
記住我


Increasing the rates of opioid prescriptions and corresponding increases in morbidity and mortality have been seen in the United States, the United Kingdom, Canada, and Australia.6,11,13,14,29 A rise in the prescribing of opioids has been largely attributed to escalating use for chronic noncancer pain, despite limited compelling evidence supporting their use.10,28 In Australia, general practice encounters for chronic pain have risen by 67% over the past decade.5 A 2018 nationwide study using pharmacy dispensing data found that 2 million Australians initiate and 3 million use prescription opioids every year, with a majority prescribed in primary care settings.32
Tapering opioids (sometimes called “deprescribing”) has been identified as a key strategy in improving pain and reducing opioid-related harms in patients using opioids for pain outside the context of active malignancy or palliation.20,24,49 The 2010 Canadian Guideline for Safe and Effective use of Opioids for Chronic Noncancer Pain and the 2016 Centers for Disease Control and Prevention Guideline for Prescribing Opioids for Chronic Pain were updated in 2017 and 2022, respectively, both with greater communication around safe and effective deprescribing of opioids.7,15,17,21 In Australia, a National Health and Medical Research Council (NHMRC) endorsed Evidence-Based Clinical Practice Guideline for Deprescribing Opioid Analgesics was published in September 2022 to guide clinicians on when and how to taper opioids.35 Further efforts to advocate for opioid deprescribing were made by national and institutional bodies.22,41
Despite the focus on deprescribing opioids, guidance on specific aspects of how to taper patients off opioids are lacking nuance. Although many practice guidelines provided recommendations on the rate and frequency of dose reduction, there is minimal guidance around the use of different types of opioids or opioid formulations (eg, use of short or long-acting opioid formulations or combination of different opioids). In addition, guidelines recommend a multidisciplinary approach to maximise nonopioid pain therapies and provide physical and psychological support during opioid taper.1,16,17 However, there are limited real-world data on how different multimodal tapering strategies may influence the taper outcomes.
Careful tapering of opioids is important to avoid unintended consequences including exacerbation of pain and mental health crises including suicide attempts.2 A recently published systematic review and priority setting study further highlighted the need for high-quality evidence to guide the opioid tapering process.23,26 Therefore, the aim of this study was to determine characteristics of opioid and nonopioid interventions associated with successful opioid taper in patients with chronic noncancer pain.
2. Methods 2.1. Study design and settingWe conducted a retrospective cohort study among patients receiving opioid prescriptions between January 2015 and December 2020. We used data from the Population Level Analysis and Reporting (POLAR) database, an Australian primary care database containing routinely collected general practice data. The database includes approximately 700,000 deidentified patient records where opioid analgesics were prescribed and captures all opioid prescriptions irrespective of their subsidy status.38 The Opioid Prescribing, Policy Impacts, and Clinical Outcomes (OPPICO) study protocol details further information on the data set.9 This study was reported according to the RECORD-PE Checklist.34
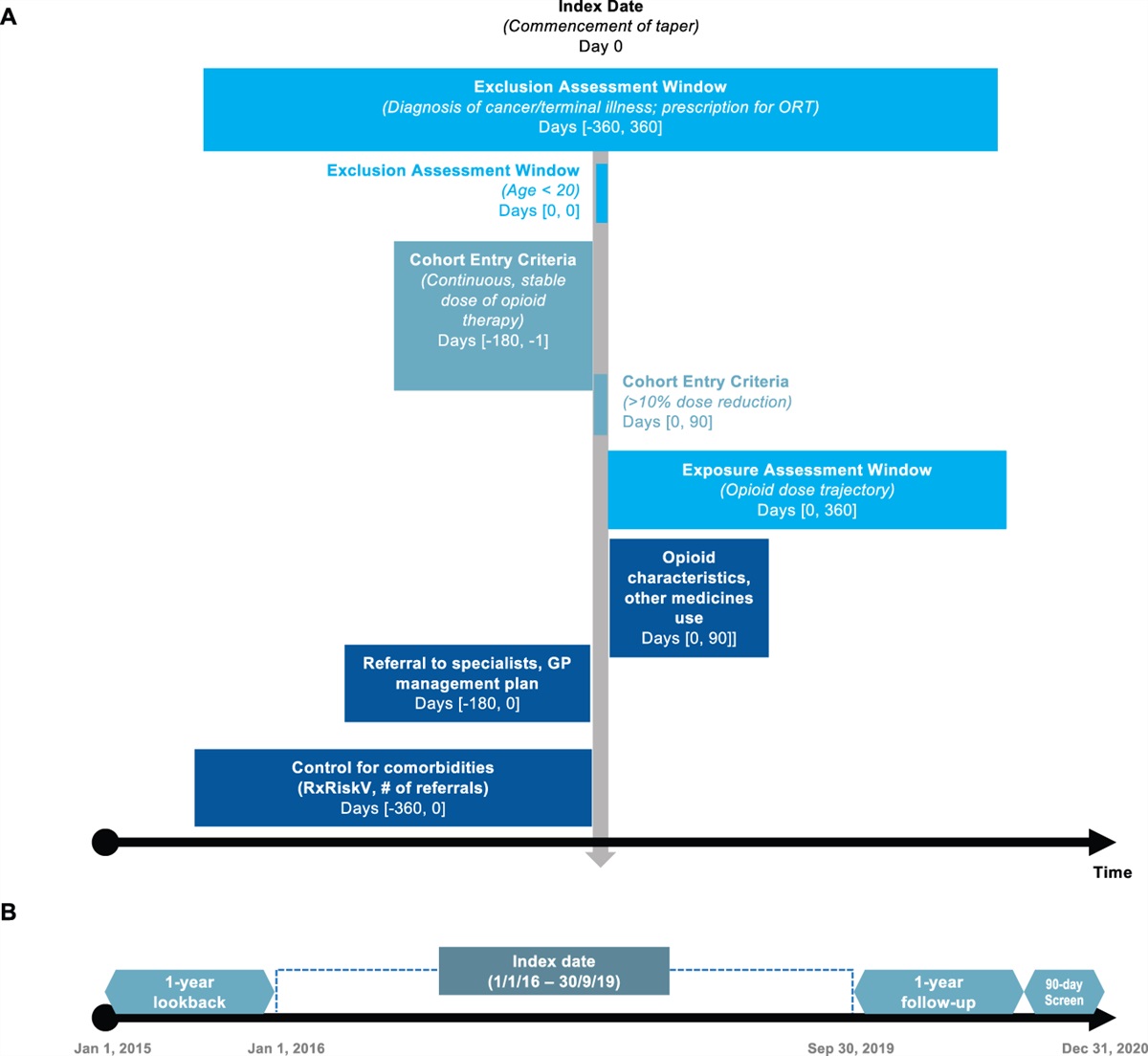
2.2. Cohort creationOur cohort comprised adults aged older than 14 years at cohort entry (equivalent to adults aged at least 20 years at the time of data extraction, with most [99.94%] being aged older than 18 years at cohort entry) prescribed long-term opioid therapy for the treatment of noncancer pain (Fig. 1A). Individuals taking opioid formulations solely used for cough or treatment for opioid use disorder were excluded. Long-term, stable dose was operationalised as having at least 6 months of opioid prescriptions with a gap of no more than 60 days between prescriptions, and average opioid dose in any single month that did not vary by more than 10% from the combined average opioid dose during the baseline 6-month period. We defined taper as greater than 10% reduction in opioid doses in the 90 days after the 6-month baseline period, compared with the average baseline dose (average monthly dose during the 6-month period immediately preceding the index date) (Fig. 2). Index date was defined as the point at which taper commences. Patients commencing taper were followed up for 12 months from the index date, using a 90-day rolling average dose to adjust for minor variations in supply dates. The same individual may have qualified multiple times for inclusion, but only the earliest taper episode was included. To exclude patients who disenrolled from the medical practices during the follow-up period, we required at least one clinic activity (eg, general practice [GP] visit or telehealth) or prescription to be recorded within 90 days after the date of the last opioid prescription. We also excluded patients with diagnosis of terminal illness or cancer (other than nonmelanoma skin cancer) and prescriptions for opioid replacement therapy (eg, methadone liquid and high-dose sublingual buprenorphine) in the 12 months before and 12 months after the index date. Further information on these variables can be found in the OPPICO protocol.9 To account for these screening windows, we censored the index date between 1 January, 2016, and 30 September, 2019 (Fig. 1B).
 Figure 1.:
Figure 1.: (A) Graphical depiction of the eligibility criteria and exposure and covariate assessment windows. (B) Illustration of the study time frame. The figure was adapted from Schneeweiss et al. (2019) (Schneeweiss S, Rassen JA, Brown JS, Rothman KJ, Happe L, Arlett P, Dal Pan G, Goettsch W, Murk W, Wang SV. Graphical Depiction of Longitudinal Study Designs in Health Care Databases. Ann Intern Med 2019;170:398–406). ORT, opioid replacement therapy.
 Figure 2.:
Figure 2.: Timeline illustrating assessment of opioid doses. Index date (day = 0), defined as time at commencement of opioid taper, was immediately preceded by a 6-month baseline period. Subsequent prescriptions during this period had a gap of no more than 60 days. Opioid doses in each of the baseline months did not vary by more than 10% from the average baseline dose, which was determined by calculating the daily average of the total dose prescribed during the 6-month baseline period (between days −180 to 0). To be considered a taper, a minimum 10% reduction in the average daily opioid dose must have been observed over a 90-day period (period 1) compared with the average baseline dose. Opioid doses were assessed for 12 months after the index date in 10 overlapping the 90-day period (periods 1-10). The figure was adapted from Fenton et al. (2019) (Fenton JJ, Agnoli AL, Xing G, Hang L, Altan AE, Tancredi DJ, Jerant A, Magnan E. Trends and Rapidity of Dose Tapering Among Patients Prescribed Long-term Opioid Therapy, 2008-2017. JAMA Netw Open 2019;2:e1916271).
2.3. Opioid prescriptionsWe included all opioids as listed in the OPPICO protocol9 (Table S1, available at https://links.lww.com/PAIN/B969). Opioid doses were converted to oral morphine equivalents (OME) using validated conversion factors.39 Where repeats were supplied on a given prescription, the total OME of the prescription was included every 28 days for transdermal and slow-release formulations and every 14 days for all other formulations. This definition was guided by our data and the standard duration of opioid supply in Australia. We imputed a small number of high doses of the average daily OME in the 90-day periods (n = 1155 of 60,678 [1.9%] of all observations; range: [250.22 mg, 1480 mg]) to a maximum value of 250 mg. This process was necessary as large variations in the dose (dependent variable) leads to technical errors in the group-based trajectory modelling analysis. To avoid having to exclude patients with these extreme values, we chose to cap the maximum dose and impute a dose of 250 mg in place of their actual high opioid doses. This approach enabled them to still be included as patients with high opioid doses in the analysis. The dose of 250 mg was determined to be the maximum dose that could be entered into the model without creating technical errors and is equivalent to approximately 3 standard deviations from the mean.3
2.4. CovariatesPredictors of opioid taper outcome included (1) opioid type and formulation (ie, the specific opioid such as morphine or oxycodone, in addition to whether the patient was prescribed only short-acting [SA] formulations or if they received a long-acting [LA] formulation alone or in combination with a SA formulation) prescribed in the 3 months after the commencement of taper (Fig. 1A, Table S1, available at https://links.lww.com/PAIN/B969); (2) concurrent prescriptions of other medicines including nonsteroidal anti-inflammatory drugs (NSAIDs), paracetamol, gabapentinoids, and benzodiazepines, as defined in the OPPICO protocol9; (3) GP management plan, identified through Medicare Benefits Schedule (Table S2, available at https://links.lww.com/PAIN/B969); and (4) referral to other healthcare professionals and services including medical and surgical specialists, allied health services, and mental health and addiction services (Table S3, available at https://links.lww.com/PAIN/B969). To minimise confounding, we controlled for the following measures at baseline: (1) age, (2) sex, (3) pension/concession status, (4) remoteness, (5) geographically derived socioeconomic status, (6) average daily OME during the 6-month baseline period, (7) number of referrals to other healthcare professionals (excluding those included as a predictor variable), and (8) number of comorbidities determined using Rx-Risk Index, a validated tool for determining comorbidities based on medication prescription.44 These measures have been chosen based on previous literature demonstrating their associations with tapering.19,27 Prescription of ≥2 opioid type was not included as a variable due to its correlation with opioid dose, resulting in multicollinearity. We chose to include opioid dose (a continuous variable) as it would provide more information than prescription of ≥2 opioid type (a dichotomous variable). Assessment time windows for each of the predictors and control measures are illustrated in Figure 1B.
2.5. Statistical analysisWe used taper groups defined in a prior group-based trajectory modelling analysis to identify the common trajectories of opioid taper.27 This model identified 6 trajectories including 3 completed and 3 noncompleted opioid taper trajectories (for details on group definition, see Supplement Methods, available at https://links.lww.com/PAIN/B969). These individual trajectory groups were collapsed to determine completed and noncompleted opioid taper groups (Figure S1, available at https://links.lww.com/PAIN/B969). Logistic regression was performed to examine the association between a set of predictors and completion of taper, compared with noncompleted taper (reference group). We tested for multicollinearity by determining the variance inflation factor (VIF). The highest VIF in our model was found to be 1.66, indicating a low correlation between the variables. To further ensure the validity of our model, variables with sample sizes less than 5 in either of the trajectory groups were excluded from the regression analysis. All analyses were conducted using Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC. Graphical illustrations were created using GraphPad Prism version 9.5.0, San Diego, California, and Microsoft PowerPoint version 16.70.
2.6. Data approval and ethical reviewThe study was approved by the Monash University Human Research Ethics Committee (Approval No. 24139).
3. Results 3.1. Sample characteristicsThe analysis included 3371 patients who commenced taper from at least 6 months of continuous, stable dose of opioid prescriptions. Of those, approximately a third (31.7%) completed taper (Table 1, Fig. 3). The highest proportion of the patients was in the 65 to 84 years age bracket for both the completed (37.2%) and the noncompleted taper group (40.6%). Most of our samples were women (62.5% and 61.1% in the completed taper and noncompleted taper cohorts, respectively). Of the total sample, the average number of comorbidities was 6.37 (SD: 2.56), and the average number of referrals to specialists in the 12 months before commencing a taper was 4.49 (SD: 7.37).
Table 1 - Descriptive characteristics of patients and their opioid and nonopioid interventions by taper outcome. Completed taper (1068, 31.7%) Noncompleted taper (2303, 68.3%) Total (n = 3371) Demographical characterstics Age 20-44 99 (9.3%) 185 (8.0%) 284 (8.4%) 45-64 299 (28.0%) 770 (33.4%) 1069 (31.7%) 65-84 397 (37.2%) 934 (40.6%) 1331 (39.5%) ≥85 273 (25.6%) 414 (18.0%) 687 (20.4%) Sex* Male 399 (37.4%) 895 (38.9%) 1294 (38.4%) Female 668 (62.5%) 1408 (61.1%) 2076 (61.6%) Concessional beneficiary status† Nonbeneficiary 261 (24.4%) 517 (22.4%) 778 (23.1%) Beneficiary 807 (75.6%) 1786 (77.6%) 2593 (76.9%) Remoteness Regional and remote Australia 813 (76.1%) 1701 (73.9%) 2514 (74.6%) Major cities of Australia 255 (23.9%) 602 (26.1%) 857 (25.4%) Socioeconomic disadvantage Average SEIFA‡ score (SD) 6.25 (2.71) 6.11 (2.77) 6.15 (2.75) Measures of comorbidities Average number of comorbidities§ (SD) 6.24 (2.57) 6.43 (2.56) 6.37 (2.56) Average number of referrals to specialists (SD) 4.56 (7.86) 4.46 (7.13) 4.49 (7.37) Opioid characteristics Type of opioid Buprenorphine 229 (21.4%) 358 (15.5%) 587 (17.4%) Codeine and codeine combinations 268 (25.1%) 345 (15.0%) 613 (18.2%) Fentanyl 62 (5.8%) 232 (10.1%) 294 (8.7%) Hydromorphone 9 (0.8%) 21 (0.9%) 30 (0.9%) Methadone 9 (0.8%) 62 (2.7%) 71 (2.1%) Morphine Short-acting only 21 (2.0%) 12 (0.5%) 33 (1.0%) Long-acting‖ 31 (2.9%) 90 (3.9%) 121 (3.6%) Oxycodone Short-acting only 135 (12.6%) 477 (20.7%) 612 (18.2%) Long-acting‖ 46 (4.3%) 200 (8.7%) 246 (7.3%) Oxycodone–naloxone 248 (23.2%) 607 (26.4%) 855 (25.4%) Tapentadol Short-acting only 8 (0.7%) 13 (0.6%) 21 (0.6%) Long-acting‖ 90 (8.4%) 214 (9.3%) 304 (9.0%) Tramadol Short-acting only 20 (1.9%) 85 (3.7%) 105 (3.1%) Long-acting‖ 112 (10.5%) 421 (18.3%) 533 (15.8%) Average daily OME in mg (SD) 46.08 (66.82) 72.12 (80.22) 63.87 (77.18) Concurrent medicine use NSAIDs 107 (10.0%) 342 (14.9%) 449 (13.3%) Paracetamol 78 (7.3%) 177 (7.7%) 255 (7.6%) Gabapentinoids 72 (6.7%) 218 (9.5%) 290 (8.6%) Benzodiazepines 309 (28.9%) 750 (32.6%) 1059 (31.4%) Other services GP management plan 170 (15.9%) 391 (17.0%) 561 (16.6%) Referral to specialists Medical specialists 85 (8.0%) 268 (11.6%) 353 (10.5%) Surgical specialists 133 (12.5%) 327 (14.2%) 460 (13.6%) Allied health 195 (18.3%) 408 (17.7%) 603 (17.9%) Mental health and addiction 99 (9.3%) 214 (9.3%) 313 (9.3%)*There were missing data in one patient record.
†Beneficiaries may hold one of the following: (i) Commonwealth Seniors Health Card; (ii) Department of Veterans' Affairs Card; (iii) Healthcare Card; (iv) Pensioner Concession Card. Nonbeneficiary status was assumed if beneficiary status was not recorded in our data.
‡Socioeconomic Indexes for Areas deciles (SEIFA) is a measure of socioeconomic index derived from patient's postcode of residence. SEIFA is ranked on a scale of 1 to 10, with 1 indicating the most disadvantaged.
§Comorbidities were determined using the Rx-Risk Index.
‖Prescription of long-acting opioids with or without concurrent prescription of short-acting opioids.
GP, general practice; NSAIDs, nonsteroidal anti-inflammatory drugs; OME, oral morphine equivalents.
 Figure 3.:
Figure 3.: Opioid dose trajectory for completed and noncompleted taper groups. The average daily oral morphine equivalents (OME) of individuals in each taper group were determined and graphed. Periods 1 to 6 and periods 7 to 16 indicate overlapping the 90-day period during the baseline and the follow-up periods, respectively. As consecutive periods are overlapping, the index date falls between periods 5 and 7 (shaded in gray).
In patients who commenced opioid taper, oxycodone (25.5%) and oxycodone–naloxone (25.4%) were the most frequently prescribed opioids, followed by tramadol (18.9%) and codeine (18.2%, includes codeine in combinations with other analgesics). Buprenorphine (SA: 0.1%; LA: 17.4%) and fentanyl (SA: <0.1%; LA: 8.7%) were predominantly prescribed as LA formulations (with or without concurrent prescription of SA formulation), whilst oxycodone (SA: 18.2%; LA: 7.3%) was mostly prescribed as a SA formulation only. The average daily OME during the 6 months before taper was 46.08 mg (SD: 66.82) for those who successfully completed taper and 72.12 mg (SD: 80.22) for those who did not complete taper. Overall, almost a third of our samples were prescribed benzodiazepines (31.4%) in the first 3 months of commencing a taper, and 16.6% had a documented GP management plan. The most frequent referral was made to allied health professionals (17.9%) followed by surgical (13.6%) and medical specialists (10.5%).
3.2. Differences by opioid taper outcomeAfter controlling for demographic characteristics, comorbidities, and the average daily opioid dose during the 6 months before commencing taper, we found that compared with those who did not complete taper, patients who successfully completed taper were less likely to be prescribed buprenorphine (odds ratio [OR], 0.691; 95% CI: 0.530-0.901), fentanyl (OR, 0.429; 95% CI: 0.295-0.622), methadone (OR, 0.349; 95% CI: 0.157-0.774), oxycodone–naloxone (OR, 0.521; 95% CI: 0.407-0.669), and LA tapentadol (OR, 0.645; 95% CI: 0.461-0.902) and were more likely to be prescribed codeine (OR, 1.308; 95% CI: 1.036-1.652) (Fig. 4, Table S4, available at https://links.lww.com/PAIN/B969). Patients who completed taper were more likely to be prescribed SA morphine (OR, 3.534; 95% CI: 1.623-7.698) and less likely to be prescribed LA morphine (OR, 0.560; 95% CI: 0.346-0.907), compared with those who did not complete taper. Compared with those who did not complete taper, patients who successfully tapered were less likely to be prescribed any formulations of oxycodone (SA: OR, 0.533; 95% CI: 0.422-0.672, LA: OR, 0.356; 95% CI: 0.240-0.530) and tramadol (SA: OR, 0.370; 95% CI: 0.218-0.628, LA: OR, 0.317; 95% CI: 0.234-0.428). Compared with those who did not complete taper, those who successfully completed taper were less likely to be prescribed NSAIDs (OR, 0.645; 95% CI: 0.505-0.824) and less likely to be referred to medical specialists, which included pain specialists (OR, 0.725; 95% CI: 0.552-0.952).
 Figure 4.:
Figure 4.: Differences in opioid type and nonopioid interventions by opioid taper outcomes. The forest plot includes odds ratio and corresponding 95% confidence intervals for statistically significant values (highlighted in blue). After controlling for potential confounding variables including demographical characteristics, baseline opioid dose, and comorbidities, we assessed the predictors of opioid taper in the completed taper group compared with the noncompleted taper group (reference group). All predictors were examined as a binary variable. *Includes codeine combination with other analgesics. GP, general practitioner; LA, long-acting; NSAIDs, nonsteroidal anti-inflammatory drugs; SA, short-acting.
4. DiscussionWe examined opioid type and nonopioid interventions correlated with taper outcomes in a cohort of patients commencing taper from long-term opioid therapy. After controlling for comorbidities, average baseline opioid dose, and other factors known to affect taper outcomes, we found that patients who successfully completed taper were less likely to be prescribed most LA opioids. In the case of oxycodone and tramadol, both SA and LA formulations were inversely associated with successful taper, and only the prescription of codeine and SA morphine was associated with successful taper. Our study also showed that patients who completed taper were less likely to be prescribed NSAIDs and less likely to be referred to medical specialists; however, there is a possibility of reverse causation or confounding by indication, meaning these findings may not be conclusive. Nevertheless, we did not identify any adjunctive medication or referral type that supported a better taper outcome.
Given the observational nature of our study, we cannot determine whether there are causal relationships in our findings. Nevertheless, these key findings highlight a number of important factors that may be considered when designing studies to identify strategies to support better taper outcomes. First, pharmacokinetics of opioids used during taper seems to play a role in determining the taper outcome. Our study showed that patients who successfully completed taper were less likely to be prescribed most LA opioids. These included opioids which were formulated as a long-acting medicine (eg, extended-release tablets and transdermal patches) and those with a prolonged duration of action (eg, methadone). Whilst many guidelines do not provide clear recommendations on the use of SA vs LA opioids, rationalising all medications to a single LA opioid when tapering is one commonly recommended approach, which was inconsistent with our findings.30,37,50 Some guidelines discussed that LA opioids may enable less frequent dosing which could reduce psychological focus on opioids and patient's pill intake and help to maintain stable blood plasma levels around the clock.4,37,42 However, our study suggests that empirical evidence is needed to support such a recommendation in light of our findings. Recommendations around tapering SA opioids are also conflicting. A Canadian guidance on opioid tapering recommended against using SA opioids during a taper as fluctuations in dosing of SA opioids may delay the taper process, increase interdose withdrawal symptoms, and potentially cause inadvertent overdose from inconsistent consumption of SA opioids.37 Conversely, the taper guideline published by the Australian Therapeutic Goods Administration recommended tapering on SA opioid if patients are on higher doses of SA opioids.50 However, these recommendations were mostly based on anecdotal evidence or expert consensus, and current evidence around tapering SA and LA opioids (ie, whether to consolidate into a single opioid or whether to taper SA and LA opioids individually and in which order) is limited. Our findings suggest that carefully designed prospective studies comparing the outcomes of tapering on LA vs SA opioids are needed to better inform practice.
Second, our findings showed that patients who completed taper were less likely to be prescribed transdermal patches. Fixed patch strengths prevent incremental tapering of doses, especially at lower doses as the patches cannot be cut into smaller dosages, and difficulty predicting equianalgesic due to variability in transdermal absorption of opioids. This latter aspect is important to consider when switching to a different opioid, which may be required to do during a taper.12,36 Of note, evidence suggests that transition to buprenorphine, a partial mu-opioid agonist, may help patients taper from high-dose full-agonist opioid treatments in chronic pain.43,48 However, these studies focus on the use of sublingual and buccal tablets. In our study, buprenorphine was predominantly prescribed as a transdermal patch and was found to be inversely associated with successful taper. This finding suggests that not only the type of opioid (ie, partial vs full mu-opioid agonist) but also the mode of delivery may be important in determining the taper outcome.
Third, even after controlling for baseline characteristics including opioid dose and comorbidities, the prescription of codeine was associated with successful opioid taper, whilst the prescription of oxycodone and tramadol, regardless of their formulations, was less likely to be correlated with successful taper. Similar findings were reported in an Australian study, where oxycodone was found to be the most commonly dispensed opioid among persistent users, while paracetamol/codeine was found to be the most commonly dispensed opioid among nonpersistent users.31 Despite reports of codeine misuse and harms and high rates of patients seeking treatment from codeine dependence,8,40 our study showed that patients who were prescribed codeine in the 3 months after the commencement of taper were able to completely taper. Conversely, there are some studies suggesting that oxycodone and tramadol are more likely to predict persistence compared with other opioids such as tapentadol or other short-acting opioids.33,51 Further comparative studies focusing on opioids prescribed during long-term opioid therapy are urgently needed, especially as these are one of the most commonly prescribed opioids globally.25
Fourth, contrary to many guideline recommendations on maximising nonopioid interventions to support opioid taper, our findings showed that the prescription of NSAIDs and referral to medical specialists were inversely associated with successful taper. However, this finding should be interpreted with caution, given the observational study design and the possibility of reverse causation. For example, patients not experiencing any withdrawal symptoms during taper may not have needed concurrent use of NSAIDs or pain medicine specialist input. In addition, prescription of medicines that are available over the counter such as NSAIDs may not be fully captured in our prescribing data. Similarly, referral data may not accurately reflect patient uptake of specialist service. In Australia, GP referral is required to seek certain healthcare specialist services (eg, pain management), and there may be a time lag between the time a referral was made and the time of specialist consultation. For other specialist services (eg, physiotherapy), referrals are not a requirement. Therefore, we cannot confirm whether patients sought help without a referral or whether they ultimately received the specialist services they were referred to. Moreover, specialist pain services are very difficult to access with long waiting lists. We did not find any positive association with any individual medication class or referral type in supporting a better taper outcome to inform a hypothesis that might be explored through prospective study design. However, future studies could explore whether any combinations of nonopioid interventions may be associated with successful opioid taper, given the growing evidence for more complex pain management regimes.18,47
4.1. Strengths and limitationsThis study should be interpreted in context of its strengths and limitations. First, our study consisted of one of the largest Australian primary care cohorts prescribed opioid analgesics. This data set included rich patient-level information, enabling key confounders to be controlled for, and prescribing of all opioids, irrespective of their subsidy status. As our analyses used prescribing data, we cannot confirm whether the prescribed opioids were dispensed or taken; however, as our study ensured continuous prescriptions, it is reasonable to assume there was ongoing opioid use. Second, an individual patient's length of prior opioid use may have an impact on the taper outcome.45 It is possible that those on opioids for much longer periods before taper may have different outcomes. Although it was not possible to determine the length of prior opioid use using our data, our study cohort was selected using strict criteria of opioid prescribing of at least 6 months to minimize heterogeneity and to ensure selection of patients at the point of taper from a stable dose, long-term opioid therapy. Third, completed vs noncompleted taper groups were determined through group-based trajectory modelling, which classifies all patients into a trajectory, meaning that some patients may be forced into trajectories that do not optimally represent their opioid dose patterns. However, model fit indices suggest that this is unlikely (see Supplement Methods for further details, available at https://links.lww.com/PAIN/B969). Fourth, as extreme values of the OME were imputed to a maximum dose of 250 mg of average daily OME, our findings may not be generalisable to those prescribed very high doses. More nuanced research examining these high opioid dose ranges may be needed, particularly given greater risks associated with prescription of high opioid doses. Fifth, we controlled for comorbidities using Rx-Risk Index, which categorises comorbidities into 46 comorbidity categories.44 This means that different types of pain diagnoses are coded under the same category of “pain,” and patients with multiple pain diagnoses would have the same comorbidity index as those having one pain diagnoses. Further research may be needed to explore whether specific pain diagnoses or the number of pain diagnoses influence taper outcomes.
5. ConclusionIn conclusion, this study adds to the very limited literature that identifies medication and other clinical factors associated with completion of an opioid taper. We found that patients who completed opioid taper were less likely to be prescribed most LA opioids, oxycodone or tramadol, but more likely to be prescribed codeine in the 3 months after commencement of taper. Examination of concurrent prescription of other medicines and referral to other healthcare professionals was limited by the observational study design but did not identify any factors that seemed to support better taper outcomes.
Conflict of interest statementS.N. has received unrelated untied research funding from Seqirus to examine pharmaceutical opioid-related harms and is a named investigator on a research grant from Indivior for an implementation trial of buprenorphine depot (no funding received). J.I. has grants from Amgen and AstraZenica unrelated to this research topic. All other authors have no conflicts of interest to declare.
Appendix A. Supplemental digital contentSupplemental digital content associated with this article can be found online at https://links.lww.com/PAIN/B969.
AcknowledgementsThe authors acknowledge Outcome Health and the participating Primary Health Networks (Eastern Melbourne, South Eastern Melbourne, and Gippsland Primary Health Networks) for provision of the data.
Author contributions: All authors contributed to the study conception and design. M.J. cleaned and analysed the data with assistance from T.X. and S.N. M.J. produced the first draft of the manuscript. All authors reviewed, provided feedback, and approved the final version of the manuscript.
The project is funded by the Australian National Health and Medical Research Council (#2002193). M.J. is a recipient of PhD Scholarship from the Monash Addiction Research Centre.
Data availability statement: The data that support the findings of this study can be requested from Outcome Health, the data custodians.
References [1]. Ackermann E, Litt J, Morgan M. Prescribing drugs of dependence in general practice, part C2: The role of opioids in pain management. East Melbourne (AU). The Royal Australian College of General Practitioners, 2017. Available at: https://www.racgp.org.au/FSDEDEV/media/documents/Clinical%20Resources/Guidelines/Drugs%20of%20dependence/Prescribing-drugs-of-dependence-in-general-practice-Part-C2.PDF. Accessed November 29, 2023. [2]. Agnoli A, Xing G, Tancredi DJ, Magnan E, Jerant A, Fenton JJ. Association of dose tapering with overdose or mental health crisis among patients prescribed long-term opioids. JAMA 2021;326:411–9. [3]. Aguinis H, Gottfredson RK, Joo H. Best-practice recommendations for defining, identifying, and handling outliers. Organizational Res Methods 2013;16:270–301. [4]. Argoff CE, Silvershein DI. A comparison of long- and short-acting opioids for the treatment of chronic noncancer pain: tailoring therapy to meet patient needs. Mayo Clin Proc 2009;84:602–12. [5]. Australian Institute of Health and Welfare (AIHW). Chronic pain in Australia. Canberra: AIHW, 2020. [6]. Australian Institute of Health and Welfare (AIHW). Opioid harm in Australia and comparisons between Australia and Canada. Cat. no. HSE 210. Canberra: AIHW, 2018. [7]. Busse JW, Craigie S, Juurlink DN, Buckley DN, Wang L, Couban RJ, Agoritsas T, Akl EA, Carrasco-Labra A, Cooper L, Cull C, da Costa BR, Frank JW, Grant G, Iorio A, Persaud N, Stern S, Tugwell P, Vandvik PO, Guyatt GH. Guideline for opioid therapy and chronic noncancer pain. CMAJ 2017;189:E659–66. [8]. Cairns R, Schaffer AL, Brown JA, Pearson SA, Buckley NA. Codeine use and harms in Australia: evaluating the effects of re-scheduling. Addiction 2020;115:451–9. [9]. Cangadis-Douglass H, Jung M, Xia T, Buchbinder R, Lalic S, Russell G, Andrew N, Pearce C, Bell JS, Ilomäki J, Nielsen S. Using primary care data to understand opioid prescribing, policy impacts and clinical outcomes: a protocol for the OPPICO study. Res Soc Adm Pharm 2022;18:4129–37. [10]. Chou R, Turner JA, Devine EB, Hansen RN, Sullivan SD, Blazina I, Dana T, Bougatsos C, Deyo RA. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med 2015;162:276–86. [11]. Curtis HJ, Croker R, Walker AJ, Richards GC, Quinlan J, Goldacre B. Opioid prescribing trends and geographical variation in England, 1998-2018: a retrospective database study. Lancet Psychiatry 2019;6:140–50. [12]. Davis MP, Digwood G, Mehta Z, McPherson ML. Tapering opioids: a comprehensive qualitative review. Ann Palliat Med 2020;9:586–610. [13]. Degenhardt L, Grebely J, Stone J, Hickman M, Vickerman P, Marshall BDL, Bruneau J, Altice FL, Henderson G, Rahimi-Movaghar A, Larney S. Global patterns of opioid use and dependence: harms to populations, interventions, and future action. Lancet 2019;394:1560–79. [14]. Donovan PJ, Arroyo D, Pattullo C, Bell A. Trends in opioid prescribing in Australia: a systematic review. Aust Health Rev 2020;44:277–87. [15]. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. JAMA 2016;315:1624–45. [16]. Dowell D, Haegerich TM. Changing the conversation about opioid tapering. Ann Intern Med 2017;167:208–9. [17]. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain—United States, 2022. MMWR Recomm Rep 2022;71:1–95.
留言 (0)