withdrawn cranially to − 2 cm (T1) and − 4 cm (T2). Thereafter, the CVC was placed caudally to the CDC at + 2 cm (T3)
If needed, noradrenaline (20 µg/ml) was given in the CVC with a target MAP of 60. At the end of the experiment, anaesthetic depth was controlled using surgical forceps. If there were signs of insufficient anaesthesia, the anaesthesia was increased. Thereafter, the piglets were euthanized by intravenous potassium chloride.
Laboratory analysesPlasma and dialysate were obtained for analysis of gentamicin and vancomycin concentrations at the start position, at − 2, − 4 and + 2 cm from start position (0 cm). Samples of blood gases were obtained at the start of CRRT as well as at the beginning and end of the experiment. Blood samples for antibiotic concentration, blood gases and point of care analyses were taken from the arterial line. Blood gas and point care analyses were performed on an ABL 800 blood gas analyser (Radiometer, Brønshøj, Denmark). Gentamicin and vancomycin were analysed on an Architect ci16200 (Abbott Laboratories, Abbott Park, IL, USA) with reagents (1P31) from the same manufacturer.
Clearance was calculated as follows:
$$}\, = \,(}\;} \times }\;})/}\;}.$$
Statistical analysis methodsData were analysed using Jamovi 1.6.15.0 (IBM Corporation, Armonk, NY, USA) and Statistica 14.1 (Cloud Software Group Inc, Palo Alto, CA, USA). Testing for normal distribution was performed using the Shapiro–Wilk test or histogram. Normally distributed data are presented as mean ± standard deviation (SD); data with a non-normal distribution are presented as median and interquartile range (IQR). Differences in timepoint characteristics were tested for using an independent Student’s t test or Mann–Whitney U test according to normality. A mixed linear model was used to test for differences between catheter positions with catheter distance and intercept as fixed effects and piglets as random effect. The level of significance was set at p < 0.05.
留言 (0)