
記住我


Many chronic pain conditions show striking differences between men and women in key disease aspects, such as prevalence, duration, intensity of symptoms, or treatment efficacy.19,34,65,69,96 Several sociocultural, educational, biological, and aethiopathological factors contributing to chronic pain have been identified to differ between men and women.8,45,63,66,71,81 An important question regarding many of these factors is whether they differ before pain onset because factors that do differ might contribute to the increased vulnerability of women for chronic pain.69,74,75
One important mechanism, observed to differ between men and women in certain chronic pain conditions, is central sensitization (CS),6,10,25,35,91 defined as an increased responsiveness of second-order neurons in the dorsal horn to normal or subthreshold afferent input.61 Yet, it is unknown whether CS differences are already present in healthy men and women, ie, before any potential pain chronification sets in. 49 Because increased responsiveness of second-order neurons cannot be directly investigated in humans, proxy measurements of CS are used.4,64,73,102
Increased mechanical sensitivity adjacent to the primary area of noxious stimulation is one well-established proxy for measuring CS (CS proxy). It is typically recorded as secondary mechanical hyperalgesia (SMH) or dynamic mechanical allodynia (DMA).20,73,83,102 Such measurements rely on cooperation and feedback from the tested person.42 Therefore, the measures are potentially subject to factors influencing response behaviour in the tested person, such as disposition, motivation, expectation, or interaction, with the experimenter that can vary between men and women.21,22,30,46,106 Studies investigating potential differences of subjective CS proxies between healthy men and women have so far been inconclusive.38,39,48 More objective CS proxies, such as the nociceptive withdrawal reflex (NWR), are an alternative to investigate potential sex differences of CS.
The NWR is a polysynaptic spinal response to an external noxious stimulus resulting in involuntary muscle activation to withdraw the affected limb, which can be measured by surface electromyographical recording (sEMG).90,100 The NWR has been used to study spinal hyperexcitability in chronic pain patients and healthy volunteers.3,7,13,15,16,72,86,99 Its characteristics, including threshold and magnitude, do not differ between healthy men and women26,67 and neither seem to be influenced by menstrual cycle phases.9,76 Importantly, supraspinal influences on the NWR17,29,84,95,101 do not differ between men and women.79 In addition, this motivates the NWR for the investigation of potential sex-specific differences in CS.
This study combined 2 objective CS proxies, the magnitude also known as reflex size (NWR-M) and the response rate (NWR-RR) of the NWR, with 2 subjective ones (SMH and DMA) to compare experimentally induced CS in healthy men and women. A previously published CS induction protocol using noxious heat51 was applied on the lateral foot dorsum distal to the lateral malleolus. A sham protocol was applied to the contralateral foot.
The primary objective of the study was to test if differences in CS proxies would be observed between healthy men and women. The secondary objective was to test whether subjective (SMH and DMA) and objective (NWR-M and NWR-RR) CS proxies would show diverging results.
2. Material and methods 2.1. General study designThe study followed a within-subject design with 2 experimentally induced conditions: heat pain and sham. Heat pain was induced by applying a noxious heat protocol on the lateral dorsum of the left or the right foot (test site) distal to the lateral malleolus. Sham was induced on the contralateral foot (control site). The conditions were induced consecutively. Mechanical sensitivity testing adjacent to the primary application area to investigate SMH and DMA and electrical stimulation at the retromalleolar pathway of the sural nerve to elicit the NWR were performed before and 20 minutes after each induction protocol for both the test leg and the control leg.89 Anthropometric data were collected right before testing. The order of the conditions, ie, starting with heat pain or sham, and the choice of test and control site, left or right, were pseudorandomly counterbalanced across participants. The study consisted of one visit, lasting about 3 hours. The experimental session took place either in the morning or in the afternoon with participants being pseudorandomly assigned a session time to minimize the influence of day time on the results.57,86 Written informed consent was obtained from all participants.
The study was approved by the Ethical Board of the Canton of Zurich (Kantonale Ethikkomission Zürich) and registered at clinicaltrials.gov (NCT05031286). The study was conducted in accordance with the Declaration of Helsinki.
2.2. ParticipantsThe study sample was restricted to men and women in good general health and with a body mass index (BMI) ≤ 30. The age range of participants was limited to 18 to 40 years to reduce influences of age on the mechanisms of interest. For practical reasons (see 2.3.1), only participants with shoe sizes ≥ 38 Paris points, the common measuring unit in continental Europe, were included. Based on results for SMH in pilot experiments for establishing the study design, a sample size of 66 with an equal number of men and women was determined with a 2-sided t test using an effect size of 0.7, a significance level of 0.05, and a power of 0.8.
2.2.1. Exclusion criteriaIndividuals with any major medical or psychiatric condition, any chronic pain condition, back pain for more than 3 consecutive days over the past 3 months, intake of any analgesics, or consumption of any stimulants in the past 24 hours before the experiment, or with scar tissue in the testing areas were excluded from study participation.
If a participant was unable to endure the thermal protocols or the electrical stimulations, or if the NWR threshold could not be detected (see 2.3.5), the experiment was terminated, and the participant excluded and replaced with respect to calculated sample size.
Participants with NWR-RR <66% at the biceps femoris for either of the 2 stimulation currents before heat pain were excluded from further analysis and replaced not to bias a potential influence on the NWR characteristics by relying on a low number of data points. This meant that participants with a particularly low NWR-RR at baseline would not inflate any potential NWR-RR increase after heat pain.
2.3. Experimental procedures 2.3.1. Participant setupThe setup followed a previously published protocol where participants sat on a test bed, with the back rest inclined at 60°, their legs comfortably extended, and a towel placed below their knees.43
2.3.2. FamiliarizationBefore the experiment, participants were familiarized with all testing modalities. For the thermal stimuli, a 3 cm × 3 cm computer controlled peltier thermode (Pathway Pain & Sensory Evolution System, Medoc, St. Ramat Yishai, IL) was attached to the lower forearm on the same side before temperatures of 40, 43, 46, and 48.5°C were each applied thrice in a row for 6 seconds using an up–down ramp of 10°C/s, a baseline temperature of 32°C, and a break of 30 seconds after each temperature. For mechanical sensitivity testing, the 2 testing measures, a 256 mN calibrated von Frey filament with a 0.5-mm blunted tip (Optihair-2, Marstock, Schriesheim, Germany), and a soft brush (200-400 mN, Brush-05, SoMedic SENSELab AB, Sösdala, Sweden) were demonstrated on the dorsum of the nondominant hand. Familiarization with the electrical stimulations for NWR elicitation took place right before the first NWR assessment and consisted of a 4-mA electrical stimulation of the same type as used for the subsequent NWR assessments (see 2.3.5).
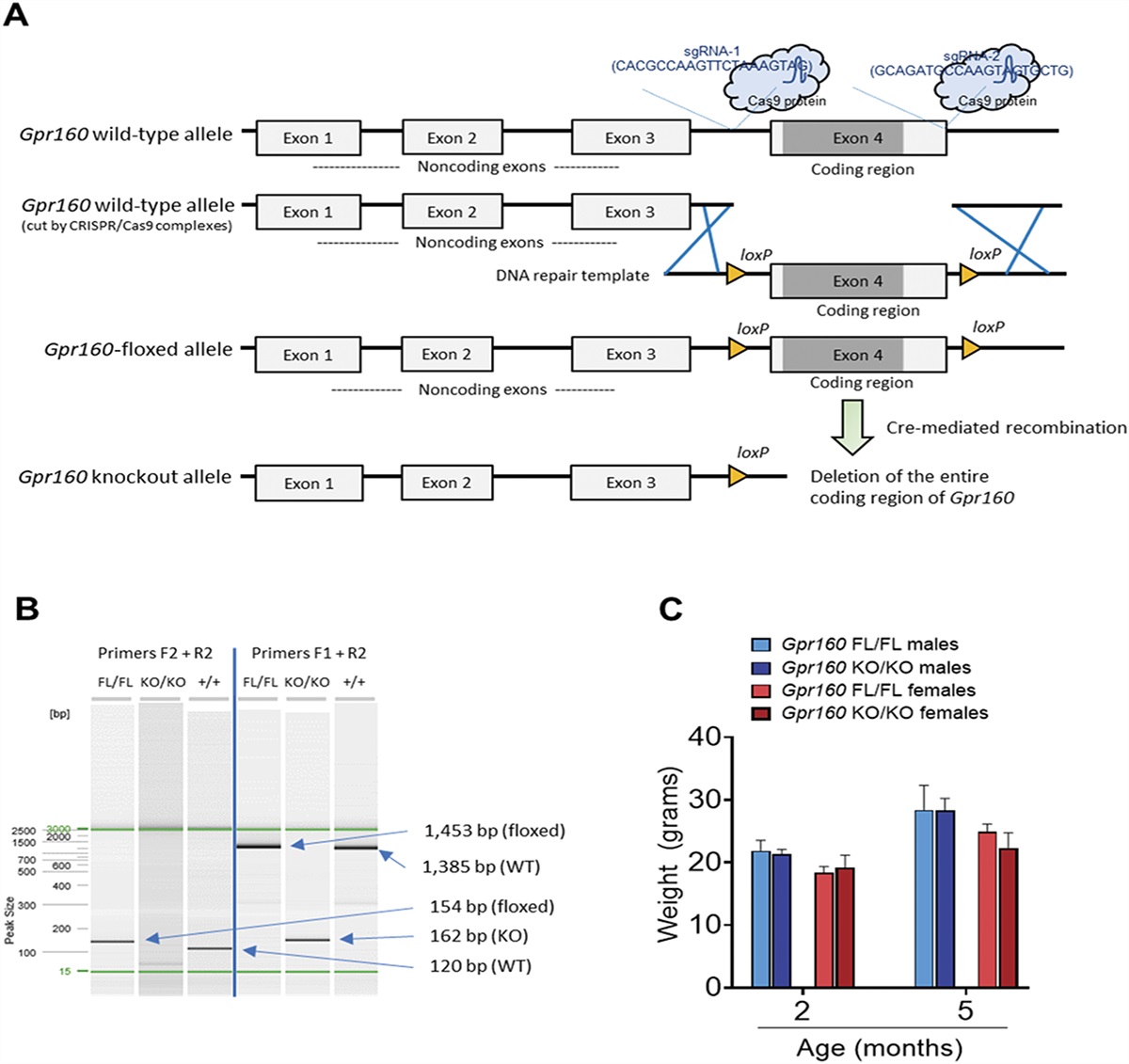
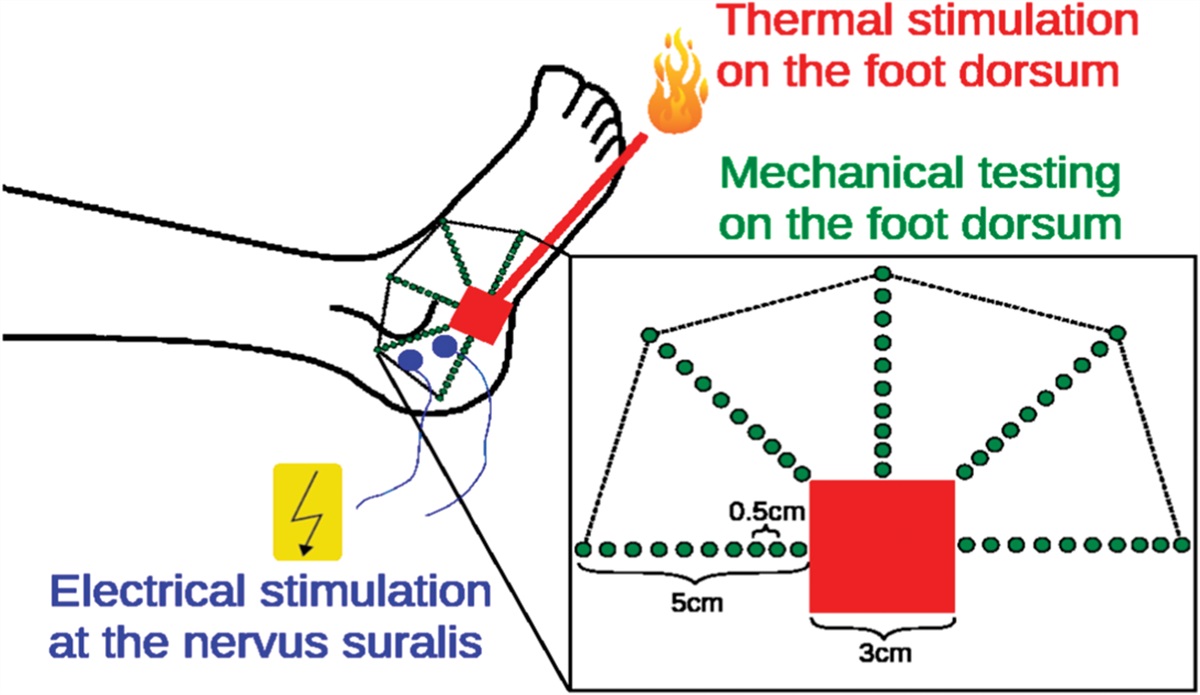
2.3.3. Thermal protocolsThe thermal stimuli of the 2 protocols to induce heat pain and sham were applied with the thermode attached to the lateral side of the foot dorsum distal to the lateral malleolus (Fig. 1).
 Figure 1.:
Figure 1.: Mechanical sensitivity testing and stimulation sites.
For heat pain, a previously published protocol for thermal CS induction, validated on the volar forearm,51,89 was employed. It consists of 10 blocks of 6 noxious heat stimuli of 48°C for 6 seconds each with pauses of 30 seconds at 32°C baseline temperature between the blocks. An up–down ramp of 10°C/s is used (see earlier studies51, 89 for details). Beforehand, the individual heat pain threshold was determined at the same location using a validated protocol.83 For sham, the protocol was analogous but with the thermode remaining at baseline temperature the whole time.
Participants were instructed to concentrate on the stimuli to rate the mean intensity per stimulation block on a numerical scale from 0 (no sensation) to 200 (most intense pain tolerable), with 100 corresponding to the pain threshold. The ratings only served to direct the participant's attention towards the thermally stimulated region because spatial attention during CS induction has been shown to facilitate SMH.33
2.3.4. Mechanical sensitivity testingTo assess mechanical sensitivity, the 2 testing measures were used in the area adjacent to the thermode on the foot dorsum (Fig. 1).51,83 On the one hand, the punctuate stimulus of the von Frey filament was applied to the skin. On the other hand, a light stroking movement with the soft brush was performed. The application order of the 2 testing modalities, starting with brush or filament testing, was pseudorandomly counterbalanced across participants.
The 2 assessments were performed along 5 testing lines. Starting from the edges of the thermode position, 5 radial dotted lines of 5-cm length were marked on the foot dorsum at 45° interline angle with dots interspaced every 5 mm (Fig. 1). To ensure the necessary testing surface and sufficient space for the thermode, participants needed to have at least a shoe size of ≥38 Paris points.
The von Frey filament was applied on the marked spots along the 5 testing lines. The soft brush was applied on the lines by stroking the brush over the distance of 2 spots, ie, using 5 strokes in total. Both mechanical sensitivity assessments always began at the outermost spot, which lay outside a potential area of sensitization as established in pilot experiments, moving inwards in intervals of 2 seconds. Testing was stopped whenever the participant reported a definite change in sensation relative to the outermost point for 2 consecutive spots or one stroke, respectively, such as a clearly stronger or weaker perception of the stimulus applied by the testing instrument (von Frey filament or brush) to the skin. The location of the first such spot and the type of change (eg, stronger or weaker) were recorded. The spots where the sensation was perceived as stronger along the testing lines were connected, and the areas between these connected lines and the edges of the thermode (Fig. 1) were considered the area of SMH and DMA, respectively. During mechanical sensitivity testing, participants were instructed to keep their eyes closed.
2.3.5. Nociceptive withdrawal reflex assessmentsTwo measures of the NWR, NWR-M and NWR-RR, were assessed. In studies of experimentally induced CS, NWR-M is often used as an objective CS proxy. To that end, NWR-M is assessed before and after CS induction within the same dermatome where the induction paradigm was performed using repetitive NWR elicitations.13,28,31,43,59 The procedure also allows to assess the NWR response rate (NWR-RR), ie, the percentage of obtained reflexes, which has recently been proposed as an objective CS proxy.43 Studying changes in NWR-RR corresponds to indirectly testing for a modulation of the NWR threshold current, the minimum electrical current necessary to elicit a reflex response.
The NWR threshold current is often used to study CS processes, particularly in clinical populations3,14,16,29,59,85 albeit with sometimes inconclusive results with respect to potential differences between chronic pain patients and healthy controls.2,60,103 The threshold needs to be separately determined requiring an individually varying number of electrical stimulations. This can lead to different numbers of applied stimulations across participants. The applied number of stimulations is considered one key factor contributing to the habituation of the NWR, an observed decrease in reflex responses and magnitude over the course of an experiment.3,27,86,98
Contrariwise, no separate testing is required to obtain the NWR-RR. It can be directly calculated from the data. By definition, any meaningful change in threshold is also reflected in the NWR-RR, which either increases or decreases accordingly, because the number of elicited reflex responses correlates with the applied current with respect to threshold.43,86,98,100 Assessing the NWR-RR thus yields the same information as separate threshold testing without the problem of the number of stimulations potentially differing across participants.
For the present NWR assessments, transcutaneous constant electrical current stimulations and sEMG recordings were performed using a Dantec Keypoint© G4 EMG/EP Workstation (Natus Medical Inc, San Carlos, CA).
The stimulations were applied over the retromalleolar pathway of the sural nerve, and sEMG recordings were obtained from biceps femoris, rectus femoris, and tibialis anterior muscles according to a previously published protocol.43 The recording window extended from 120 milliseconds prestimulation to 380 milliseconds poststimulation. Every electrical stimulation consisted of a train of 5 rectangular stimuli of 1-millisecond duration delivered at 200 Hz.
At each of the sEMG recording sites, 2 Ambu (Ambu A/S, Copenhagen, DK) Blue Sensor NF-50 1.5-mm surface electrodes were attached, one on the muscle belly and one near the tendon insertion. Before attaching the electrodes, the skin was cleaned with ethanol and exfoliated with Nuprep gel (Weaver and Company, Aurora, CO) to achieve impedances below 10 kΩ. For the electrical stimulations, 2 Ambu Neuroline 700 2-mm surface electrodes were placed 2 cm apart over the retromalleolar pathway of the sural nerve.
The NWR was always assessed after mechanical sensitivity testing to avoid a potential influence on SMH and DMA. This precaution was deemed necessary because electrical stimulations have been shown to cause sensitization within the same dermatome of their application.12,13,28,59,73
First, the NWR threshold at the biceps femoris was determined. It was defined as the higher of the single stimulation and 3-stimulation threshold. The single stimulation threshold is the lowest current to reliably elicit a reflex with a single electrical stimulation. The 3-stimulation threshold refers to the third stimulation in a triplet of identical electrical stimulations delivered at 2 Hz. It is the lowest current to reliably elicit a reflex with the third stimulation of such a triplet.80,94,95 In both, a single ascending staircase78 was used with increments of 1 mA starting at 1 mA until the first reflex was reached and continued for 4 more increments for validation but not higher than 25 mA. Reflexes were identified using predefined automated scoring criteria (see 2.4.2).
Following NWR threshold determination, 30 suprathreshold stimulations were applied, 15 at 120% and 15 at 140% NWR threshold. The stimulation order was randomized with the limitation that no more than 5 identical stimulations would be applied consecutively. The interstimulation interval was randomly varied between 5 and 15 seconds. Participants were asked to distract themselves with their cell phones during the stimulations because a distraction-related facilitation of the NWR has been proposed.95
2.4. Data analysisThe primary objective of this study was to test for potential differences in 4 CS proxies (SMH, DMA, NWR-M, and NWR-RR) between men and women. Therefore, it was assessed whether an effect on these proxies was observable within condition, ie, comparing the measures before and 20 minutes after the application of the respective induction protocol, as well as between the conditions, ie, testing if the effects differed between heat pain and sham. Effect size was calculated as Cohen d and interpreted accordingly.23,88 Any relevant cohort characteristics, such as anthropometric data and heat pain threshold, were compared between men and women because differences have been reported to impact sensitization processes and the NWR.86
2.4.1. Sensitized skin areaThe extent of sensitized skin area outside the primary stimulation area before and 20 minutes after protocol application was defined as the skin area adjacent to the thermode limited by the points for which participants reported a definite change in sensation and the edges of the thermode. The outermost points on each radial line for which a change is reported are connected, and the skin area is calculated as if it were a flat surface. Although such a calculation ignores the individual curvature of the foot dorsum, the deviation from the real area is negligibly small. To account for individual foot length the relative area, defined as the calculated area in square centimeters divided by the shoe size according to the Continental European System in half units, was evaluated as well.
2.4.2. Nociceptive withdrawal reflexesThe sEMG signals were sampled at 48 kHz and downsampled to 6 kHz, rectified, band-pass filtered from 10 Hz to 500 Hz, and amplified up to 125 times. From −120 milliseconds prestimulation to 380 milliseconds poststimulation, traces were automatically saved into separate text files (txt). For reflex identification, 2 well-established, automated, scoring criteria were used: the NWR interval Z score (Z) and the NWR Cohen d (D). Z is defined as the mean of the 90 to 150 milliseconds poststimulation amplitude and the mean of the 80 to 20 milliseconds prestimulation amplitude divided by the standard deviation of the 80 to 20 milliseconds prestimulation amplitude.36,77 D differs from Z only by the denominator, which is the pooled standard deviation of the 80 to 20 milliseconds prestimulation and 90 to 150 milliseconds poststimulation amplitude.36,77 Using both, Z and D as scoring criteria minimizes false classification of reflexes, which can be in the range of up to 5% because of contamination of the EMG traces by spontaneous muscle activation.43 Furthermore, all traces were also visually inspected by the experimenters.
For all analyses, biceps femoris and rectus femoris were separated because this study was not designed to assess the NWR on the basis of muscle synergies, which would typically require more recording sites.50 Tibialis anterior recordings were not analysed in this study because they were collected for an unrelated research question.
Nociceptive withdrawal reflex magnitude was quantified with D. To assess condition effect, individual effect sizes were calculated to account for interindividual and intraindividual differences in NWR-RR. Statistical analyses were always performed separately for the 2 relative stimulation currents to avoid distorting the result ranges by pooling the data.
2.4.3. Statistical analysisAnthropometric characteristics, mechanical sensitivity testing results, and all data extracted from sEMG traces were stored in comma separated values (csv) files. All data analysis was performed in R 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria) using the “tidyverse” collection of packages and the packages coda 0.19-4, Bayesian estimation testing (BEST) 0.5.4, rjags 4.13, and runjags 2.2.1-7 relying on JAGS 4.3.0. A Bayesian analytical framework was used for statistical testing. Bayesian statistical analyses do require less assumptions on data distribution and outliers. Instead of point estimates, posterior distributions are obtained for the parameters of interest based on the original data. These distributions are then used to make inferences. Furthermore, they allow for clear-cut probabilistic interpretations and do not rely on significance testing.54 The recommended reporting guidelines for Bayesian statistical analyses56 were observed whenever applicable.
Unless explicitly stated otherwise, comparisons were made with BEST, whereby the data to be compared is described by t distributions whose parameters are estimated using Bayesian inference. Bayesian estimation testing is a robust method to determine differences between groups that yields more easily interpretable information than frequentist comparisons, eg, the t test.53 Bayesian estimation testing was directly performed in JAGS and using the package BEST 0.5.4 in R. Broad uninformed priors were implemented. Three sampling chains with 50,000 iterations, a burnin of 5000, and a thinning factor of 5 were used to calculate posterior distributions. Convergence of sampling chains was accepted for a Brooks–Gelman–Rubin scale reduction factor <1.1.40
Interpretations and probabilistic analyses focussed on the 95% highest density interval (HDI95) of the posterior distributions and its median value. If HDI95 included 0, the results were not considered statistically meaningful. To gauge the clinical relevance of the results, a region of practical equivalence (ROPE) was applied before calculating the probabilities for statistical differences.55 For the extent of sensitized skin, the ROPE was set to ±0.5 cm2. Such a ROPE reflects the potential imprecision of the experimenter during testing along the marked spots. For between-condition comparisons of NWR-M, a ROPE of ±0.1 was set because such a small difference in effect would be considered clinically irrelevant. In the same vein, the probabilistic analysis was restricted to differences >0.2. Identical restrictions were implemented for the within-condition comparisons (men − women) of NWR-M.
For both conditions (heat pain and sham), individual effect sizes were calculated for the NWR-M at the biceps femoris and at the rectus femoris with respect to relative stimulation current. These values were then entered into a Bayesian normal–normal model with uninformed priors to determine the HDI95 and the respective probability of an effect. Alternatively, these group-level results for men and women can be obtained from a simple Bayesian hierarchical model with uninformed priors.
For NWR-RR, Bayesian beta-binomial models were used to determine the respective ranges (HDI95) before and after protocol application. Changes between before and after protocol application were assessed by calculating greater effectiveness defined as 1 minus the rate of the 2 calculated ranges.43 The ROPE was set to ±0.07 because a greater effectiveness of ± 7% or less would correspond to changes of not more than 1 reflex. Such a change in NWR-RR was not considered clinically relevant.
3. ResultsIn total, 95 subjects were recruited. Two (1 m + 1w) were not included due to the presence of exclusion criteria that had been missed upon first contact: scar tissue in the testing area and BMI > 30, respectively. Sixteen participants aborted the experiment because of not tolerating the applied stimuli, 11 (8 m + 3 w) during familiarization of the heat-pain stimuli, 1(1 m) during NWR threshold assessment, and 4 (2 m + 2 w) during heat pain induction. A further (2 m + 1 w) 3 had to be excluded after data collection, 2 because of protocol violations by the experimenter, and 1 because of belatedly disclosed pain killer consumption within 24 hours before the experiment. The study cohort thus consisted of 74 included participants who finished the experiment and whose data were analysed. A further 8 (6 m + 2 w) participants were excluded following preliminary data analysis because of NWR-RR < 66%, leaving a final cohort of 66 participants, 33 men and 33 women.
3.1. Participant characteristicsTable 1 shows the characteristics of the 66 included participants at baseline, ie, before the application of the thermal protocols. The statistically meaningful differences in height, weight, BMI, and shoe size between men and women were expected because of the respective distributions in the general healthy population. Neither heat pain threshold nor reflex thresholds differed between men and women. Stimuli ratings during the thermal induction protocols also did not differ between men and women for any of the 10 blocks (Table 2).
Table 1 - Characteristics of the final study cohort (n = 66 [33 m + 33 w]). Full cohort (mean ± SD) Men (mean ± SD) Women (mean ± SD) HDI95 (men − women) Age [y] 26.3 ± 4.6 27.3 ± 4.6 25.4 ± 4.5 −0.73, 3.83 Height [cm] 173.9 ± 9.5 180.0 ± 8.4 167.8 ± 6.0 8.5, 15.9 Weight [kg] 67.0 ± 12.1 75.0 ± 11.0 59.0 ± 6.8 11.5, 12.8 BMI [kg/m2] 22.0 ± 2.7 23.1 ± 2.8 20.9 ± 2.1 1.0, 3.5 Shoe size [Paris points] 41.1 ± 2.7 43.3 ± 1.9 38.9 ± 1.1 3.6, 5.2 HPT [°C] (n = 64 [32 m +32 w]) 43.8 ± 3.1 43.4 ± 3.4 44.2 ± 2.7 −2.3, 0.7 NWR threshold current [A] test leg 11.6 ± 4.3 11.3 ± 4.1 11.9 ± 4.5 −1.5, 2.9 NWR threshold current [A] control leg 10.9 ± 4.1 10.5 ± 3.8 11.3 ± 4.5 −1.3, 3.0The outermost column shows the HDI95 for the difference in means (men − women) after Bayesian estimation testing. HPT was only available for 64 (32 men and 32 women) out of 66 participants due to incomplete data collection. Bold HDI95 values indicate statistically meaningful differences.
A, ampère; BMI, body mass index; cm, centimetres; HDI95, 95% highest density interval for difference in means (men − women) of Bayesian posterior distributions; HPT, heat pain threshold; m, men; NWR, nociceptive withdrawal reflex; Paris points, continental European shoe size; w, women.
Intensity ratings on a scale from 0 (no sensation) to 200 (most intense pain tolerable) with 100 = pain threshold. All values given as mean ± standard deviation.
Of the 2 subjective proxies, SMH was reliably detected for heat pain in all but 3 participants. Furthermore, SMH was higher in women than in men. Dynamic mechanical allodynia could only be detected in a small minority of participants.
Before protocol application, none of the participants reported any sensitized skin when mechanical stimulations were applied. This remained unchanged for sham. However, 63 (30 men and 33 women) of 66 participants experienced a definite change in sensation (stronger perception) when being tested with the von Frey filament for heat pain, indicating the presence of SMH. No weaker perception was reported by participants. By contrast, only 19 (9 men and 10 women) presented signs of DMA with brush testing. Table 3 shows the calculated extent in sensitized skin area for heat pain.
Table 3 - Extent of sensitized skin 20 minutes after heat pain protocol. Full cohort (mean ± SD) Men (mean ± SD) Women (mean ± SD) HDI95 (men − women) SMH [cm2] (n = 63 [30 m + 33 w]) 9.97 ± 7.63 7.81 ± 6.56 12.13 ± 8.12 −8.09, −0.54 DMA [cm2] (n = 19 [9 m + 10 w]) 1.06 ± 2.09 1.17 ± 2.45 0.95 ± 1.68 −3 × 10−3, 3 × 10−3Bold HDI95 values indicate statistically meaningful differences.
cm, centimetres; DMA, extent of dynamic mechanical allodynia after brush stroke; HDI95, 95% highest density interval for difference in means (men − women) of posterior distributions after Bayesian estimation testing; SMH, extent of secondary mechanical hyperalgesia after von Frey filament application.
For SMH, the effect size for the full cohort was 1.85. However, the extent of sensitized skin greatly differed between men and women with group effect sizes of 1.68 and 2.11, respectively, which were confirmed by BEST (median values of 1.67 and 2.10). On average, the extent was greater by 4.31 cm2 in women than in men. The probability of women presenting a greater extent of sensitized skin was 95.7%. The relative difference remained unchanged when shoe size was taken into account (data not shown). Figure 2 shows the posterior distributions after BEST for the extent of SMH for men and women with median values of 7.64 cm2 for men and 11.99 cm2 for women, confirming the experimental data (7.81 and 12.13 cm2).
 Figure 2.:
Figure 2.: Bayesian posterior distributions of secondary mechanical hyperalgesia 20 minutes after heat pain protocol, with dashed lines indicating means.
For DMA, the difference in sensitized skin area was negligible with BEST revealing a null effect. Median values after BEST were 0 for both groups as expected from the low number of participants reporting sensitized skin to brush strokes and mean extent of 0 cm2 in the data. This is in line with the literature,73 and DMA was therefore not further analysed.
3.3. Reflex assessmentsSummarizing the results for the 2 objective proxies, a statistically meaningful effect of heat pain on NWR-M was observed in women for both relative stimulation currents and at both recording sites with median effect sizes between 0.31 and 0.36. However, between-condition differences (heat pain − sham) were only statistically meaningful at the biceps femoris. In men, no statistically meaningful effect of heat pain on NWR-M was observable with median effect sizes between 0.12 and 0.29. In addition, within-condition differences between men and women were not meaningful. At the rectus femoris, NWR-RR showed increases for heat pain in women with respect to both stimulation currents and a decrease for sham in men and women at 140% NWR threshold current stimulation. Between-condition differences were meaningful at the rectus femoris with respect to both currents for women but not for men. Within-condition differences between men and women were meaningful for heat pain at the rectus femoris with respect to both currents and for sham at the rectus femoris for 140% threshold current.
3.3.1. MagnitudeTable 4 shows the effect size of condition on NWR-M with respect to recording site and stimulation current, for the full cohort as well as for men and women separately. The effect of heat pain on NWR-M was always statistically meaningful for women with median effect sizes of 0.36 and 0.33 at the biceps femoris as well as 0.31 and 0.36 at the rectus femoris, for 120% and 140% NWR threshold, respectively, and resulting probabilities ≥98.6. This was never the case for men with HDI95 always containing 0 as visible in Figure 3 with median effect sizes 0.12 and 0.20 at the biceps femoris as well as 0.21 and 0.29 for the rectus femoris, for 120% and 140% NWR threshold, respectively. Meaningful effects for the full sample, including the negative effect for sham at 140% NWR threshold stimulation at the biceps femoris (Table 4), merely resulted from pooling the data of men and women. They are thus not further discussed.
Table 4 - Effect size [HDI95] of condition on nociceptive withdrawal reflex magnitude with respect to recording site and stimulation current with calculated probabilities (percent). Heat pain Sham Full sample Men Women Full sample Men Women 120% NWR threshold current stimulation BF [0.04, 0.45] (98.8) [−0.16, 0.39] (81.3) [0.04, 0.69] (98.6) [−0.39, 0.01] (3.3) [−0.40, 0.11] (13.1) [−0.57, 0.10] (7.8) RF [0.05, 0.47] (99.2) [−0.15, 0.57] (87.7) [0.08, 0.55] (99.5) [−0.29, 0.11] (19.0) [−0.41, 0.09] (9.3) [−0.34, 0.31] (46.8) 140% NWR threshold current stimulation BF [0.09, 0.45] (99.8) [−0.05, 0.46] (94.1) [0.06, 0.61] (99.0) [−0.40, −0.01] (2.1) [−0.53, 0.14] (13.7) [−0.45, 0.01] (2.9) RF [0.12, 0.52] (99.9) [−0.05, 0.63] (95.2) [0.13, 0.58] (99.8) [−0.29, 0.1] (15.5) [−0.40, 0.05] (6.6) [−0.35, 0.30] (43.0)Bold HDI95 values indicate a meaningful effect. Values in parentheses represent the probability in percent for the effect >0.
BF, biceps femoris muscle; HDI95, 95% highest density interval for difference of Bayesian posterior distributions; NWR, nociceptive withdrawal reflex; RF, Rectus femoris muscle.
 Figure 3.:
Figure 3.: Bayesian posterior distributions for effect of heat pain condition on nociceptive withdrawal reflex magnitude at the biceps femoris and rectus femoris muscles with 95% highest density intervals (HDI95) and null effect line.
The results of BEST with broad priors are given in Table 5. For men, there were no statistically meaningful differences between the conditions, ie, the respective HDI95 always included 0 (no difference). For women, the differences in effect between the conditions were meaningful at the biceps femoris for both relative stimulation currents. With a probability of 95.6% and 97.2%, respectively, heat pain exerted a greater effect on NWR-M at the biceps femoris than sham corresponding to median differences of 0.60 and 0.55 (men: 0.27 and 0.42). However, the differences between men and women within the same condition were not statistically meaningful (0 ∈ HDI95). The between-condition differences for the full sample were meaningful at the biceps femoris for both relative currents and at the rectus femoris for 140% NWR threshold. But these results were again due to data pooling. To test for a potential predictive influence on the results, heat pain threshold was included as a metric predictor in a hierarchical Bayesian model. This yielded no additional information (data not shown).
Table 5 - Difference in effect [HDI95] on nociceptive withdrawal reflex magnitude between the conditions (heat pain − sham) and within condition (men − women) with respect to recording site and stimulation current with calculated probabilities (percent). Between-conditions difference (heat pain − sham) Within-co
留言 (0)