
記住我
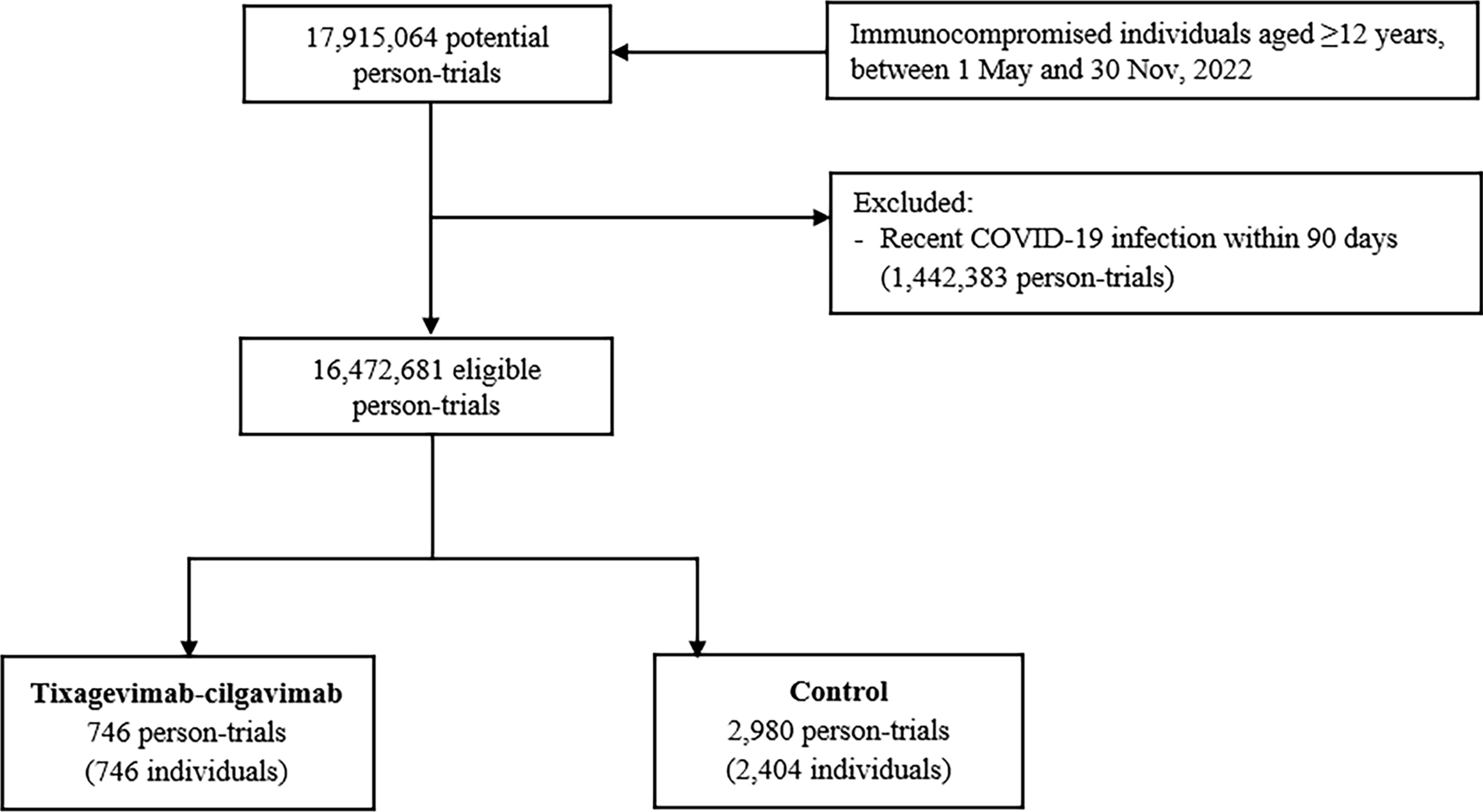


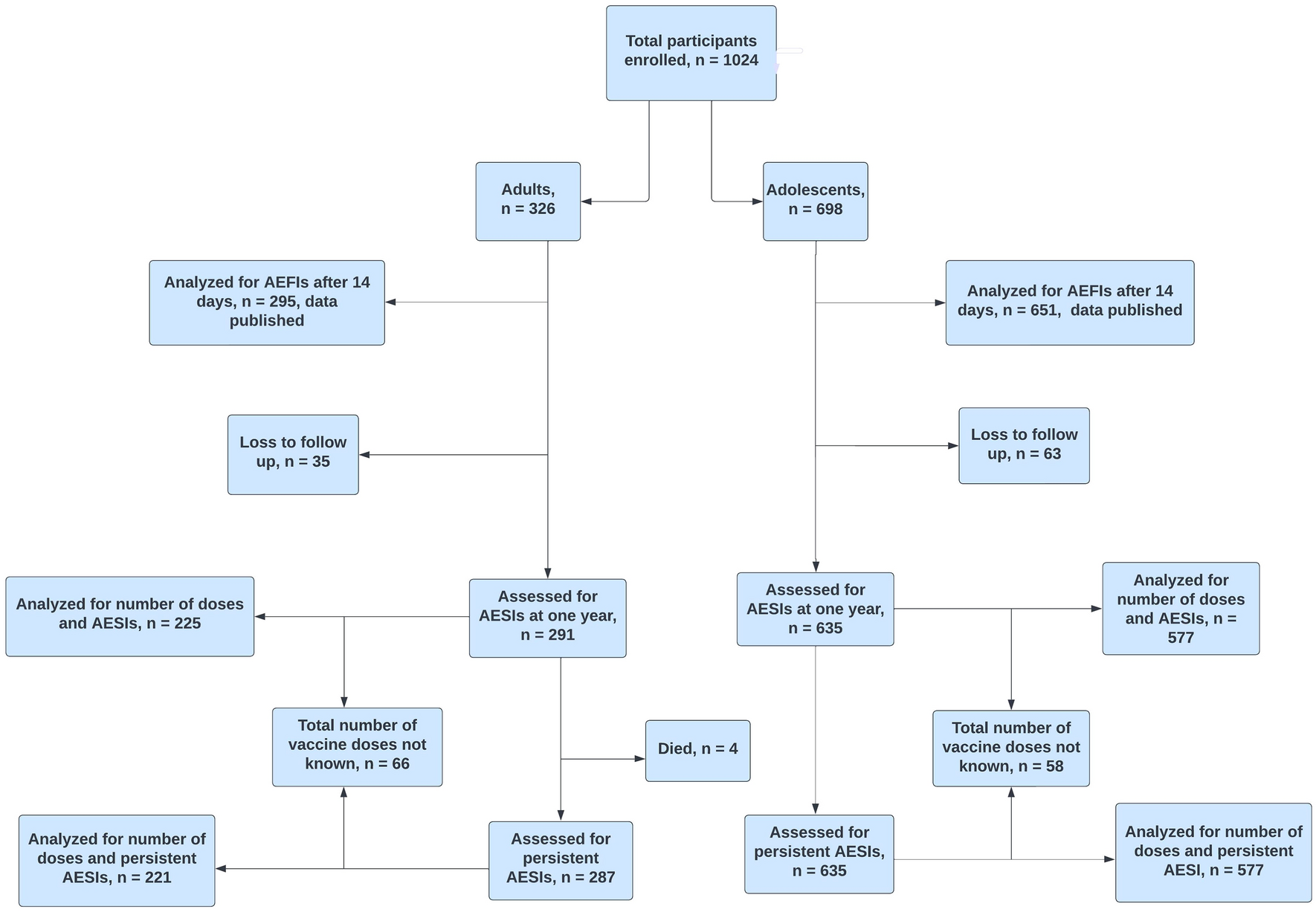

Overall, a total of 946 recruited immunocompromised vaccinees completed the baseline questionnaire at either first vaccination cycle (653, 69.0%) or booster dose (293, 31.0%). Of these, only 773 (81.7%) (N = 566, 73.2% at the first dose, N = 207, 26.8% at the booster dose) filled also at least the first FU-Q and therefore were finally included in the analysis. Those vaccinees were matched 1:4 to 3092 non-immunocompromised vaccinees by age, gender, dose, and vaccine brand (N = 2264, 73.2% at the first dose; N = 828, 26.8% at the booster dose) from the same source population.
Considering vaccinees recruited at the first vaccination cycle, 59.0% of the immunocompromised subjects and 61.9% of the matched controls completed all six questionnaires; instead, at the booster dose, only 41.5% of the immunocompromised vaccinees versus 48.3% of the matched controls completed all the five questionnaires (Fig. 1).
Fig. 1
Flowchart including the number of questionnaires filled by immunocompromised vaccinees and matched control, at the first vaccination cycle and the booster dose
3.1 Demographic and Clinical CharacteristicsAs shown in Table 1, at the first vaccination cycle, the majority of vaccinees were female (68.0%), and the median age was 56 (IQR: 43–74) years. Regarding vaccine brand, 29.2% of vaccinees included in the study received the Vaxzevria vaccine, 49.1% Comirnaty vaccine, 17.7% Spikevax vaccine and 3.7% Jcovden vaccine.
Table 1 Demographic and clinical characteristics of immunocompromised people versus matched controls, following the administration of the first dose and the booster dose of any vaccineAs for the booster dose, 61.8% of recruited vaccinees were female, and the median age was 51 (IQR: 41–60) years. Almost all the vaccinees received Comirnaty (62.8%) or the Spikevax vaccine (36.2%).
The main cause of immunosuppression reported was immunosuppression due to autoimmune disorder (N = 111, 53.6%). Other causes of immunosuppression reported were related to malignant tumour (13.5%), infection (5.3%), and rheumatic disease (2.9%). In addition, 12.2% of patients did not report this information.
Furthermore, almost half of the subjects enrolled (48.8%) indicated a current use of medications that affect the immune system, particularly the use of immunosuppressants (32.9%) like TNF-alpha inhibitors and selective immunosuppressants.
3.2 Descriptive Analyses of ADR FrequenciesThe frequency of immunocompromised people and matched controls reporting at least one ADR in FU-Qs was similar. After the first vaccination cycle and the booster dose, most subjects reported at least one ADR after the FU-Q1 (first vaccination cycle: immunocompromised subjects: 71.4%, matched controls: 65.5%; booster dose: immunocompromised subjects: 57.0%, matched controls: 57.6%) (Supplementary Table 3).
Overall, after all doses, higher frequencies of at least one ADR in the immunocompromised versus matched controls were reported (Table 2). The frequency of vaccinees reporting at least one ADR was higher after the first dose of any COVID-19 vaccine (immunocompromised vaccinees: 82.0%; matched control: 76.1%), as compared to the second (80.7% and 74.0%) and the booster (61.8% and 59.7%) doses.
Table 2 Frequency of immunocompromised people and matched controls reporting at least one ADR, at least one solicited/unsolicited/serious ADR and at least one AESI, following the administration of the first dose and the booster dose of any vaccineOverall, when compared to the matched controls, the immunocompromised cohort showed a higher frequency of solicited ADRs after all doses. A statistically significant difference was especially observed for nausea after the first dose (p = 0.003), and for nausea (p = 0.005) and arthralgia (p = 0.005) after the booster dose (Supplementary Table 4).
Injection-site pain was the most frequently reported local solicited ADR following all doses for both groups (immunocompromised subjects vs matched controls: first dose: 41.2% vs 37.8%, second dose: 25.3% vs 24.7%, booster dose: 40.1% vs 35.7%). As for systemic solicited ADR, fatigue was reported most commonly after all doses, for both immunocompromised vaccinees (first dose: 38.2%, second dose: 25.3%, booster dose: 32.9%) and the matched control (first dose: 32.9%, second dose: 23.6%, booster dose: 29,8%) (Supplementary Table 4).
All solicited ADRs were more frequently reported in females, as compared to males, across all doses and study cohorts. Specifically, immunocompromised females showed higher frequencies of local solicited reaction injection-site pain following the first dose (48% vs 27%) as well as the booster dose (52% vs 20%) when compared to males. Additionally, increased frequencies of the systemic solicited reaction fatigue were observed in immunocompromised females vs males (first dose: 47% vs 20%, second dose: 30% vs 17%, booster dose: 38% vs 24%) (Fig. 2 and Supplementary Table 5).
Fig. 2
Heatmap for vaccinee-reported local and systemic solicited ADRs following the first, the second and the booster dose of any vaccine, in immunocompromised people and matched controls, stratified by gender
Systemic solicited ADRs were most frequently experienced by participants after the first dose of the Vaxzevria vaccine and the Jcovden vaccine and after the second dose of the Spikevax vaccine. In detail, after the Vaxzevria vaccine, headache was the most reported systemic solicited ADR in both groups (immunocompromised subjects: 57% vs matched control: 60%). Fatigue (67%) was the most frequently reported reaction after the administration of the Jcovden vaccine in immunocompromised vaccinees, while malaise (52%) in the matched control. Regarding the second dose, for immunocompromised vaccinees and matched controls, fatigue (53% vs 46%) and malaise (51% vs 58%), respectively, were the most frequently reported ADRs after receiving the Spikevax vaccine. At the booster dose, the highest frequency was observed for fatigue (37% and 31%) after the Spikevax vaccine for both study groups (Fig. 3 and Supplementary Tables 6, 7, 8).
Fig. 3
Heatmap for reported local and systemic solicited ADRs following the first, the second and the booster dose of any vaccine, in immunocompromised people and matched controls, stratified by vaccine brand
The frequency of vaccinees reporting at least one unsolicited ADR was highest after the first dose of COVID-19 in both groups (immunocompromised subjects vs matched controls: first dose: 34.8% vs 30.7%, second dose: 23.1% vs 20.3%, booster dose: 17.4% vs 14.0%). Dizziness was the most frequently reported unsolicited ADR after the first dose of COVID-19 vaccines in both groups (immunocompromised subjects: 2.5% and matched controls: 2.1%) and after the second dose in matched controls (1.0%), while immunocompromised people indicated extensive swelling of the vaccinated limb (1.4%) after the second dose. At the booster dose, lymphadenopathy (3.9%) and lymphadenitis (1.8%) were the most reported unsolicited ADRs for immunocompromised subjects and matched controls, respectively.
Of note, after the first dose, 3 (0.5%) immunocompromised subjects indicated “condition aggravated” and 1 (0.2%) “Crohn’s disease”. At the booster dose, 2 (1.0%) immunocompromised subjects reported “rheumatoid arthritis”, 1 (0.5%) “ankylosing spondylitis”, 1 (0.5%) “polymyalgia rheumatica”, and 1 (0.5%) “psoriasis” (Supplementary Table 9).
For each study cohort, only 1 AESI was reported after the administration of the first dose of any COVID-19 manufacturers. In particular, in the FU-Q1, 1 (0.2%) immunocompromised vaccinee reported “epilepsy”, while 1 (< 0.1%) matched control “facial paralysis”, both with Vaxzevria vaccine.
After the second dose, in the FU-Q3, 1 (0.2%) immunocompromised subject indicated “platelet count decreased” after the administration of Spikevax, while 1 (0.1%) “hypersensitivity” (FU-Q3, Comirnaty) and 1 (0.1%) “facial paralysis” (FU-Q3, Spikevax) were reported for matched controls. No AESIs were reported after the booster dose in either group (Supplementary Table 10).
With regard to serious ADRs, at the first dose, only 3 (0.5%) immunocompromised subjects and 3 (0.1%) matched controls reported at least one serious ADR. At the second dose, only 2 (0.5%) immunocompromised subjects reported serious ADRs, while at the booster dose, serious ADRs were reported by only 2 (0.2%) matched controls. Supplementary Table 10 provides a comprehensive list of reported serious ADRs.
3.3 Analyses of Time-to-Onset and Duration of EventsOverall, after both the first vaccination cycle and the booster dose, participants showed a median TTO within one day. In particular, the median TTO of reported ADRs in the first vaccination cycle was equal to 20.9 h and 17.9 h for immunocompromised vaccinees and matched control, respectively (p = 0.424). For the booster dose, the median TTO for the immunocompromised vaccinees and matched controls was slightly shorter (13.7 h vs 15.4 h, p < 0.001) (Fig. 4).
Fig. 4
Combination of violin plot and boxplot of the median time to onset (in h) and time to recovery (in hours) of reported ADRs for the first vaccination cycle and the booster dose, in immunocompromised people and matched control
A statistically significant difference was observed in the median TTR in immunocompromised vaccinees versus matched controls (first vaccination cycle: 40.9 h vs 37.7 h, p < 0.001; booster dose: 40.8 h vs 38.4 h, p < 0.001) (Fig. 4).
留言 (0)