2.1 Data Source
We obtained clinical data from the electronic health records database of the Hospital Authority (HA), vaccination records from the Department of Health (DH), and COVID-19 confirmed case records from the Center of Health Protection (CHP) of the Government of the Hong Kong Special Administrative Region (HKSAR). The HA is the statutory administrative organisation managing the public healthcare sector, providing all public inpatient services and the majority of outpatient services in Hong Kong. The electronic health records database of the HA contains data on patient demographics, diagnoses, procedures, prescriptions, laboratory tests, inpatient admissions, and outpatient and emergency department attendances, providing real-time information to support routine clinical management across all public clinics and hospitals. The DH maintains a database of COVID-19 vaccination records for all Hong Kong citizens. The CHP maintains a database of all confirmed COVID-19 cases, based on both mandatory and voluntary reporting of positive polymerase chain reaction (PCR) and rapid antigen test (RAT) results. These territory-wide databases were integrated using unique anonymised patient identifiers, and have been frequently applied in prior studies about the risk of adverse effects following COVID-19 vaccinations and the effectiveness of COVID-19 oral antivirals [13, 14].
The Hong Kong government has implemented extensive PCR testing for SARS-CoV-2 in public hospitals and clinics for close contacts with confirmed cases. Territory-wide community testing centres were also in place to screen asymptomatic individuals and provide regular testing to various staff groups with a high risk of exposure, such as those working in nursing homes. Compulsory SARS-CoV-2 testing were conducted among three groups: close contacts of confirmed cases, high-risk individuals, and residents in areas suspected of having local outbreaks or positive sewage test results. Individuals were required to fulfill this mandate by reporting either PCR or RAT test results [15]. Reporting of positive RAT results via an online system set up by the HKSAR government was necessary to obtain official proof of SARS-CoV-2 infection, which was required for purposes such as the fulfilment of a compulsory testing notice, exemption of booster vaccination requirements, and application of sick leave [16]. The DH also conduct random checking on voluntarily reported RAT results, and it is an offence to declare false information. Thus, it is expected that the possibility of false-positives is minimal while the proportion of missed asymptomatic infections remains relatively small compared to other regions relying solely on voluntary testing.
2.2 Study Design and Eligibility Criteria
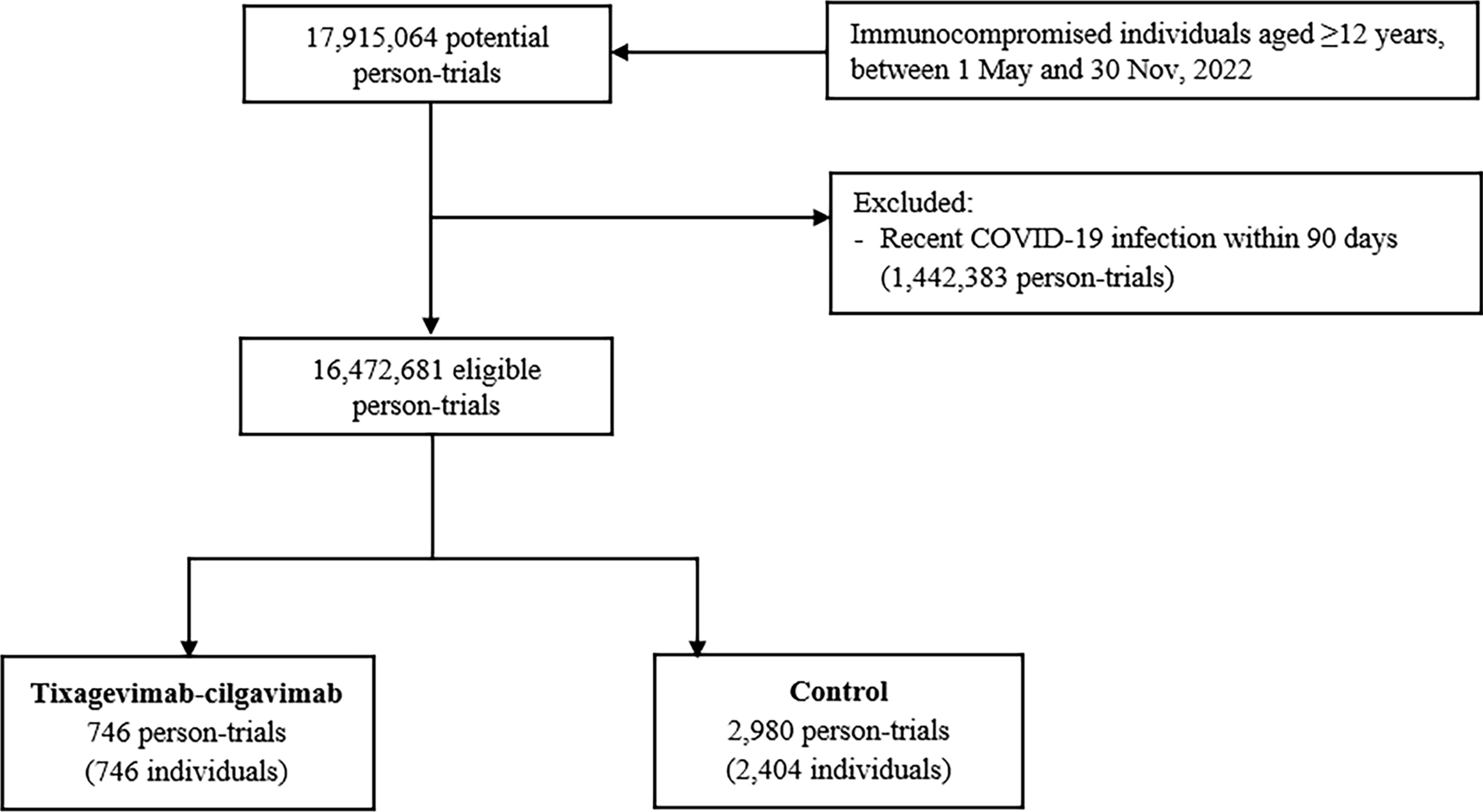
A target trial emulation study was conducted using territory-wide electronic health records databases in Hong Kong. The target trial emulation approach is appropriate to prevent some of the common pitfalls encountered in observational study designs, such as immortal time and selection biases [17]. The setting of this target trial was largely adapted from the PROVENT trial [6], with important differences in the eligibility criteria to reflect real-world clinical practice, which is discussed further below. The specification and emulation of the target trial are presented in Supplementary Table 1 (see the electronic supplementary material). The participant inclusion period was from 1 May 2022 (when tixagevimab–cilgavimab became available in Hong Kong) to 30 November 2022 (to allow at least 60 days of follow-up). Individuals aged ≥ 12 years who had an immunocompromised condition or had received immunosuppressive treatment within 1 year were included (see Supplementary Table 2 for detailed definitions). These eligibility criteria were selected in accordance with real-world clinical practice, since currently the use of tixagevimab–cilgavimab is limited to the immunocompromised population in Hong Kong, despite being approved by the FDA for any individuals aged ≥ 12 years prone to inadequate response to COVID-19 vaccines [7]. The dosage of tixagevimab–cilgavimab was 300 + 300 mg. Patients who had previously received COVID-19 vaccination or had a history of COVID-19 infection (> 90 days before baseline [18]) remained eligible, and their vaccination and infection status were accounted for in the analyses. Patients who had a recent COVID-19 infection within the past 90 days were excluded, to prevent counting re-positivity of a previous SARS-CoV-2 infection as an outcome [19]. Patients who died on or before baseline were also excluded.
2.3 Exposure and Control Matching
A sequential trial emulation approach was adopted to compare the risk of outcomes between individuals who received tixagevimab–cilgavimab and individuals who did not receive tixagevimab–cilgavimab [20, 21]. On each day during the participant inclusion period (index date), all eligible individuals who newly received tixagevimab–cilgavimab (recipients) were matched 1:4 to eligible individuals who had not yet received tixagevimab–cilgavimab on that day (controls), using exact matching (and nearest-neighbour matching with a narrow calliper of 0.2 when exact matching was not feasible). Covariates matched included age, sex, number of COVID-19 vaccine doses received (exact match), months since last COVID-19 vaccine dose, history of COVID-19 infection (exact match), months since previous COVID-19 infection, Charlson Comorbidity Index (CCI) score, type of immunocompromised condition, immunosuppressive therapies received within 1 year, and presence of other comorbidities (chronic kidney disease, respiratory disease, diabetes, cardiovascular disease, dementia). These covariates were selected since they were potential confounders of tixagevimab–cilgavimab treatment and COVID-19 infection and severity. These covariates were time-varying and updated at daily intervals.
The index date for tixagevimab–cilgavimab recipients was defined as the date of first prescription of tixagevimab–cilgavimab, whereas the index date for controls was assigned as per their matched tixagevimab–cilgavimab recipients. Individuals were followed up from the index date until the earliest outcome occurrence, death, 60 days after the index date, or the end of data availability (31 January 2023). Controls who received tixagevimab–cilgavimab after the index date were censored on the date of first tixagevimab–cilgavimab prescription (the corresponding individuals matched with these controls were also censored), and would be re-enrolled as a tixagevimab–cilgavimab recipient with a new set of matched controls.
2.4 Outcomes
The primary outcome was COVID-19 infection, defined as a positive PCR or RAT result. Secondary outcomes included (1) COVID-19-related hospitalisation, defined as hospital admission within 28 days after COVID-19 infection; (2) severe COVID-19, defined as intensive care unit (ICU) admission or use of ventilatory support within 28 days after COVID-19 infection; and (3) COVID-19-related mortality, defined as all-cause mortality within 28 days after COVID-19 infection. Information regarding mortality was extracted from the Hong Kong Deaths Registry, the official government registry documenting all registered deaths in Hong Kong. Use of ventilatory support was identified using International Classification of Diseases-Ninth Revision (ICD-9) procedure codes (39.65, 89.18, 93.90, 93.95, 93.96, 96.7, 96.04).
Safety outcomes for descriptive analyses included a pre-specified list of adverse events of special interest (AESIs) covering various organ systems, identified using ICD-9 codes (Supplementary Table 3; see the electronic supplementary material). These AESIs were adapted from those endorsed by the World Health Organization (WHO) and the European Medicines Agency for the safety surveillance of COVID-19 vaccines, and have been used in previous studies to evaluate the safety of COVID-19 vaccines in Hong Kong [22], and they are also applicable to the safety assessment of pharmaceuticals, particularly biological medicines. The validity of ICD-9 codes in our database has been demonstrated in previous population-based studies, with a high positive predictive value (PPV) for many diagnoses [23, 24].
2.5 Statistical Analysis
Covariate balance in the matched cohort was assessed, and an acceptable threshold for the standardised mean difference (SMD) between tixagevimab–cilgavimab recipients and controls was set at 0.2 or less for all covariates. Survival curves were presented using the Kaplan–Meier estimator, and p values of the log-rank test were reported. Cox proportional hazards regression was used to compare the risk of outcomes between tixagevimab–cilgavimab recipients and controls. Hazard ratios (HRs) with 95% confidence intervals (CIs) were reported. Schoenfeld residuals test was conducted to test the assumption of proportional hazards. For safety outcomes where the number of events was limited, incidence rates were reported with 95% CIs estimated based on Poisson distribution. As the follow-up duration was relatively short, post-baseline time-varying covariates and competing risk of death were not considered in this study.
Pre-specified subgroup analyses stratified by vaccination status (0–2 or ≥ 3 vaccine doses received), age (12–59, ≥ 60 years), sex (male, female), and CCI score (0–4, ≥ 5) were carried out. Interaction effects between treatment and vaccination status, age (continuous variable), sex, and CCI score (continuous variable) were also tested, and the p values for interaction were reported. Sensitivity analyses was conducted where the definition of patients with cancer was restricted to only patients with active cancer (defined as patients with cancer undergoing chemotherapy or radiotherapy or those who had metastasis within 1 year before the index date), rather than all patients with a cancer diagnosis before index.
All statistical tests were two-sided, and p values less than 0.05 were considered statistically significant. Statistical analysis was conducted using R version 4.0.3 (http://www.R-project.org). Two investigators (VY, YY) conducted the statistical analyses independently for quality assurance. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklists were followed to guide transparent reporting of the cohort study.




留言 (0)