1. Introduction
The Global Burden of Diseases, Injuries, and Risk Factors Study 2017 found that chronic pain was the leading cause of years lived with disability (YLD) rates across the world.17 Chronic pain is defined as pain lasting for at least 3 months.43 Chronic pain patients often need to give up work, hobbies, sport, and household chores.29 Chronic pain is associated with substantial economic burden due to healthcare resources used, productivity losses, and lower quality of life, including anxiety and depression.19,30,35 Sick-listed employees may find it difficult or impossible to return to the workplace because of the combined challenges of managing their pain and poor environmental support.30,49 Estimates of the prevalence of chronic pain are variable, depending on which definitions and methods are being used, and range from approximately 20% in Australia5 28.4% adults in the United States11 to up to 51.3% adults in the United Kingdom.14
Productivity costs occur when the productivity of individuals is affected by illness, treatment, disability, or premature death.19 Chronic pain management interventions aimed at functional improvements in working age patients have the potential to produce substantial societal gains because of improved productivity. Economic evaluations of an intervention can aid decision makers in the allocation of limited healthcare resources (a healthcare perspective) and help determine the benefit to society as a whole (the societal perspective). The relevance of including productivity loss (costs) or gain (benefits) in these evaluations is increasingly recognized, and therefore, studies quantifying productivity outcomes (costs and/or benefits) are needed.
In Australia, the cost of productivity losses associated with chronic pain was estimated to be AU$48.3 billion in 2018,12 and studies have indicated that older working age people with chronic pain have an increased risk of falling into income poverty.35 In the United States, Gaskin and Richard estimated that the annual cost of lost productivity because of pain (in 2010 dollars) was between US $299 and US $335 billion.16 In Chile, musculoskeletal chronic pain was estimated to cost 0.417% of the national gross domestic product (GDP) with more than US $19 million estimated to be due to productivity losses.48 Some groups of people with chronic pain seem to fare worse than others. For example, patients with chronic neuropathic pain appear generally in poorer health and to have higher costs of health care resource utilization and lower productivity than chronic pain patients with nonneuropathic pain.3,34
Because of the prevalence and generally poor outcomes of treatments for chronic pain, a wide variety of pain management approaches have been developed, along with guidelines for treatment.6 Not surprisingly, these come with a cost. Although several cost-effectiveness studies of chronic pain management interventions have been reported,7,33 a comprehensive review of the productivity outcomes of such interventions has not yet been conducted. As such, the aim of this review was to answer 2 questions:
(1) What productivity measures have been used in economic evaluations completed alongside randomised controlled trials (RCTs) of chronic pain management intervention in the working age population?
(2) What was the effect on productivity outcomes of those interventions?
2. Materials and methods
The systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines.28 The protocol for this study was published previously by these authors.8
2.1. Eligibility criteria
We determined study eligibility using the Population, Intervention, Comparison, Outcome framework27 and summarised as follows:
2.1.1. Study types
English-language economic evaluations (cost-effectiveness and cost-utility studies) of chronic pain management interventions arising from RCTs.
2.1.2. Participants
Working-age adults (18-65 years) experiencing musculoskeletal and/or neuropathic pain.
2.1.3. Interventions
Any nonpharmaceutical and nonsurgical interventions and any control.
2.1.4. Outcomes
Any reported productivity outcomes such as return to work or reduced sick leave.
Studies involving working-age adults with other conditions (such as pain related to pregnancy, cancer) were excluded. Grey literature and conference proceedings were also excluded.
Studies were grouped by type of study (intervention vs usual care and intervention vs alternate intervention) and productivity outcome for synthesis.
2.2. Identification and selection of studies
Four investigators (A.R.C., P.L.G., D.S. and M.N.) determined and used the following search strategy ((chronic) AND ((neck pain) OR (shoulder pain) OR (arm pain) OR (leg pain) OR (back pain) OR (neuropathic pain))) AND ((cost benefit) OR (cost effectiveness) OR (cost utility) OR (economic evaluation)). The electronic databases Econlit, Embase, and Pubmed were searched for relevant studies published from inception to March 2023. Abstracts and titles of the studies identified through the database search were screened independently by 2 investigators (A.R.C. and P.L.G.) to identify full-text English-language RCTs, including productivity outcomes for detailed review. Differences were resolved by consensus. Studies were included if they met the terms of the inclusion criteria.
2.3. Data extraction
Data extraction was performed using a standardized form. A.R.C. extracted study characteristics, including year of publication, country, settings, intervention(s), measures of clinical and healthcare utilization and follow-up and measures of productivity. These extracted data were checked and verified by 2 coauthors (D.S. and D.C.). Differences were resolved by consensus. Cost-effectiveness results were extracted from measures of both effectiveness (efficacy) and economic costs by A.R.C. and D.C. Measures of productivity, including the return to work, human capital approach (HCA), and/or friction cost methods (FCM), were extracted. The HCA measures the future monetary value of lost productivity such as sick leave or absenteeism at paid work because of illness or disability.23 The FCM restricts costs of productivity loss to the friction period—the period it takes to replace a worker because of illness, although internal resource reserves are taking up the work of a missing employee and the duration and the costs of hiring and training new workers taking into account the degree of scarcity of labour in the economy.22,46 Other cost-effectiveness measures extracted for this study were derived from health outcomes, standardized health-related quality of life measures, and measures to evaluate psychological components of chronic pain conditions and disability associated with the conditions.
2.4. Assessment of the health economic evaluation reporting standards and risk of bias
Data for the assessment of the economic evaluation reporting standards were extracted using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 statement. This statement provides decision makers and researchers with guidance and a checklist to improve reporting.20 Key data extracted included the population of interest, perspective, comparators, time horizon, discounting, outcome measures, including efficacy, quality of life, and productivity measures, incremental costs and outcomes, analytical methods supporting the evaluation, measures of uncertainty, reporting style, findings of the study, sources of funding, and conflicts of interest. A.R.C. and D.S. jointly assessed the included studies. P.L.G. resolved disagreements where necessary.
Risk of bias was assessed independently by 2 authors (A.R.C. and P.L.G.) using the revised Cochrane risk of bias tool for randomized trials.40 This tool explicitly assesses the risk of bias associated with the randomization process, deviation from the intended interventions, missing outcomes, measurement of the outcomes, and selection of the reported results. Overall, where studies had one or more domains in which there were some concerns or high concerns about the risk of bias, these studies were categorised as at high risk of bias using the Cochrane tool. Differences were resolved by consensus.
2.5. Effect measures and synthesis
The primary outcome of interest was the difference in productivity measures between intervention arms. Because of anticipated variability in trials designs, interventions applied, cohorts studied, and definitions and methods of collecting productivity measures, a narrative synthesis was planned.
3. Results
3.1. Flow of studies through the review
A total of 896 studies were identified through the initial search. After removing 2 duplicates, 894 titles and abstracts were screened for inclusion. Of these, 140 full-text articles were assessed for eligibility with 12 RCTs included in the narrative synthesis. Figure 1 shows the flow diagram.
;) Figure 1.:
Figure 1.: PRISMA flowchart of the study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
3.2. Characteristics of studies included
The included study characteristics are summarised in Table 1. The included studies were all from Europe and the United Kingdom, 91.7% (11/12) were on low back pain, 1 study was on whiplash or neck disorder,25 and 1 study included patients with unspecific chronic pain.21 Among the included studies, 58.3% (7/12) involved intervention vs usual care and the rest (41.7%) comprised comparison of 2 or more interventions. All studies had similar cohorts in terms of age (working age population) and their chronic pain duration (typical duration >3 months).
Table 1 -
Characteristics of included studies.
Authors, y (additional supporting papers used for data extraction such as study protocols etc)
Setting (outpatient, primary, secondary etc)
Interventions
Target population/sample size
Details of the economic evaluation
Measures of clinical and healthcare utilization and informal care cost outcomes and follow-up
Measures of productivity
Apeldoorn et al. 2012
2 Apeldoorn et al. 2010
1
Primary and secondary care
Intervention 1: treatment according to a classification system (direction-specific exercises, spinal manipulation or stabilization exercises)
Intervention2: usual physical therapy according to Dutch low back pain (LBP) guidelines
Age: 18-65 y
F: 56.95%
Pain type: subacute and chronic low back pain (CLBP)
Pain duration: >6 wk
Total sample size: 156
Country: Netherlands
Currency: Euro
Time horizon: 1 year
Perspective: societal
Type of economic evaluation: CEA and CUA
Reference year: 2009
Discounting: not applied as 1 y time horizon
Health outcome measure:
Global perceived effect measured by self-assessed 7 points Likert scale
Pain intensity using an 11-point numerical rating scale (NRS)
Health-related quality of life using EQ-5D
Quality-adjusted life years (QALYs) measured by multiplying utility of a health state by the time spent in this health state
Cost measures:
Direct cost:
Healthcare utilization (HCU) cost:
Primary care cost
Secondary care cost
Nonhealthcare cost:
Informal care (per hour)
Paid home help (per hour)
Follow-up: 8, 26,39, and 52 wk
Reported as Indirect cost:
Cost of absenteeism by mean productivity cost (GBP) per hour using Friction Cost Method (FCM) and Disease Questionnaire (PRODISQ) (sensitivity analysis was conducted using human capital approach (HCA))
Chuang et al. 2012
9Cox et al. 2010
10
Primary and secondary care
Intervention 1: yoga+ usual care
Intervention 2: usual care (any ongoing treatment)
Age: 18-65 y
F:N/A
Pain type: CLBP
Pain duration: 18 mo
Total sample size: 313
Country: UK
Currency: GBP
Time horizon: 1 y
Perspective: National Health Services (NHS) and Societal
Type of economic evaluation: CEA and CUA
Reference year: 2008-2009
Discounting: N/A
Health outcome measure:
Roland–Morris disability questionnaire (RMDQ) to measure back function
EQ-5D to measure QALYs
HCU:
Primary care cost
Secondary care cost
Private care cost
Nonhealthcare cost:
Equipment purchase cost
Follow-up: 3, 6, and 12 mo
Reported as Other costs:
Cost of absenteeism by number of days off work in terms of GBP (national income per day)
Goossens et al. 2015
18Leeuw et al. 2008
26
Multicentre (Hospital) settings
Intervention 1: exposure in vivo (EXP) (CBT, educational sessions)
Intervention2: graded activity—CBT one session
Age: 18-65 y
F: 50%
Pain type: LBP
Pain duration: ≥3 mo
Total sample size:62
Country: Netherlands
Currency: Euro
Time horizon: 15 mo
Perspective:
type of economic evaluation:
Reference year: 2014
Discounting: N/A
Health outcome measure:
36-item Short-Form Health Survey (SF-36)
Quebec back pain disability scale
Cost measures:
Healthcare costs
Intervention cost
Patient and family costs
Productivity loss
Follow-up: 6,12 mo
Cost of absenteeism was measured by the number of days off for back pain multiplied by cost per day using HCA
Also estimated using the FCM in a sensitivity analysis
Kemani et al. 2015
21
Hospital services
Intervention 1: acceptance and commitment therapy
Intervention2: applied relaxation
Age: 18-65 y
F:73%
Pain type: chronic unspecific pain
Pain duration: ≥6 mo
Total sample size:60
Country: Sweden
Currency: USD
Time horizon: 6 mo
Perspective: societal
Type of economic evaluation: CEA
Reference year: 2013
Discounting: N/A
Health outcome measure:
The Pain Disability Index (PDI) (0-10 scale)to assess the disabling effects of chronic pain on daily activities
The Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety and depression
Acceptance of pain using the Chronic Pain Acceptance Questionnaire (CPAQ)
Short Form-12 health survey (SF-12) to assess health-related quality of life
Cost measures:
direct healthcare utilization cost
Direct nonmedical cost
Productivity loss
Follow-up: posttreatment, 3 and 6 mo
Productivity losses were estimated using the HCA, ie, monetary losses associated with work loss and work cutback were based on the average gross earning in Sweden for the duration of the reported number of days off
Lambeek et al. 2010
24
Primary and secondary care
Intervention 1: integrated care
Intervention2: usual care with advice (following the Dutch physiotherapy guideline)
Age:18-65 y
F: 63%
Pain type: CLBP
Pain duration:>3 mo
Total sample size: 134
Country: Netherlands
Currency:
Time horizon:
Perspective: societal
Type of economic evaluation: CBA,CEA,CUA
Reference year: 2007
Discounting: N/A
Health outcome measure:
Duration until sustainable return to work
QALYs using the Euro- Qol
Cost measures:
Direct healthcare cost
Nondirect healthcare cost
Productivity loss
Follow-up: 12 mo
HCA to calculate the costs of productivity loss as a result of days off (work hours multiplied by per hour cost of productivity loss)
Landén Ludvigsson et al. 2017
25
Multicentre
Intervention 1: physiotherapist-led neck-specific exercise (NSE)
Intervention2: NSE with a behavioural approach (NSEB)
Intervention 3: prescription of physical activity
Age: 18-63 y
F:65%
Pain type: chronic whiplash-associated disorders (WAD)
Pain duration: 6-36 mo
Total sample size:216
Country: Sweden
Currency: USD
Time horizon: 12 mo
Perspective: societal
Type of economic evaluation: CUA
Reference year: 2016
Discounting: N/A
Health outcome measure:
The neck disability index (NDI)
EQ-5D
SF-6D
Cost measures:
Healthcare utilization cost
Intervention cost
Productivity loss
Follow-up: 3, 6, and 12 mo
Productivity loss was calculated using the HCA including gross salary plus taxes
Niemisto et al. 2005
31
Intervention 1: manipulative-treatment group
Intervention2: physician's consultation group
Age: 24-48 y
F: 55%
Pain type: CLBP
Pain duration:>3 mo
Total sample size: 204
Country: Finland
Currency: USD
Time horizon: 12 mo
Perspective: societal
Type of economic evaluation: CEA
Reference year: 2002
Discounting: N/A
Health outcome measure:
A visual analogue scale (VAS; from 0 to 100)
The Oswestry Low Back Pain Disability Questionnaire (ODI; from 0 to 100)
Health-related quality of life (HRQoL) (15D)
Cost measures:
Health care utilization cost
Productivity loss
Follow-up: 5 and 12 mo; 2 y
Productivity costs because of absence from work. Productivity costs were estimated by the average 2000-y wage level in Finland
Schweikert et al. 2006
36
Intervention 1: usual care + cognitive behavioural pain management program
Intervention2: usual care (including physiotherapy, massage, seminars, and exercise)
Age: ≥18 y
F:17.2%
Pain type: CLBP
Pain duration: >6 mo
Total sample size:409
Country: Germany
Currency: Euro
Time horizon: 6 mo
Perspective: societal
Type of economic evaluation: CEA, CUA
Reference year: 2001
Discounting: N/A
Health outcome measure:
VAS
Euro-QoL
Cost measures:
Healthcare utilization cost
Nonmedical cost
Productivity loss
Follow-up: 1 and 6 mo
Productivity costs were estimated by age- and sex-adjusted average labor costs incorporating salaries and social insurance premiums paid by employers and employees because of days off at work
Smeets et al. 2009
39
Outpatient rehabilitation centres
Intervention 1: active physical training (APT)
Intervention 2: behavioural therapy (GAP)
Intervention 3: APT + GAP (combined training)
Age:18-65 y
F: 45%
Pain type: LBP
Pain duration: ≥3 mo
Total sample size: 160
Country: Netherlands
Currency: Euro
Time horizon: 12 mo
Perspective: societal
Type of economic evaluation: CEA, CUA
Reference year: 2003
Discounting: N/A
Health outcome measure:
RMDQ
Euro-QoL
Cost measures:
Direct healthcare cost
Nondirect healthcare cost
Productivity loss
Follow-up: 6, 12 mo
Absenteeism from paid work was calculated according to the HCA
Thomas et al. 2005
42
Primary and secondary care
Intervention 1: acupuncture
Intervention2: usual care (pragmatic GP management, with no restrictions on the care they received)
Age:18–65 y
F:60.2%
Pain type: nonspecific LBP
Pain duration: 4–52 wk
Total sample size: 241
Country: UK
Currency: GBP
Time horizon: 24 mo
Perspective: societal
Type of economic evaluation: CEA and CUA
Reference year: FY:2001-02
Discounting: 3.5%
Health outcome measure:
Short form 36 (SF-36) bodily pain dimension (range 0-100 points)
EuroQoL 5 dimensions (EQ-5D)
McGill present pain index (PPI)
Oswestry Pain Disability Index (ODI)
Cost measures:
Healthcare utilization cost
Productivity loss
Follow-up: 3, 12, and 24 mo
Employment status and time lost from work because of lower back pain in terms of GBP using age- and gender-adjusted daily wage
Van der Roer 2008
47
Primary care
Intervention 1: intensive group training protocol
Intervention2: usual care (physiotherapy)
Age:18-65 y
F:N/R
Pain type: Non-specific CLBP
Pain duration: >12 wk
Total sample size: 114
Country: Netherlands
Currency: Euro
Time horizon: 12 mo
Perspective: societal
Type of economic evaluation: CEA, CUA
Reference year: 2004
Discounting: N/A
Health outcome measure:
RMDQ
Pain intensity measure
General perceived effects measure scale
Euro-QoL-5D
Cost measures:
Direct healthcare utilization cost
Indirect healthcare utilization cost
Productivity loss
Follow-up: 6, 13, 26, and 52 wk
Absenteeism from paid work using HCA
Werner et al. 2016
52
Primary settings
Intervention 1: cognitive-based education program (CBEP)
Intervention2: usual care (provided by general practitioners [GP] and physiotherapists [PT])
Age: 20-55 y
F: 58.5%
Pain type: unspecific LBP
Pain duration: 4-12 mo
Total sample size:216
Country: Norway
Currency: USD
Time horizon: 12 mo
Perspective: societal
Type of economic evaluation: CEA,CUA
Reference year: 2012
Discounting: N/A
Health outcome measure:
RMDQ
EQ-5D
Cost measures:
Healthcare utilization cost
Productivity loss
Follow-up: 4 wk, 3, 4, 6, and 12 mo
Absenteeism costs were estimated by multiplying the number of days absent from work by the average wage rate
It was necessary to consult other publications1,10,26 on these studies to determine some of the information.
3.2.1. Health outcome measures
The included studies used various health outcome measures, including numerical or Likert rating scales for pain intensity (4 studies)2,31,36,47 or pain index questionnaires (1 study42) and functional status (9 studies)9,18,21,24,25,36,42,47,52 and measures of anxiety and depression (1 study21) and pain acceptance (1 study21).
3.2.2. Quality-adjusted life years
Quality-adjusted life years (QALYs) were measured by all studies. One study measured QALYs by multiplying utility of a health state by the time spent in this health state,18 9 studies evaluated health-related quality of life using the EQ-5D,1,9,24,25,32,36,39,42,47,52 36-item Short-Form Health Survey (SF-36)50 (2 studies),18,42 Short Form-12 Health Survey (SF-12)51 (1 study),21 SF-6D (2 studies),25,53 and health-related quality of life (HRQoL) (15D)38 (1 study).18
3.2.3. Economic evaluation
All 12 included studies measured costs from a societal perspective. The study of Chuang et al. also measured costs from a healthcare perspective.9 Cost-effectiveness of the intervention of interest was established in 6 studies.9,18,24,25,31,36 The study conducted by Kemani et al.21 established cost-effectiveness of the intervention at posttreatment and in 3 months but not at 6 months; however, differences in costs and outcomes were not statistically significant except for the differences in the productivity outcome.
3.2.4. Productivity outcome
All of the included studies calculated and reported productivity loss using absenteeism from paid work translating return to work measures into indirect costs (cost savings) in monetary terms (indicated by an amount of money such as UK pound sterling, Euro etc). All but 1 study2 used the HCA to calculate absenteeism from paid work with the study by Goossens et al.18 and also conducting a sensitivity analysis by applying the FCM. The remaining study, Apeldoorn et al.,2 calculated the cost of absenteeism using the FCM and conducted a sensitivity analysis by applying the HCA. The study of Lambeek et al.24 was the only one to capture productivity gain by including return to work as their primary outcome.
3.3. Assessment of the health economic evaluation reporting standards
Results of the CHEERS assessment, presented in Figure 2, shows the proportion of RCTs for which a yes (Y), not reported (N), or not applicable (NA) response was obtained for each CHEERS checklist item. All studies addressed items 1 to 3, 5 to 9, 11 to 15, 19, 20, 23, 26, and 27 (the list of items and detailed interpretations is shown in Husereau et al).20 None of the studies used modelling (items 16) or engaged with noninvestigator stakeholders (items 21 and 25) and only 1 study (8%)42 used discounting (item 10). Only 2 studies2,9 validated data for statistical analysis (item 17), and 4 studies2,9,31,42 described subgroup results (item 18). In 2 studies, conflicts of interest did not appear to be reported36,39 (item 28) and in 5 studies,21,25,36,39,42 separate publication of a health economic analysis plan was not reported (item 4). The results implied reasonable methodological quality overall.
Figure 2.: Proportion of yes, no (not reported), and not applicable responses to each Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist item by the 12 included studies. Responses to each checklist item was recorded as N/A, not applicable; N, not reported; Y, reported.
3.4. Risk of bias
Responses to the risk of bias assessment were similar across all included studies (Fig. 3). Most studies were considered to have a “low risk of bias” for most domains; 91.7% of studies had low risk of bias for “randomisation process” and “deviations from intended interventions,” 66.7% for “missing outcome data,” and 50% for “selection of the reported result.” For the domain “measurement of the outcome,” most studies were deemed to have a high risk of bias (91.7%) as outcomes were self-reported. All but 2 studies2,52 were assessed to have a high risk of bias with this overall result arising from having one or more domains considered high risk.
Figure 3.: Cochrane Risk of Bias (RoB 2 tool) summary.
3.5. Summary of productivity outcomes of chronic pain management and cost-effectiveness of the included studies from chronic pain management interventions
Summaries of the productivity and other cost-effectiveness outcomes for each study are shown in Table 2.
Table 2 -
Results of included studies.
Studies
Costs, mean (SD)
Mean difference (95% CI) (Societal perspective)
Costs of productivity, mean (SD)
Mean difference (95% CI)
Effects, mean (SD)
Mean difference (95% CI)
Reported ICER
Author's conclusion: cost-effective?
Mean (SD) number of sick leave at follow-up
Apeldoorn et al. 2012
2Apeldoorn et al. 2010
1
Intervention 1: €2287 (482)
Intervention 2: €2020 (331)
Mean difference (95% CI) = €266 (−720; 1612)
Intervention 1: €1575 (378)
Intervention 2: € 1208 (289)
Mean difference (95% CI) = €367 (−423, 1545)
Intervention 1:
GPE = 0.68 (0.06)
ODI improvement = −8.2 (1.7)
NRS improvement = −2.83 (0.40)
QALYs gained = 0.82 (0.02)
Intervention 2:
GPE = 0.47 (0.06)
ODI improvement = −7.8 (1.7)
NRS improvement = −2.69 (0.35)
QALYs gained = 0.80 (0.02)
Mean (SD) difference (Int 1 − Int 2):
GPE = 0.20 (0.04, 0.37)
ODI improvement = 0.5 (−4.4, 5.4)
NRS improvement = 0.13 (−0.86, 1.12)
QALYs gained = 0.02 (−0.03, 0.08)
ICER based on GPE = €1299
ICUR based on QALYs = €10,543 cost per QALYs gained
Intervention 1 not cost-effective compared with Intervention 2 (Outcome and cost differences were not statistically significant) Authors do not recommend widespread approach
Intervention 1: 12.6 d (30.4)
Intervention 2: 14.0 d (47.2)
Chuang et al. 2012
9Cox et al. 2010
10
Intervention 1: £1502.1 (2550.4)
Intervention 2: £2319.2 (3188.1)
Mean difference (95% CI) = −£ 667.48 (−1492.9 to 157.9)
Intervention 1: £374.2 (1142.5)
Intervention 2: £ 1201.8 (2550)
Mean difference = −£827.6
Intervention 1:
QALYs gained = 0.778 (0.143)
Intervention 2:
QALYs gained = 0.725 (0.172)
Mean difference (95% CI):
QALYs gained = 0.054 (0.021-0.088)
NHS perspective, ICUR based on QALYs = £13,606 cost per QALYs gained
Societal perspective, ICUR based on QALYs = £20,000 cost per QALYs gained
Intervention 1 was cost-effective compared with intervention 2. Cost of productivity lost = 1201.8 (UC) vs 374.2 (yoga)
Intervention 1: 3.83 d (SD: 11.68)
Intervention 2: 12.29 d (SD: 26.07)
Goossens et al. 2015
18Leeuw et al. 2008
26
Intervention 1: €13,477.71 (2450.28)
Intervention2: €10,843.50 (1747.89)
Mean difference (95% CI): −€2643 (−8535 to 3058)
Intervention 1: €1126.98 (355.07)
Intervention2: €754.83 (255.86)
Mean difference (95% CI): €372.15 (−4987 to 1908)
Intervention 1:
QPBDS: 40.42 (22.34)
SF36:0.68 (0.14)
QALY:0.82 (0.12)
Intervention 2:
QPBDS:38.19 (20.84)
SF36:0.66 (0.14)
QALY:0.83 (0.13)
Mean difference (95% CI):
QPBDS: −2.23 (−13.20 to 8.75)
SF36: −0.15 (−0.08 to 0.05)
QALY: 0.01 (−0.6 to 0.07)
Based on QPBDS, €16,000 for an additional improvement in QPBDS
Based on QALYs, 0.01 for an additional QALY
Intervention 2 cost-effective compared with intervention 1 but differences were not significant
Intervention 1: 191.39 h (SD 362.60 h)
Intervention2: 291.69 h (SD 501.99 h)
Kemani et al. 2015
21
Intervention 1: $7836 (5676)
Intervention 2: $5694 (4713)
Intervention 1: $5406 (4258)
Intervention 2: $3664 (3650)
6-mo follow-up:
Intervention 1:
PDI: 31.2 (19.0)
Pain:4.4 (1.3)
SF12M:39.3 (10.8)
SF12P:39.3 (10.2)
HADS-a:9.1 (5.1)
HADS-d:8.4 (5.6)
CPAQ: 63.4 (21.2)
Intervention2:
PDI: 34.0 (16.2)
Pain: 4.1 (1.5)
SF12M: 38.8 (13.8)
SF12P: 32.3 (9.8)
HADS-a: 9.2 (5.1)
HADS-d: 8.4 (5.5)
CPAQ: 50.2 (21.9)
At 3 mo follow-up: −648, indicating that each incremental improvement on the PDI for participants
in ACT relative to AR generated a societal earning of $648
Intervention 1 was more cost-effective compared with Intervention 2 at 3-mo follow-up but not at 6-mo follow-up. Differences in indirect costs were significant (as determined by sign tests)
Intervention 1: 67 h (SD 246 h)
Intervention2: applied relaxation (AR)= 1002 h (SD 2081 h)
Lambeek et al. 2010
24
Intervention 1: £13,165 (SD £13,600)
Intervention 2: £18,475 (SD £13,616)
Mean difference (95% CI): −£5310 (−10,042 to −391)
Intervention 1: £11,686 (SD £12,553)
Intervention2: £17,213 (SD £13,416)
Mean difference (95% CI): −£5527 (−10160 to −740)
Intervention 1:
Days until sustainable return to work: 129 (117)
QALYs: 0.74 (0.19)
Intervention 2:
Days until sustainable return to work: 197 (129)
QALYs: 0.65 (0.21)
Mean difference (95% CI):
Days until sustainable return to work: −68 (−110 to −26)
QALYs: 0.09 (0.01-0.16)
Days until sustainable return to work: £ −3
QALYs: £A61,000 cost per QALYs gained
Intervention 1 would significantly reduce societal costs, increase effectiveness of care, improve quality of life, and improve function on a broad scale compared with intervention 2
Intervention 1: 88.5 number of net days (SD 95.5 number of net days)
Intervention2: 130.4 number of net days (SD 102.7 number of net days)
Mean difference of net sick leave at 12 mo follow-up −68 d
Landén Ludvigsson et al. 2017
25
Intervention 1: $2976 (SD $7650)
Intervention2: $6810 (SD $13,453)
Intervention 3: $5.349 (SD $10,429)
Intervention 1: $2154 (SD $6963)
Intervention2: $5556 (SD $13,058)
Intervention 3: $4147 (SD $10,003)
Intervention 1:
Utility change score
EQ-5D: 0.046 (0.208)
NDI: 0.040 (0.10)
SF-6D: 0.054 (0.113)
QALY gained
EQ-5D: 0.023 (0.103)
NDI: 0.020 (0.050)
SF-6D: 0.027 (0.056)
Intervention 2
Utility change score
EQ-5D: 0.106 (0.252)
NDI: 0.055 (0.086)
SF-6D: 0.028 (0.106)
QALY gained
EQ-5D: 0.053 (0.126)
NDI: 0.028 (0.043)
SF-6D: 0.014 (0.053)
Intervention 3:
Utility change score
EQ-5D: −0.038 (0.282)
NDI: −0.006 (0.080)
SF-6D: 0.002 (0.112)
QALY gained
EQ-5D: −0.019 (0.141)
NDI: −0.003 (0.040)
SF-6D: 0.001 (0.060)
Intervention 1 vs 2:
Societal perspective: EQ5D: 127,800 (95% CI: 37,816-711,302)
NDI: 14,400 (5039-74,484)
Healthcare perspective:
EQ5D: $479,250 (49,160-2,951,905)
NDI: $54,000 (6550-309,197)
Intervention 1 was cost-effective compared with intervention 2 and 3
Intervention 1: 13.8 d (SD 43.7 d)
Intervention2: 29.7 d (SD 74.9 d)
Intervention 3: 21.6 d (SD 46.5 d)
Niemisto et al. 2005
31
Intervention 1:$2262 (SD $3156)
Intervention 2: $2280 (SD $5294)
Mean difference =-$18
Intervention 1: $1632 (SD $2728)
Intervention 2: $1970 (SD $5068)
Mean difference = −$338
Intervention 1:
VAS: 30.7 (24.4)
The Oswestry Low Back Pain Disability Questionnaire = 12.0 (11.6)
HRQoL(15D) = 0.91 (0.078)
Intervention 2: VAS: 33.1 (24.9)
The Oswestry Low Back Pain Disability Questionnaire = 14.0 (9.9)
HRQoL(15D) = 0.91 (0.082)
Intervention 1 vs Intervention 2: VAS: $512 (15,714)
The Oswestry Low Back Pain Disability Questionnaire = $78 (20,818)
Intervention 2 was cost-effective than intervention 1. Productivity costs were lower in the physician's consultation group compared with the manipulative treatment group
Intervention 1: 12.3 d (SD 20.5 d)
Intervention2: 14.8 d (SD 38.0 d)
Schweikert et al. 2006
36
Intervention 1: €8849.3 (SD €5820.0)
Intervention 2: $10,519.9 (SD €8073.6)
Mean difference: –$1670.6 (P-value for the diff −0.054)
Intervention 1: €1441.1 (SD €3713.4)
Intervention 2: €2192.1 (SD €4622.9)
Mean difference: −€751
Incremental effects:
Intervention 1:
∆ admission − discharge:
EuroQoL: 9.6 (18.3)
Functional capacity: 2.8 (12.3)
Depression: −2.3 (4.7)
Anxiety: −2.7 (6.9)
Subjective back pain: −1.2 (1.2)
∆ 6-mo follow-up–discharge:
EuroQoL: −2.4 (17.8)
Intervention 2:
∆ Admission–discharge:
EuroQoL: 9.3 (15.2)
Functional capacity: 3.5 (13.4)
Depression: −1.6(4.2)
Anxiety: −2.3 (6.3)
Subjective back pain: −1.2 (1.2)
∆ 6-mo follow-up–discharge
EuroQoL: −4.5 (14.9)
–€126,731 cost per QALY gained
Intervention 1 may be more cost saving than intervention 2
Intervention 1: 11.4 d (SD 28.9 d)
Intervention2: 16.8 d (SD 34.1 d)
Smeets et al. 2009
39
Intervention 1: €20,015 (SD €19,675)
Intervention 2: €14,794 (SD €17,209)
Intervention 3: 19,559 (SD €14,708)
Mean difference (95% CI): (3 vs 1): −€407 (−6987 to 5900)
Mean difference (95% CI): (3 vs 2): −€4787 (984-10,540)
Intervention 1: €16,153 (SD €18,748)
Intervention 2: €11,816 (SD €15,804)
Intervention 3: €14,987 (SD €1562)
Mean difference (3 vs 1): −€1166
Mean difference (3 vs 2): €3171
RDQ
Mean difference (3 vs 1): −1.23 (−3.01 to 0.55)
Mean difference (3 vs 2): −1.27 (−2.96 to 0.42)
QALY:
Mean difference (3 vs 1): −0.014 (0.094-0.066)
Mean difference (3 vs 2): −0.045 (−0.119 to 0.029)
RDQ:
Intervention 3 vs 1: APT 371
Intervention 3 vs 2: GAP −3759
QALY:
Intervention 3 vs 1: APT 35,060
Intervention 3 vs 2: GAP −108,857
Intervention 3 was not more cost-effective than intervention 1 or 2
Intervention 1: 906.94 h (SD 1052.64 h)
Intervention 2: 663.44 h (SD 887.35 h)
Intervention 3: 841.50 h (SD 922.84 h)
Thomas et al. 2005
42
Intervention 1: £2135.39 (£3798.45)
Intervention 2: £2469.09 (£3618.97)
Mean difference (95% CI): –e333.70 (–31601.92 to £1179.81)
Intervention 1: £1679.99 (£4812.54)
Intervention 2: £2321.68 (£6011.38)
Mean difference (95% CI): –e641.69 (–42130.62 to £1299.52)
AUC using SF6D: Mean difference (95% CI): 0.027 (−0.056, 0.110)
£4241 (95% CI: £191 to £28,026)
Intervention 1 was significantly more effective with a higher cost (difference in societal costs were not statistically significant)
Intervention 1: 16.086 total days (0-24 mo) (SD 43.271 d)
Intervention 2: Usual care = 20.13 total days (0-24 mo) (SD 53.739 d)
Van der Roer et al. 2008
47
Intervention 1: €3891 (SD €7011)
Intervention 2: €3658 (SD €5970)
Mean difference (95% CI): €233 (185-2764)
Intervention 1: € 2770 (SD €6643)
Intervention 2: €2838 (SD €5814)
Mean difference (95% CI): −€68 (−2504 to 2302)
Mean difference (95% CI):
Functional status (RDQ): 0.06 (−2.22 to 2.34)
Pain intensity (PI-NRS): −1.02 (−2.14 to 0.09)
Perceived recovery (GPE): 13%
OR 1.71 (0.67-4.38)
QALYNL (EQ-5D): 0.03 (−0.06-0.12)
Functional status (RDQ): 16,349
Pain intensity (PI-NRS): −175
Perceived recovery (GPE): 1720
QALYNL (EQ-5D): 5141
No differences between the interventions

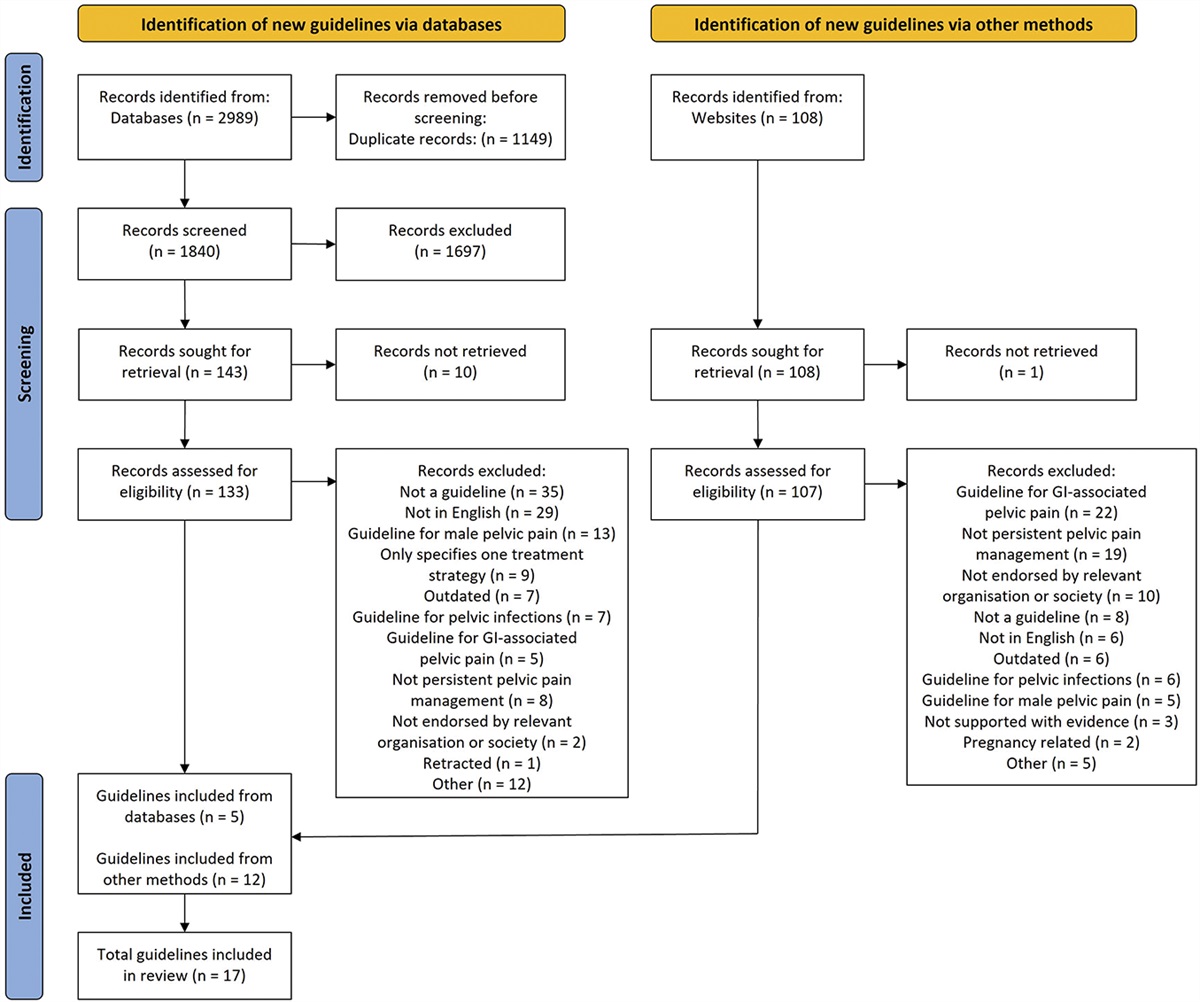


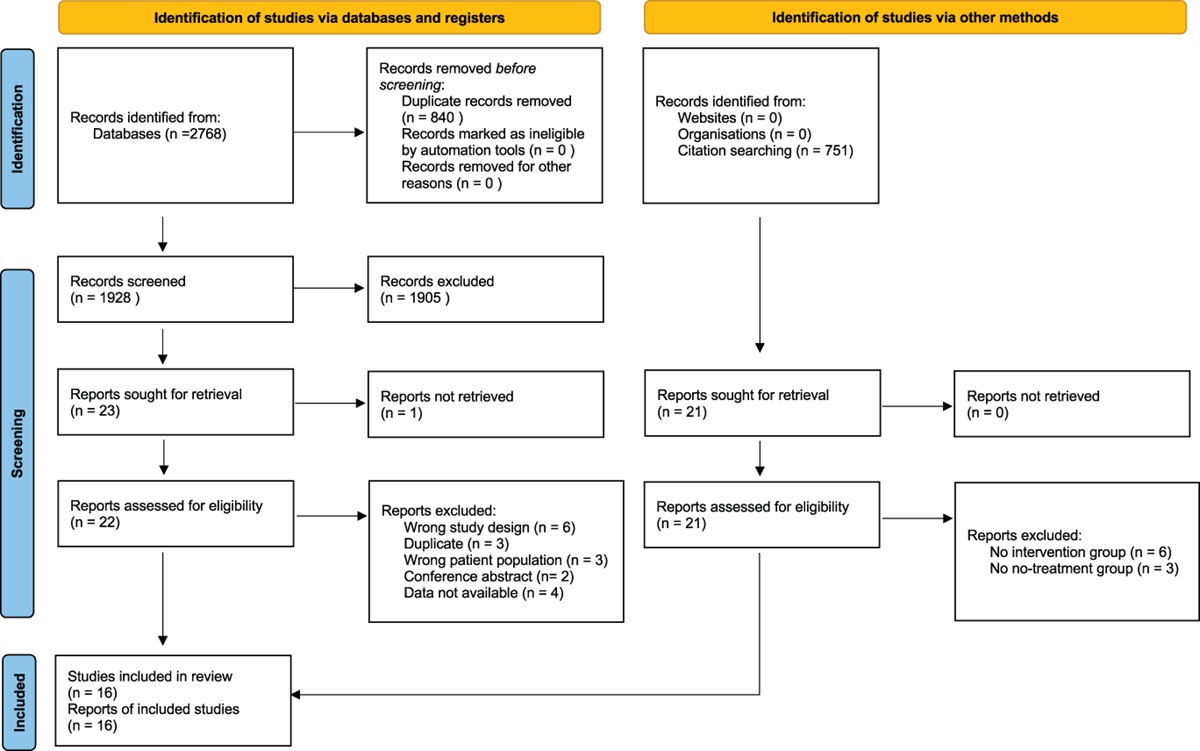
 Figure 1.:
Figure 1.:  Figure 2.:
Figure 2.:  Figure 3.:
Figure 3.:
留言 (0)