The concentration of antibiotics in the blood does not automatically indicate the concentration at the site of infection. Linezolid is often used in critically ill patients with pneumonia due to a postulated high penetration rate and is associated with a better outcome than the treatment with vancomycin [13, 18]. The measurement of linezolid in patients´ lung, if the suffer from pneumonia, seems, therefore, promising [14, 19]. The high rate of E. faecalis in our collective might be caused by the high number of immunosuppressed patients after severe infections with prolonged intensive care stay or organ transplantation. In other hospitals, the detection of, e.g., pneumococci, is to be expected.
Measuring linezolid concentrations in endotracheal aspirate is a potential new, simpler, and non-invasive method compared to BAL. It would be less time-consuming and does not require additional equipment, such as a bronchoscope. If the suctioning is performed with a closed system, the patient is not exposed to any loss of PEEP or risk of infection [15]. However, the suction depth, the thickness of the catheter and a potential biofilm formation in the endotracheal tubes could have an influence on the quality of the sample and the included linezolid concentration. In contrast, a standardized BAL also has different limitations: the dwell time plays a central role in the percentage of the drug that is transferred into the aspirate [20]. Furthermore, the high dilution with NaCl leads to very low drug concentrations with the necessity of reevaluating the calibration range. The transfer factor is typically estimated using the urea method, which, as already mentioned, is only an estimate [21, 22].
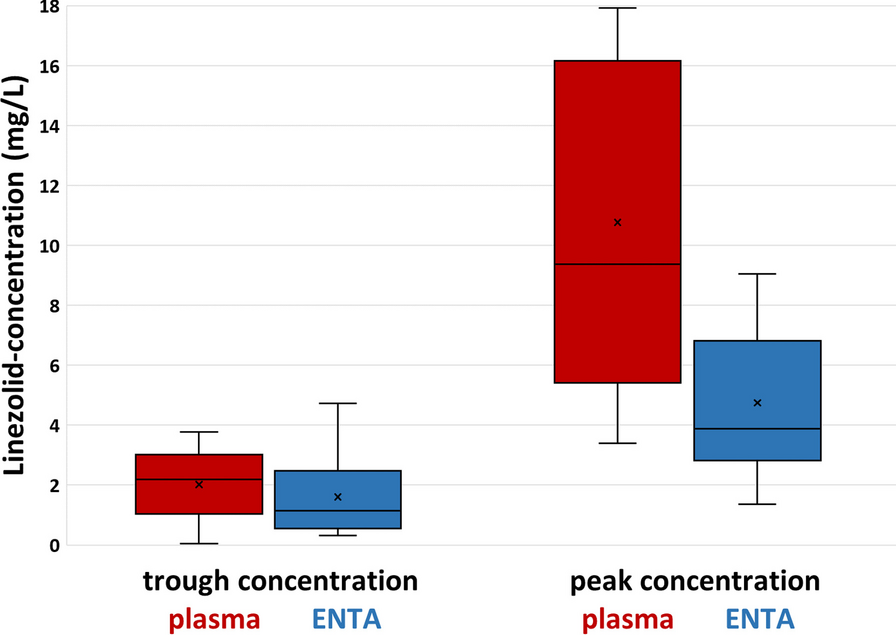
The preliminary measurements taught us that validly measurement of linezolid in the ENTA is possible in samples with sufficient volume (> 0.5 mL) and viscous texture. If there is too little liquid secretion, it is possible that only the condensation water from the ventilation tube is drawn off, and therefore, no valid measurement is possible. Patients with pneumonia mostly have viscous pulmonary secretions and the linezolid concentration in the lung is especially of interest in those patients. Linezolid trough concentrations in ENTA were shown to be comparable to plasma concentrations in appropriate patients, as confirmed by a moderate correlation coefficient of 0.52. In fact, 58% of the trough levels were even higher in ENTA than in plasma, which has already been observed in the BAL, demonstrating the good penetration of linezolid into the lung and indicating that our method might be valid for non-invasive measurement of linezolid in the critically ill [19, 23].
Although also peak concentrations were measured in plasma and ENTA and further concentrations in the dosing interval, no reliable interpretation can be made due to the lack of knowledge about the penetration velocity in patients with intermitted dosing. To improve the interpretation of the data, a pharmacokinetic model would be beneficial in the future. Significant differences were observed in the lung penetration rate of linezolid (e.g., patient 1 with a very low penetration rate). No specific cause can be named for this, although large inter-individual differences in the linezolid blood concentration are already known and the reasons for this are at least partially transferable to the lungs [9, 12]. This again demonstrates the need for TDM of linezolid not only in the blood but also at the site of infection to identify patients like patient 1 with low penetration rates and to enable the target range to be achieved in these patients as well [3, 21, 24].
Only four published studies were identified that investigated the intrapulmonary trough concentration of intravenously administered linezolid in critically ill patients using the gold standard “BAL”. This already shows that the current data situation is very limited. Boselli et al. studied the intrapulmonary concentration of linezolid in 16 patients with ventilator-associated pneumonia. The mean linezolid penetration into ELF was 104% [25]. In another study, Boselli et al. investigated the alveolar diffusion of linezolid during continuous linezolid administration in 12 patients with a median (IQR) linezolid penetration rate of 97% [19]. De Pascale et al. received a median penetration rate of 80% in seven critically ill obese patients [14]. Finally, Wu et al. studied 23 patients with sepsis and was able to show a penetration rate of 112% [10]. The median penetration rate into the ELF in these four studies is 101%. Based on the available data, all studies demonstrate a low variability of the penetration rate.
We observed a median ENTA/plasma ratio of the trough concentrations of 104%. The penetration rate measured in our study appears to be comparable to the median penetration rate measured in the ELF in the above-mentioned studies. It should be noted that a direct comparison is not possible as different patients were used. This allows the hypothesis to be derived that the measurement of linezolid in the ENTA might be a valid method for the future. To test this hypothesis, the measurement of linezolid in ENTA and BAL in the same patient at the same time is pending. The primary goal of examining whether linezolid can be measured in endotracheal aspiration in patients with viscous secretions was thus achieved.
This proof-of-concept trial has several limitations. Only nine patients were included and, therefore, less patients as in the published studies where linezolid was measured in the ELF. However, the goal of the proof of concept study was to verify if and when a measurement of linezolid in the ENTA is possible at all. This goal was achieved by including nine selected and valuable patients. Since the speed of linezolid penetration into the lungs is not yet known, it is unclear whether the linezolid peak levels in the blood corresponds to the peak level in the lungs when measured at the same time. A pharmacokinetic model could, therefore, be helpful. The penetration of linezolid into pneumonic areas may be limited, as they are less perfused under the assumption of the Euler–Liljestrand reflex. A BAL directly from this area might contribute to an even more precise determination of the concentration at the site of infection. Finally, linezolid in the lung was only determined in ENTA and not additionally from the BAL in the same patient. A direct comparison of the concentrations is not possible yet. The next step should be to directly compare the concentration in the ENTA with the concentration in the BAL in the same patient at the same time. Thereafter, ENTA can perhaps be used as a non-invasive standard method in the future.





留言 (0)