
記住我
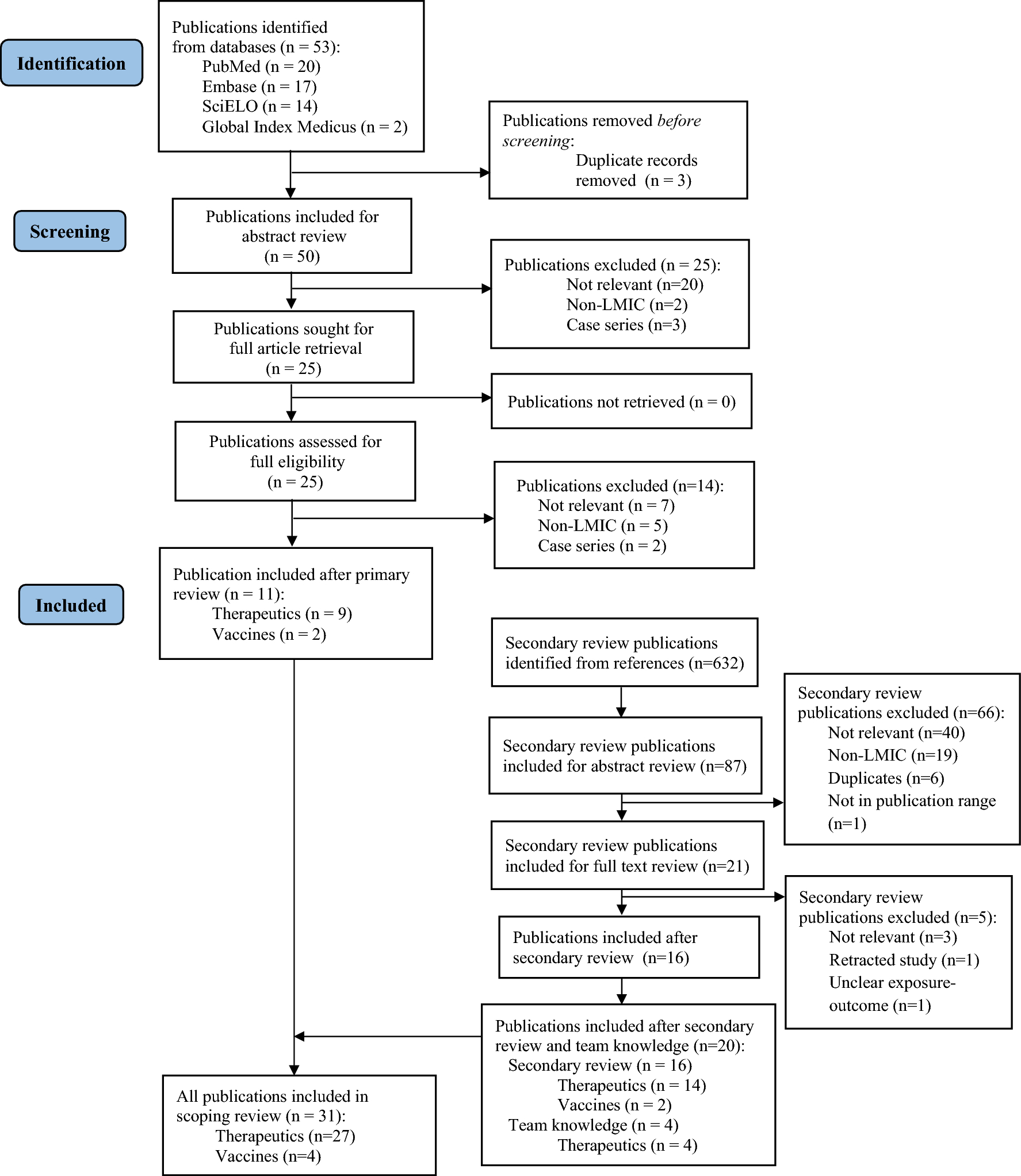


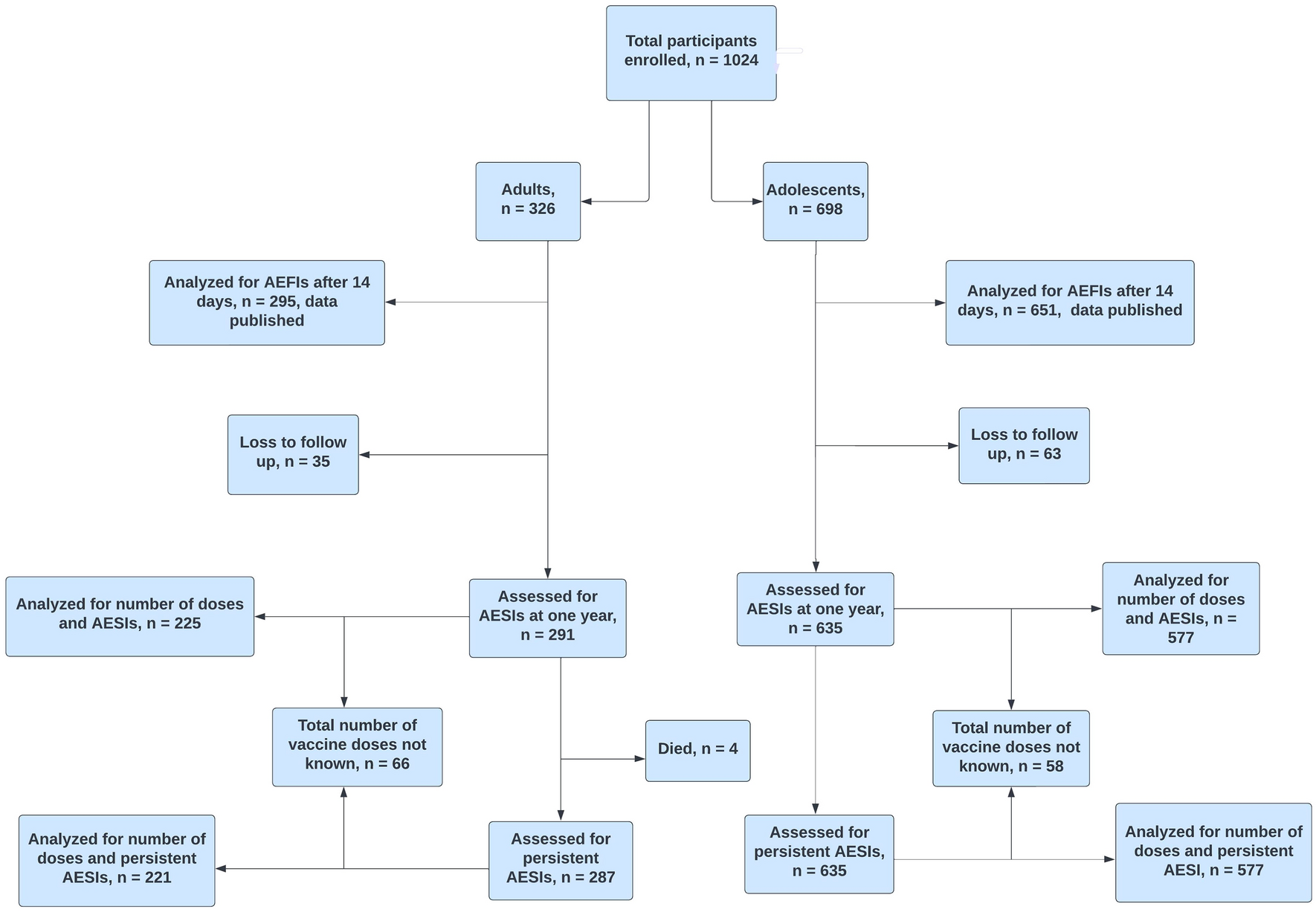

In our primary review, our search string produced 53 publications across all databases. After deduplication, there were 50 publications remaining (Fig. 1, [13]). We identified 25 publications meeting our inclusion criteria based on title and abstract alone. We included these 25 publications for full text review. Of these, 14 were excluded for the following reasons: irrelevant (i.e., did not report maternal, birth, or neonatal/infant outcomes, n = 7), publication focus was non-LMICs (n = 5), or publication was a case series or case report (n = 2). The database sources for the 11 included publications were: PubMed (n = 8), Embase (n = 2), SciELO (n = 1), and none were identified from Global Index Medicus.
Fig. 1
Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) publication selection procedure flow chart. LMIC low- and middle-income country
From the secondary review of the references of the primary publications, we identified 632 references, of which 87 publications met our inclusion criteria based on title alone (Fig. 1 [13]). After abstract review, we excluded 66 publications and included 21 publications for full text review. These publications were excluded for being duplicates (n = 6), non-LMICs (n = 19), irrelevant (i.e., did not report maternal, birth, or neonatal/infant outcomes, n = 40), or for not being within the publication range (2012–2022, n = 1). After a full text review, we excluded 5 additional publications for the following reasons: retracted study ( n = 1), irrelevant (i.e., did not report maternal, birth, or neonatal/infant outcomes, n = 3), unclear exposure-outcome ascertainment (i.e., publication was a hypothetical trial, n = 1), leaving 16 secondary review publications.
After a full text review of all publications included in the primary and secondary review, we included 31 publications in our synthesis, with n = 11 included from the primary search string, n = 16 from secondary review, and n = 4 from team knowledge (Table 1).
Table 1 Publications included in scoping review (N = 31)4.2 Characteristics of Sources of EvidenceAfter compiling the data extraction for the 31 included publications, we further categorized the publications into two groups: publications relating to therapeutics for infectious diseases (n = 27, Table 2) and vaccines (n = 4, Table 3). The publications ranged across more than 28 countries, with several publications covering more than one country (n = 11); the majority of studies were from Africa (n = 28). Most publications ( n = 30) had pregnant people as the only study population. All of the publications covered infectious diseases/conditions, with most publications (n = 27) focusing on a therapeutic exposure (n = 17 for HIV, n = 7 for malaria, n = 9 for TB, n = 2 for multi-class therapeutics exposure) compared to publications about vaccinations (n = 1 for pertussis, tetanus, and diphtheria, n = 3 for influenza). As for outcomes, n = 15, n = 31, and n = 20 of the publications covered maternal, birth, and neonatal/infant outcomes, respectively.
Table 2 Summary of infectious disease-related publicationsTable 3 Summary of vaccine-related publications4.3 Synthesis of ResultsThe results are presented in two sections pertaining to infectious diseases-related (1) therapeutics and (2) vaccines. We discuss in detail common themes arising from the publications, including ascertainment of exposures and outcomes, timing of exposures during pregnancy, and comparator groups used in the exposure-outcome relationship assessment.
4.4 Infectious Diseases Therapeutics-Related Publications (Table 2)For the 27 infectious diseases therapeutics-related publications, the major diseases analyzed in relation to pregnant people and their newborns were HIV (n = 17), malaria (n = 7), drug-resistant tuberculosis (DR-TB)/multidrug-resistant tuberculosis (MDR-TB) (n = 9), along with multi-class therapeutics exposure (n = 2; Table 2).
4.5 HIVAmong publications with HIV as the infectious disease of study, the primary exposure-outcome relationship of focus was exposure to maternal antiretroviral therapy (ART) (primarily dolutegravir-, efavirenz-, nevirapine-containing ART or zidovudine monotherapy) and adverse maternal, birth, and neonatal/infant outcomes.
For the vast majority of HIV-centered publications (n = 17), a focal point of analysis was the time of ART initiation and the duration of treatment in relation to gestation, and birth, maternal, and neonatal/infant outcomes [14,15,16,17,18,19,20,21,22,23,24,25]. For example, some publications categorized the time of initiation into subcategories based on stages of pregnancy such as early (< 8 weeks), mid (9–20 weeks), and late pregnancy (21–36 weeks) [22] or first trimester (< 14 weeks), first half of second trimester (14–20 weeks), second half of second trimester (21–27 weeks), and third trimester (>28 weeks) [20]. Notably, Mehta et al specifically evaluated first trimester ART exposure and found that there was no association between first trimester exposure to efavirenz-containing ART regimens and congenital malformations yet found that first trimester exposure to nevirapine was associated with a greater risk of congenital malformations compared to births not exposed to ART during the first trimester [15]. The evaluation of first trimester exposure allowed Mehta et al to specifically comment on birth and infant outcomes in relation to specific exposure timing, as this cohort excluded pregnant people for whom the timing of ART was uncertain [15]. Similarly, by evaluating ART exposure based on varying lengths of treatment, Bengston et al was able to report that there was no evidence of elevated risk of low birth weight (LBW) infants for individuals receiving combination ART for any treatment length compared to individuals who never initiated ART [22].
However, most publications defined the categories of ART initiation as pre- (before) or post-conception (during pregnancy) (n = 8) [17,18,19,20,21, 23,24,25]. For publications defining ART initiation as pre- or post-conception, ART initiation preconception was defined as maternal ART that started before the calculated date of the last menstrual period (LMP), and post-conception ART initiation was defined as maternal ART that started after that date. To account for errors in estimation, one publication defined ART exposure prior to conception as 2 weeks before LMP, with broader exposure categories being based on the trimester in which ART treatment was initiated (e.g., 15 weeks post-LMP) [15].
Notably, many publications were able to comment on the significance of the timing of treatment initiation in relation to maternal, birth, and neonatal/infant outcomes due to exposure initiation stratification. To illustrate, Zash et al (2019) specifically sought to evaluate the effects of dolutegravir exposure at conception on the prevalence of neural tube defects and found that neural tube defects were more prevalent in association with dolutegravir-based treatment at conception than with non-dolutegravir ART at conception [18]. Ramokolo et al reported higher preterm delivery rates among pregnant people who initiated ART preconception compared to those who initiated ART post-conception [21]. Last, Chen et al evaluated ART exposure based on timing of ART initiation (before or after 32 weeks’ gestation), and thus were able to report that there were no significant differences in preterm delivery, SGA infants, or stillbirth rates based on timing of ART initiation [24].
To estimate gestational age in relation to the time of ART initiation, various factors were utilized across the publications. All publications utilized the estimated date of LMP and other factors depending on the data available in the publication. Some publications utilized LMP along with fundal height (n = 4) [20, 22,23,24], some used LMP and a dating ultrasound (if available) (n = 4) [15, 20, 24, 25], and one publication further assessed the accuracy of estimation by comparing the mean birthweight for each week of gestation age to a reference growth curve adjusted for the population [22]. For the majority of the reviewed HIV-related publications, whether they utilized data from a larger PV database or medical records, there was some degree of uncertainty in the exact timing of ART initiation relative to conception and/or trimester of exposure.
For HIV-centered publications that utilized comparator groups or had explicit information detailing their comparator groups, we found that all publications used contemporaneous/concurrent comparator groups (n = 10). Among these, the comparator groups included: pregnant people not living with HIV [15, 17,18,19,20], pregnant people living with HIV with various ART exposures [17,18,19, 21, 23, 24], pregnant people living with HIV with ART exposures at various gestational durations [22], and pregnant people living with HIV with no antenatal ART use [21]. Some publications collected data prior to WHO guidelines for universal ART use for pregnant people, thus overall ART exposure before and after this time period shifted [17,18,19, 23, 24].
4.6 MalariaFor publications with malaria as the infectious disease of study, the primary exposure-outcome relationship of interest was the association between antimalarial medication exposure during pregnancy and adverse maternal, birth, and neonatal/infant outcomes. These publications analyzed various antimalarial medications: artemisinin derivatives, such as artemisinin-based combination therapies (n = 6, [26,27,28,29,30,31]), quinoline derivatives, such as chloroquine, quinine, and amodiaquine (n = 3, [27, 28, 32]), and antifolates, such as sulfadoxine-pyrimethamine (n = 2, [28, 32]). The birth outcomes of interest were live birth, stillbirth, and miscarriages; birth maturity (preterm birth or full-term birth); birth weight; and congenital malformations. Among these publications there was an emphasis on examining the timing of exposure in relation to the outcome. Particularly, these publications sought to understand the effect of antimalarial medication exposure during the first trimester or preconception and adverse maternal, birth, and neonatal/infant outcomes [27, 29, 32], although two publications sought to understand the effect of antimalarial medication exposure during the second and/or third trimester compared to first trimester and preconception exposure (n = 2) [30, 31].
Many publications noted limitations in determining the timing of therapeutic exposure (due to incomplete records and related factors), particularly periconceptional exposure, which was dated retrospectively using estimated gestational age. Gestational age was most often estimated using LMP accompanied by other factors, depending on the publication [27, 29,30,31,32]. There were several combinations of estimation methods: 1) LMP, ultrasound, Dubowitz newborn assessment, fundal height formula validated for population [27], 2) LMP, Ballard score, fundal height, and ultrasound [31], or 3) LMP, fundal height, and date of quickening [30]. Last, one publication did not have such data available and used descriptive statistics to link records from outpatient and delivery/pregnancy complication registers [26].
For malaria-centered publications that utilized comparator groups or had explicit information detailing their comparator groups, we found that all publications used contemporaneous/concurrent comparator groups (n = 6). Among these 6 publications, the comparator groups included: pregnant people without malaria [27], pregnant people with an episode of malaria in first trimester [27], pregnant people with antimalarial therapeutic exposure during any period of pregnancy [28,29,30,31,32], and pregnant people (with or without malaria) with no therapeutic exposure [28,29,30,31,32].
4.7 TuberculosisFor publications where the infectious disease of focus was TB, there were two main exposure groupings: 1) second-line DR-TB or MDR-TB therapeutics and 2) isoniazid-based therapeutics. The publications that focused on second-line therapeutics exposure investigated linezolid [33], a fluoroquinolone [34, 35] and bedaquiline, clofazimine, and levofloxacin specifically [35] to treat DR-TB or MDR-TB. The publications focused on isoniazid-based therapeutics and analyzed the safety of isoniazid preventive therapy (IPT) among pregnant people living with HIV [36,37,38].
Among these publications, common outcomes of interest were adverse birth and neonatal/infant outcomes such as preterm birth, LBW, stillbirth/miscarriage, neonatal mortality, and congenital anomalies [28, 33,34,35,36, 38,39,40]. All publications analyzed some maternal TB/IPT treatment outcomes and adverse maternal outcomes, but they differed in the specific outcomes that were analyzed. Some publications defined adverse maternal outcomes as overall maternal morbidity and mortality [33], whereas other publications defined adverse maternal outcomes as therapeutics-related adverse events such as liver impairment, kidney function impairment, gastrointestinal disorders, or psychiatric disorder
留言 (0)