
記住我


Opioid and nonopioid analgesics are commonly prescribed to young individuals to alleviate pain in outpatient settings.17,18,74 Receiving prescription analgesics implies seeking help for pain management, indicating the severity of the pain condition.27 Even short-term prescriptions increase the risk of persistent use and future misuse of potent analgesics, such as opioids,1,35,36 and they should therefore be prescribed with great caution in all settings.23,44 Overall, more frequent use of both opioid and nonopioid analgesics is linked to female sex, low socioeconomic status, pain in multiple sites, and psychological distress,8,13,54,62,68,69 with prescriptions increasing sharply from midadolescence.69 Although evidence is sparse, retrospectively assessed childhood interpersonal trauma, including sexual abuse, emotional abuse, and exposure to physical violence, has been found to be associated with using more analgesics.6,29,64 Recent results from a large, prospective study on the relation of childhood trauma to subsequent use of over-the-counter analgesics are consistent with these findings, with results indicating an increased risk of frequent use of over-the-counter analgesics among young adults exposed to childhood trauma.9 Trauma types representing interpersonal violence, such as bullying, sexual abuse, and physical violence, and particularly multiple types of such trauma, have been found to be especially strongly associated with frequent use of over-the-counter analgesics.8 Such cumulative load may be of importance for the relation to analgesics use also for other trauma types.8 Childhood trauma is associated with pain, often in combination with functional impairment as well as psychological distress, with the latter representing an independent risk factor for chronic pain.3,5,15,72 Exposure to childhood trauma may therefore result in an increased risk of receiving prescription analgesics, including opioids.
There is a dearth of prospective studies on the relation of childhood trauma to prescription rates for analgesics in adolescence and young adulthood. Knowledge about the potential importance of childhood trauma exposure as a risk factor for receiving prescription analgesics may inform clinical approaches to pain management for this especially vulnerable group.
In this study, we aimed to investigate the relation of a broad range of childhood trauma exposures to risk of receiving prescriptions for opioid and nonopioid analgesics in adolescence and young adulthood. We further explored whether exposure to multiple trauma types would predict an especially high prescription rate.
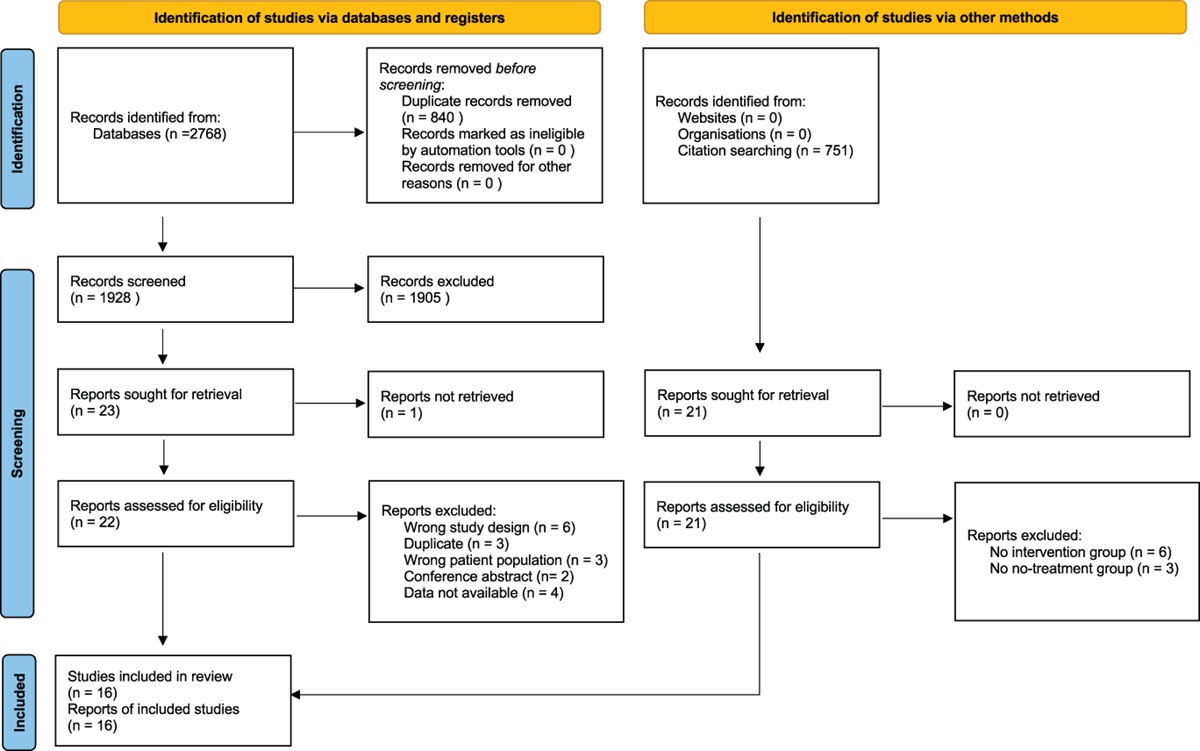
2. Methods 2.1. Data sourcesThis large, prospective cohort study used self-reported data on childhood trauma exposures from adolescents (aged 13-19 years) who participated in the Young-HUNT3 Study (2006-2008)39 linked to data from the Norwegian Prescription Database (NorPD).28 The linkage enabled tracking of individual prescriptions for opioid and nonopioid analgesics for the participants from 2004 to 2021. The Norwegian Institute of Public Health linked the data from the Young-HUNT3 and NorPD based on the unique personal identification number of each individual, ensuring high linkage quality.37 Prescription data were linked for all 8199 participants, including participants who did not receive analgesics prescriptions within the follow-up period. The study was approved by the Norwegian Regional Committee for Medical Research Ethics (project ID: 2017/2229).
In Young-HUNT3, all 10,464 adolescents in the region of Norway formerly called Nord-Trøndelag were invited to participate. The participation rate in Young-HUNT3 was 78% (n = 8199). Inclusion was based on written consent from participants aged 16 years or older and from the parents of those younger than 16 years, in accordance with Norwegian law. The consent to linkage of survey data to registry data was an integrated part of the consent to participate in the HUNT Study because data from the HUNT Study are extensively used in linkage studies. Participants can withdraw their consent at any time. Individuals who withdraw consent to linkage are considered nonparticipants, and they are not included in participant counts. Most adolescents completed the self-administered questionnaire during school hours.
Norwegian prescription database is an electronic registry which has obtained data on all filled prescriptions from all pharmacies in Norway since 2004.28 Each filled prescription is registered with patient identifiers and drug information, including the date of dispensing and an Anatomical Therapeutic Chemical (ATC) code identifying the specific drug.77 All prescriptions filled at a pharmacy, whether issued in primary or specialist care, including hospitals and institutions, are registered. Medications directly dispensed from an institution's medication inventory are not registered.
2.2. Norwegian health services and prescription subsidy programResidents of Norway are automatically enrolled in the public health care system, covering both primary and specialist care.66 Specialist care, including hospital care, requires a referral, while primary care services do not. The costs of health services are subsidized by the government and maintained at an affordable rate.
Prescription medications are paid for by the recipient. Analgesics can be obtained on a reimbursed prescription for chronic pain, where the cost of medication is reduced to 39% of the total cost. To qualify, the patient must have chronic, severe pain that significantly reduces quality of life and function. Validated tools must be used to assess diagnosis, pain severity, and treatment effect. Only 2% of the entire Norwegian population received an analgesic to treat chronic pain on a reimbursed prescription in 2010, corresponding to approximately 10% of those with a diagnosis of chronic pain at the time.57
There is a cost limit for all payments within the public health care system, including payment for consultations and reimbursed prescriptions. Once this limit is reached, further consultations and reimbursed prescriptions are free of charge. Individuals living in a low-income household can apply for reimbursement of health costs regardless of total health expenses. For individuals younger than 16 years, medication on a reimbursed prescription will be dispensed for free, irrespective of total health expenses.
While prescription medication has a fixed maximum price, the pricing of nonprescription medication is not regulated in Norway. Nonsteroid anti-inflammatory drugs (NSAIDs) and paracetamol can be purchased over the counter; however, acquiring them through a prescription can be more affordable.
2.3. Measures 2.3.1. Sociodemographics in adolescenceData on sex and age at the time of attendance in the Young-HUNT3 Study were obtained from the Norwegian National Population Registry. Pubertal development was assessed using a four-item version of the pubertal development scale by Carskadon and Acebo14. Participants were asked 2 questions regarding household structure, and they were categorized as “living with both parents” or “living in other type of household” for the variable Household structure. The adolescents were asked whether they perceived their family economy as below average, average, or above average and were grouped into “family economy average or better” and “family economy below average” for the variable Family economy.
2.3.2. Childhood trauma 2.3.2.1. Lifetime trauma screenChildhood exposure to potentially traumatic events, termed childhood trauma, was assessed in adolescence by a lifetime trauma screen derived from the University of California, Los Angeles Posttraumatic Stress Disorder Reaction Index (UCLA PTSD Reaction Index), part I,70,71 adapted to a Norwegian context. All events were listed under the question “Did you ever experience any of these events?” Response alternatives were “never,” “yes, last year,” and “yes, in my life” for all items. Participants responding “yes, last year” and “yes, in my life” were labelled as exposed.
2.3.2.2. Direct interpersonal traumaItems on exposure to direct interpersonal trauma included physical violence, bullying, and sexual abuse. Participants were classified as exposed to physical violence if they responded affirmatively to the statement “been subjected to violence (beaten/injured)”. Participants who answered “yes” to the statement “been threatened or physically harassed by fellow students at school over a period of time” were classified as exposed to bullying. Exposure to sexual abuse was measured by 2 items: “subjected to an unpleasant sexual act by a peer” and “subjected to an unpleasant sexual act by an adult.” Reports of exposure to either or both were categorized as sexual abuse. A sum score (range 0-3) of the 3 items assessing exposure to different types of direct interpersonal trauma was computed and labelled Interpersonal trauma, number of types. For regression analyses, scores of 2 and 3 were combined because of low counts.
2.3.2.3. Other traumaParticipants were asked whether they had “seen someone else being subjected to violence,” and responders answering affirmatively were classified as having been a witness to violence. Responders answering “yes” to either “someone in your family was seriously ill” or “the death of someone close to you” was classified as exposed to severe illness or death of someone close. Participants responding “yes” to experiencing “a disaster (fire, hurricane or similar)”, “a serious accident (eg, serious car accident),” “painful or frightening hospital treatment for a disease or an accident,” or “other experience that was very frightening, dangerous or violent” were classified as exposed to other potentially traumatic event. A sum score (range 0-3) of the 3 items assessing exposure to different types of other trauma was computed and labelled other trauma, number of types.
2.3.3. Chronic pain and psychological symptoms in adolescencePost-traumatic stress symptoms, psychological distress, headaches, and musculoskeletal pain were assessed in Young-HUNT3; these measures are detailed in Supplementary Table 1 (available at https://links.lww.com/PAIN/B975).
2.3.4. Opioid and nonopioid prescription analgesicsCounts of all prescriptions of opioid analgesics (ATC group N02A) and the nonopioid analgesics paracetamol (ATC group N02BE), gabapentinoids (N03AX12 and N03AX16), and NSAIDs (nonsteroid anti-inflammatory drugs, ATC group M01A) filled by the participants as (1) adolescents and (2) young adults in the period 2004 to 2021 served as outcome measures. The number of filled prescriptions within each analgesic group was counted for each individual. Prescriptions in adolescence (age 13-19 years) and in young adulthood (age 20-32 years) were analyzed separately, accounting for number of follow-up years (eg, an individual who was aged 13 years in 2006 would have 7 years of follow-up as an adolescent and 9 years as a young adult, while an individual who was aged 19 years in 2006 would have 3 years of follow-up as an adolescent and 13 years as a young adult). The count measure for each developmental stage was chosen based on the knowledge that prescription opioid use is relatively rare among adolescents and young adults and that very few will meet the criteria of previously used definitions for persistent use.32,33 Prescriptions with a reimbursement code indicating palliative care (−90) were excluded.48,49
2.4. Statistical proceduresDescriptive data on the adolescents' sociodemographics, exposure to childhood trauma, and nonopioid analgesics prescriptions were presented stratified by the follow-up periods in which the participants received opioid prescriptions and by sex. Categorical variables were described with counts and percentages; continuous variables were described with mean and SD. The half rule was used to handle missing values, meaning that participants who answered at least half of the questions were used to calculate mean scores and sum scores. Number of types of exposure to other trauma types was presented by number of types of exposure to interpersonal trauma.
The number of prescriptions of opioids, paracetamol, NSAIDs, and gabapentinoids filled in (1) adolescence (age 13-19 years) and (2) young adulthood (age 20-32 years) served as separate outcomes in zero-inflated negative binomial regression analyses. Variation in follow-up time was accounted for by offsetting for log follow-up time, resulting in incidence rate ratios that may be interpreted as ratios between rates per year.25 Exposure to each trauma type was assessed in separate complete case analyses, while number of trauma types was assessed in one complete case analysis including interpersonal trauma and other trauma types. For the subsample reporting trauma exposure, symptoms reported in adolescence were assessed in separate zero-inflated negative binomial regression analyses for the number of analgesics prescriptions filled in adolescence and young adulthood
All the described analyses were adjusted for the variables age, sex, household structure, and family economy as reported in adolescence.7,46 Analyses for prescription analgesics in adolescence were additionally adjusted for pubertal development.16,47 Separate and unadjusted zero-inflated negative binomial regression analyses were run to show the association of background variables to the outcomes. Statistical analyses were conducted using R version 4.2.2 and Stata version 17.0, with the R package data.table24 for aggregating from data on individual prescriptions to number of prescriptions for participants and Stata for estimation of zero-inflated negative binomial regression models.
3. Results 3.1. Sample descriptivesGirls and boys were evenly represented among participating adolescents in the Young-HUNT3 Study (50.3% female participants, n = 4128). During the study period, about 1 in 10 participants received opioid analgesics in adolescence and 2 in 5 received opioids in young adulthood (Table 1, Supplementary Table 2, available at https://links.lww.com/PAIN/B975). Among nonopioids, NSAIDs were prescribed to the largest proportion of participants, both in adolescence (about 2 in 5) and in young adulthood (2 in 3), while paracetamol prescriptions were received by fewer participants than opioid prescriptions, both in adolescence and in young adulthood. Very few participants received gabapentinoid prescriptions. Participants who received opioid prescriptions in both adolescence and young adulthood were overall more exposed to childhood trauma (Table 1). This cohort also received more nonopioid prescription analgesics in both developmental stages. As adolescents, participants in this cohort reported more psychological and somatic symptomatology, including post-traumatic stress, psychological distress, recurrent musculoskeletal pain, and headaches. Girls reported higher childhood exposure to sexual abuse, and boys reported higher exposure to physical violence and witnessing violence (Supplementary Table 2, available at https://links.lww.com/PAIN/B975). More female participants than male participants received opioid and nonopioid analgesics, both in adolescence and in young adulthood, and girls reported more chronic pain and psychological symptoms than boys. There was considerable overlap of exposure to different trauma types, with a substantial subgroup reporting exposure to the maximum number of types for both interpersonal trauma and other trauma (Supplementary Table 3, available at https://links.lww.com/PAIN/B975).
Table 1 - Number and proportion of participants receiving opioid analgesics in adolescence or young adulthood by background factors, trauma, and history of nonopioid analgesics. n All No prescription opioids in adolescence or young adulthood Prescription opioids in adolescence only Prescription opioids in young adulthood only Prescription opioids in adolescence and young adulthood n (%)/mean (SD) n (%)/mean (SD) n (%)/mean (SD) n (%)/mean (SD) n (%)/mean (SD) All participants 8199 8199 4314 (52.6) 378 (4.6) 2947 (35.9) 560 (6.8) Female participants 4128 4128 (50.3) 1962 (47.5) 208 (5.04) 1601 (38.8) 357 (8.7) Male participants 4071 4071 (49.7) 2352 (57.8) 170 (4.2) 1346 (33.1) 203 (5.0) Age at Young-HUNT3, mean (min 12.7, max 20.9) 8199 15.9 (1.7) 15.8 (1.7) 15.6 (1.7) 16.0 (1.7) 16.0 (1.7) Pubertal development score, mean (range 1-4) 7511 3.1 (0.7) 3.1 (0.7) 3.1 (0.6) 3.1 (0.7) 3.2 (0.6) Socioeconomic factors Family economy below average 7636 708 (9.3) 351 (8.7) 27 (7.6) 266 (9.7) 64 (12.1) Household, not living with both parents 8104 3776 (46.6) 1874 (43.9) 173 (46.3) 1433 (49.2) 296 (53.6) Direct interpersonal trauma By type Bullying 7803 628 (8.1) 284 (6.9) 22 (6.0) 257 (9.2) 65 (12.0) Physical violence 7809 789 (10.1) 340 (8.3) 29 (7.9) 340 (12.2) 80 (14.8) Sexual abuse 7829 430 (5.5) 189 (4.6) 18 (4.9) 165 (5.9) 58 (10.7) By number of types 7833 No events 6464 (82.5) 3512 (85.1) 313 (84.6) 2226 (79.7) 413 (76.1) 1 type 987 (12.6) 457 (11.1) 48 (13.0) 407 (14.6) 75 (13.8) ≥2 types 382 (4.9) 158 (3.8) 9 (2.4) 160 (5.7) 55 (10.1) Other trauma By type Witness to violence 7812 1810 (23.2) 869 (21.1) 82 (22.4) 692 (24.8) 167 (30.9) Disease or death of someone close 7848 5757 (73.4) 2979 (72.0) 278 (75.1) 2073 (74.1) 427 (78.8) Severe accident, disaster, or other traumatic event 7848 2481 (31.6) 1168 (28.2) 115 (31.0) 959 (34.3) 239 (44.0) By number of types 7863 No events 1657 (21.1) 942 (22.7) 72 (19.4) 570 (20.3) 73 (13.4) 1 type 3307 (42.1) 1803 (43.5) 168 (45.3) 1133 (40.4) 203 (37.4) 2 types 1956 (24.9) 990 (23.9) 86 (23.2) 709 (25.3) 171 (31.5) 3 types 943 (12.0) 411 (9.9) 45 (12.1) 391 (14.0) 96 (17.7) ≥1 nonopioid prescriptions in adolescence 8199 Paracetamol 646 (7.9) 193 (4.5) 89 (23.5) 215 (7.3) 149 (26.6) NSAIDs 3196 (39.0) 1243 (28.8) 270 (71.4) 1234 (41.9) 449 (80.2) Gabapentinoids 21 (0.3) <5 <5 <5 9 (1.6) ≥1 nonopioid prescriptions in young adulthood 8199 Paracetamol 2439 (29.8) 669 (15.5) 73 (19.3) 1370 (46.5) 327 (58.4) NSAIDs 5472 (66.7) 2238 (51.9) 235 (62.2) 2491 (84.5) 508 (90.7) Gabapentinoids 178 (2.2) 18 (0.4) <5 108 (3.7) 47 (8.4) Symptoms reported in adolescence Psychological distress (SCL-5, 1-4) 7961 1.50 (0.55) 1.46 (0.51) 1.49 (0.56) 1.54 (0.58) 1.64 (0.65) Post-traumatic stress symptoms (0-3) 5016 0.82 (0.99) 0.73 (0.93) 0.82 (0.98) 0.90 (1.05) 1.00 (1.07) Musculoskeletal pain, weekly 8035 2748 (34.2) 1190 (28.2) 139 (37.5) 1124 (38.9) 295 (53.5) Headaches, weekly 7619 617 (8.10) 226 (5.6) 39 (11.1) 274 (10.0) 78 (15.1)NSAIDs, nonsteroid anti-inflammatory drugs SCL-5, Hopkins Symptom Checklist, short version with five items.
The results from the regression analyses showed significant and consistent relationships between the broad range of childhood trauma exposures and higher prescription rates for opioid analgesics in both the shorter term, during adolescence, and the longer term, during young adulthood (Table 2). Patterns were similar for paracetamol and NSAIDs, although less distinct in adolescence than in young adulthood. Childhood trauma exposure was generally significantly related to higher prescription rates for NSAIDs in adolescence, whereas prescriptions for paracetamol were only significantly linked to prior exposure to severe illness or death of someone close and severe accidents, disasters, or other event (Table 2). In young adulthood, childhood trauma was significantly associated with higher prescription rates for both NSAIDs and paracetamol (Table 2).
Table 2 - Zero-inflated negative binomial regression analyses for number of prescriptions of analgesics in adolescence and young adulthood by type of traumatic events and number of types of direct interpersonal trauma and other trauma types. n Opioids Nonopioid analgesics Opioids Paracetamol NSAIDs IRR (95% CI) P IRR (95% CI) P IRR (95% CI) P Adolescence (age 12-19) n = 938 n = 646 n = 3196 Direct interpersonal trauma Bullying 7244 1.46 (1.10, 1.94) 0.009 1.33 (0.93, 1.89) 0.113 1.21 (1.04, 1.41) 0.013 Sexual abuse 7266 1.63 (1.19, 2.23) 0.002 1.08 (0.71, 1.65) 0.718 1.26 (1.06, 1.50) 0.011 Physical violence 7244 1.50 (1.17, 1.94) 0.002 1.07 (0.76, 1.50) 0.693 1.05 (0.91, 1.21) 0.510 Other trauma types Witness to violence 7245 1.17 (0.97, 1.41) 0.099 0.98 (0.77, 1.26) 0.902 1.04 (0.94, 1.15) 0.461 Severe illness or death of someone close 7269 1.37 (1.13, 1.66) 0.001 1.56 (1.23, 1.99) <0.001 1.34 (1.21, 1.48) <0.001 Severe accident, disaster, or other traumatic event 7274 1.59 (1.35, 1.88) <0.001 1.57 (1.28, 1.94) <0.001 1.30 (1.19, 1.42) <0.001 Direct interpersonal trauma, number of types 1 type 7270 0.83 (0.64, 1.07) 0.141 0.70 (0.51, 0.97) 0.033 0.93 (0.81, 1.06) 0.248 ≥2 types 7270 1.61 (1.13, 2.29) 0.008 1.22 (0.76, 1.95) 0.419 1.18 (0.97, 1.44) 0.106 Other trauma, number of types 1 type 7270 1.24 (0.99, 1.56) 0.067 1.49 (1.13, 2.00) 0.005 1.27 (1.13, 1.42) <0.001 2 types 7270 1.76 (1.37, 2.27) <0.001 1.88 (1.38, 2.57) <0.001 1.45 (1.28, 1.65) <0.001 3 types 7270 1.63 (1.19, 2.22) 0.002 1.92 (1.29, 2.87) 0.001 1.48 (1.25, 1.74) <0.001 Young adulthood (age 20-32) n = 3507 n = 2439 n = 5472 Direct interpersonal trauma Bullying 7455 1.72 (1.43, 2.06) <0.001 2.20 (1.82, 2.67) <0.001 1.49 (1.34, 1.66) <0.001 Sexual abuse 7480 1.59 (1.28, 1.98) <0.001 1.38 (1.10, 1.75) 0.006 1.24 (1.08, 1.41) 0.002 Physical violence 7460 2.66 (2.27, 3.12) <0.001 1.95 (1.63, 2.32) <0.001 1.32 (1.19, 1.46) <0.001 Other trauma types Witness to violence 7461 1.96 (1.74, 2.21) <0.001 1.51 (1.32, 1.72) <0.001 1.20 (1.11, 1.29) <0.001 Severe illness or death of someone close 7485 1.17 (1.04, 1.31) 0.008 1.39 (1.22, 1.58) <0.001 1.21 (1.13, 1.30) <0.001 Severe accident, disaster, or other traumatic event 7490 1.69 (1.52, 1.88) <0.001 1.62 (1.44, 1.82) <0.001 1.24 (1.17, 1.33) <0.001 Direct interpersonal trauma, number of types 1 type 7484 1.40 (1.20, 1.64) <0.001 1.35 (1.15, 1.60) <0.001 1.23 (1.12, 1.36) <0.001 ≥2 types 7484 1.94 (1.53, 2.46) <0.001 2.07 (1.61, 2.66) <0.001 1.35 (1.16, 1.56) <0.001 Other trauma, number of types 1 type 7484 1.02 (0.89, 1.17) 0.761 1.26 (1.08, 1.47) 0.003 1.16 (1.06, 1.26) 0.001 2 types 7484 1.48 (1.27, 1.72) <0.001 1.58 (1.33, 1.87) <0.001 1.28 (1.16, 1.41) <0.001 3 types 7484 1.82 (1.49, 2.21) <0.001 1.84 (1.49, 2.27) <0.001 1.33 (1.19, 1.50)
留言 (0)