
記住我


Pain functions to alarm for harm, enabling avoidance, escape, or withdrawal for recovery. Biological and psychological responses to pain or fear of pain can be measured at multiple levels, from the molecular to the behavioral. Capturing these changes requires multiple methodologies, and sensor-based digital technologies can provide information on, and analysis of, responses to pain. These technologies are continually improving in ease of use, methods of capture, and analysis, moving from the laboratory or clinic to the naturalistic environments that characterise daily life. Data capture in daily life, especially for sampling physiology, behavior, or self-report, is commonplace, and as technologies and their uses improve, they can be deployed passively without interference from participant awareness of measurement.
Existing reviews have quantified the benefits of technology to support exercise programmes,53,92 improve broader outcomes of treatment,55,92 or investigate use and preferences.10 Some have addressed specific uses, such as sensor data to complement self-report by people in pain, summarized in 7 reviews for adults13,53,55,75,92,93,98 and 110 in e-health interventions for children and young people. Three of these described the current state of wearable sensors in pain,75,93,98 but only 1 used systematic search methods. Most reviews nominated pain intensity as the outcome of interest, overlooking other psychological and social aspects of pain experience, such as interference in daily life and social interactions. A few reviews mention emotions associated with pain experience, but only in passing,55 or as contextual information for understanding pain intensity data.75 Given the burgeoning use of technology in mental health research,78 we were interested in the use of technology to investigate integral psychosocial aspects of pain. This scoping review addresses this gap by including relevant psychological and social constructs in our search, highlighting them in our results, and critically considering the implications of their use within our discussion.
This scoping review addresses the historical use of measurement technology assessing a broad range of pain-relevant psychological and social variables in dynamic real-world environments. In contrast to previously published reviews, we are also explicitly concerned with studies outside the laboratory, where every day people with pain face decisions and challenges without healthcare staff support. We are also concerned with the potential for data capture and analysis for use in determining states of chronic pain and transitions between those states.22 We recognize that the impact of chronic pain is dynamic (fluctuating) and contextual22; measurement in the context where pain occurs, daily life, is an important extension of our inquiry. In fact, although some technologies are particularly suitable for application in both laboratory and community settings without degrading or voiding the experimental procedures, other technologies may present methodological and technical challenges preventing their application in daily life contexts.
2. MethodsThe protocol was developed using the scoping review framework by Joanna Briggs Institute,73 preregistered and available at the Open Science Framework (OSF), doi: 10.17605/OSF.IO/3CBDG.
2.1. Research questionsFor sensors with potential application in daily life contexts and that sampled psychological and social data of interest in chronic pain, we aimed to
(1) map sensors by type; (2) describe relationships between sensor data and psychological and social variables, clarifying assumptions linking measurement of an event or state to the sensor data (“ground truth”); (3) document practical limitations and strengths of the sensors or devices in relation to the measurement tasks and their contexts; (4) document the research designs in which sensors or devices were applied; and (5) identify sensor applications that are promising but understudied in pain. 2.2 Data sources and search strategy 2.2.1. Pilot searchWith a view to capturing the full breadth of the use of sensors in studies of psychological and social variables, we ran a pilot search for studies with or without the term pain but with keywords related to disability. We then limited the search to those studies that included keywords related to psychological distress and to wearable technology compatible with home use. This first search yielded more than 10,000 results. One author (T.O.) screened these titles and then 3 authors (T.O., D.V., and A.W.) examined the results from the first title screening and decided that the search identified many titles that were (1) not directly concerned with pain or chronic pain and (2) focused exclusively on sensor feasibility without reference to any psychological or social constructs related to pain. This first search was therefore treated as a pilot search, and terms were revised for a new search that would include only pain or chronic pain studies that were also concerned with how sensor data related to existing psychological and social constructs related to pain.
2.2.2. Search strategyPubMed, PsychINFO, and Web of Science publication databases were searched from inception to December 31, 2022, for published peer-reviewed articles meeting the criteria below. The search strategy applied the term “pain” in combination with keywords related to disability or movement difficulty, limiting studies to those that contained at least 1 from a list of terms related to psychological or social constructs and to any wearable or passive sensing technology compatible with home use (see search supplementary information, available at https://links.lww.com/PAIN/B973).
2.2.3. Inclusion criteriaWe included all studies that recruited participants with either chronic pain or painful movement and that monitored at least 1 psychological or social variable. All included studies used 1 or more sensors (wearable or installed in the participant's house) to assess specific aspects of psychological (such as fear of movement or catastrophizing) or social (such as voice tone or count of social interactions) experiences related to pain.
2.2.4. Exclusion criteriaWe excluded studies that did not explore (either qualitatively or quantitatively) any relationship between sensor data and other psychological or social aspects of pain (eg, fear of movement). In addition, for relevance to chronic pain, we excluded dental studies and any other studies (such as in surgical wards) where pain might be acute and activity was constrained. We excluded studies with sensors that could not be transferred to use in daily life contexts, such as requiring specialized laboratory settings or technology that required invasive procedures (eg, blood tests, implanted sensors). We excluded studies that were based on secondary data and articles in languages other than English.
2.3. Title and abstract screeningFrom the 3 data sources, the searches identified 3139 articles that were imported into EndNote 20 software31 and deduplicated using DOI and then the EndNote 20 deduplication tool. This provided 2799 titles and abstracts. One author (T.O.) screened 461 titles from this updated search, and D.V. and A.W. screened the remaining 2338 new titles. D.V. and A.W. screened a random selection (10%) of titles screened by T.O. and calculated the ɸ reliability coefficient.32 Similarly, D.V. and A.W. screened 10% of the titles allocated to each of them. The interrater reliability between A.W. and T.O. was ɸ = 0.80, between D.V. and T.O. was ɸ = 0.84, and between D.V. and A.W. was ɸ = 0.86. All differences between reviewers were documented and resolved through consensus, leading to the inclusion of 1 article that had initially been excluded (refer to the PRISMA diagram).
2.3.1. Additional searchesThe database searches yielded 37 reviews focused on pain, chronic pain, and wearable technology. The reference lists of these reviews were screened to identify further studies leading to the inclusion of 2 additional full texts. A total of 106 full texts were retrieved and examined (refer to the PRISMA diagram).
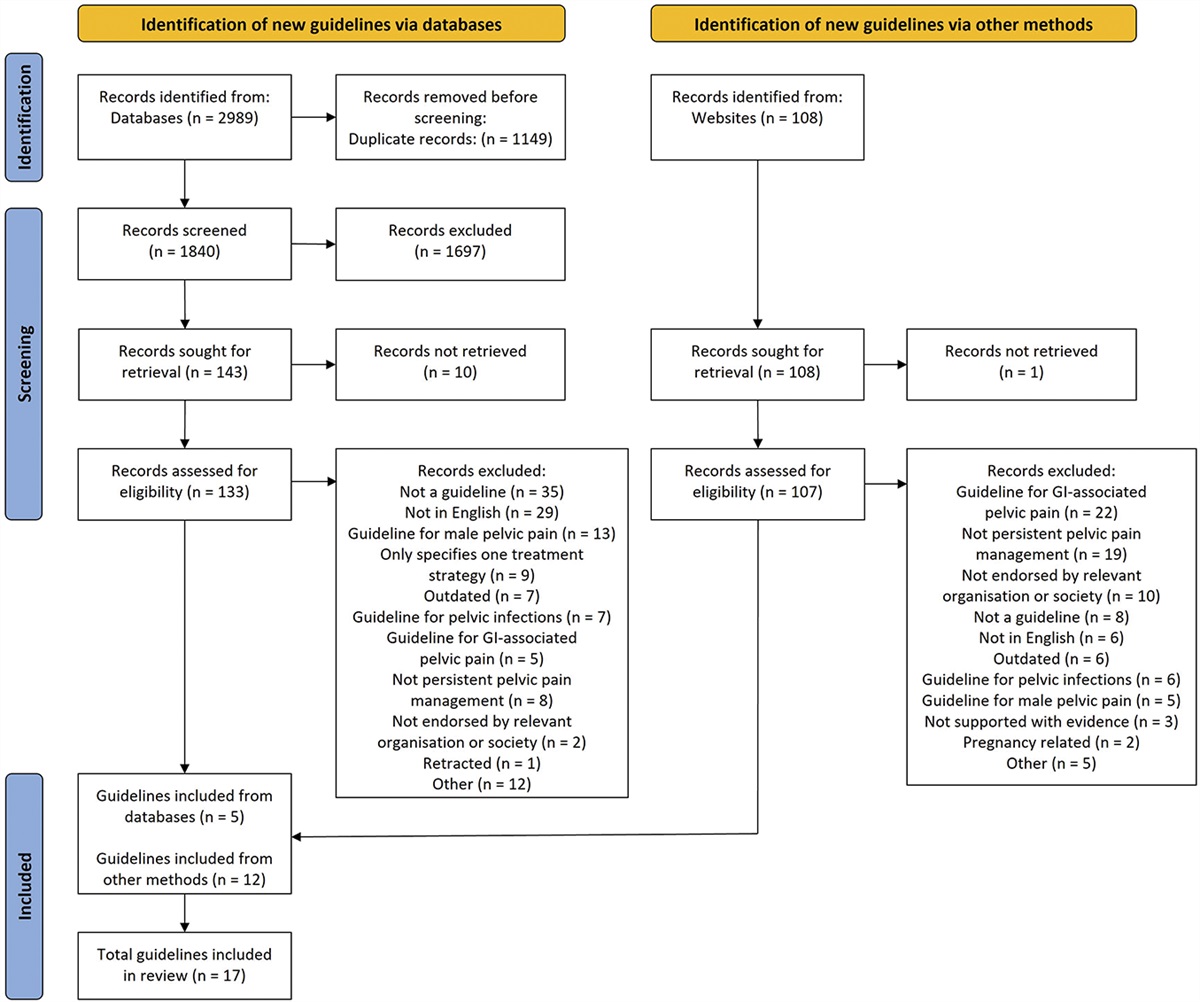
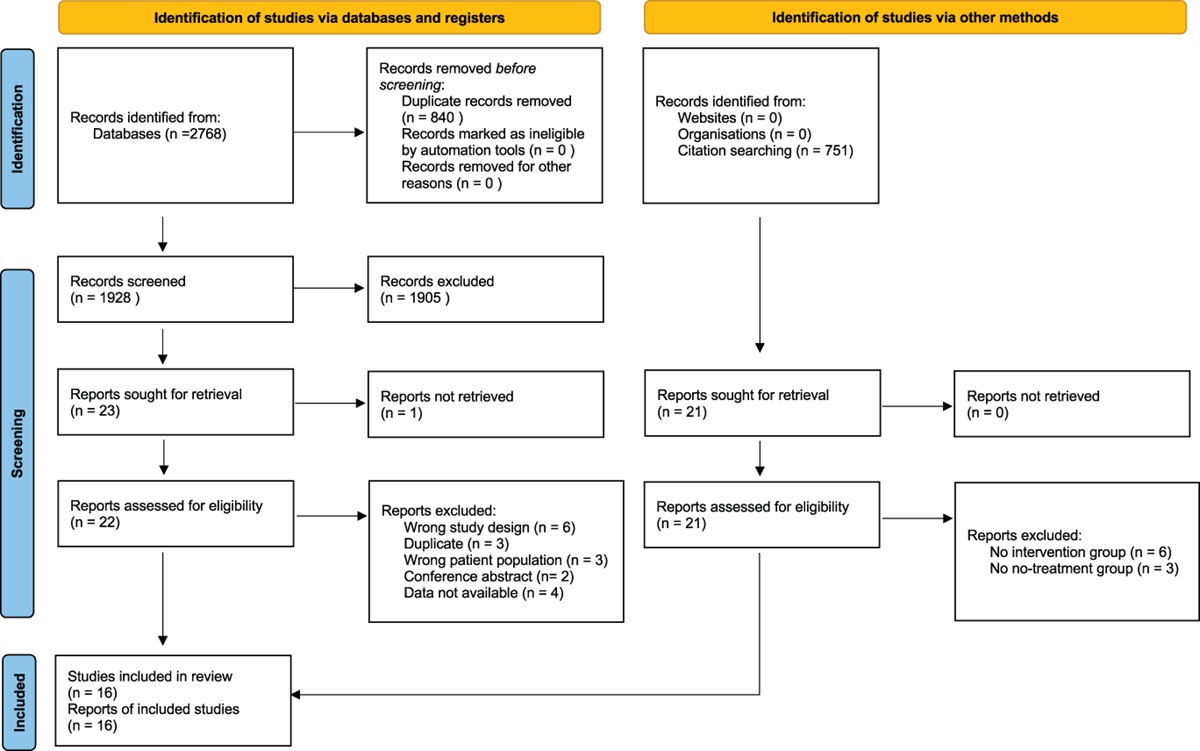
2.4. Full-text screeningFull texts were reviewed by a similar process. A.W. reviewed 23 of the 106 full texts and then reviewed an additional 15 titles that were randomly selected from those allocated to D.V. (n =83). Of the 15 full texts reviewed by both D.V. and A.W., 1 disagreement was resolved with the exclusion of 1 text. After the full-text review, the final list of full texts included was 60 (Fig. 1).
 Figure 1.:
Figure 1.: PRISMA diagram.
2.5. Data extractionTwo authors (T.O. and D.V.) extracted data, including title, year, author of publication, and key information about the sensors, how they were used, methods used to capture the experiences of interest from the sensor data, and relevant challenges reported for each technology (see supplementary information, available at https://links.lww.com/PAIN/B973).
3. ResultsConsistent with accelerating trends in the availability and affordability of wearable sensors, 48.3% of the 60 studies included in this review were published between January 1, 2018, and December 31, 2022, with the remaining 31 covering a span of 23 years (Table 1). Most of the 60 studies (71.6%) were conducted either in Europe (38.3%) or in North America (33.3%), 16.6% in Asia, 5% in Australia, and 3.3% in South America and Middle East. Of the 23 European studies, 7 were from the United Kingdom, 3 from the Netherlands, and 2 from Germany. Of the 60 studies, 46 (76.6%) involved people with chronic pain and 14 recruited subjects with acute or other nonchronic pain presentations. Almost half of the selected studies (n = 28) involved people with back pain, and overall, we identified 11 general classifications of pain or chronic pain (Fig. 2), not mutually exclusive.
Table 1 - Title and short description of studies. Author year Design Research context Pain-related condition Type of sensor Data available Age category Sample size (pain gr.) Attrition rate Mean age* Age SD* N. Female Alalawi 20221 Controlled Lab./Hosp. b1. Neck/Shoulder IMU No info provided Adults 18 0.00% 38.7 12 14 Alberts 20202 Controlled Daily life c. Cancer Resp. rate Unclear Adults 65 3.08% 44.1 8.7 35 Alcaraz 20213 Controlled Lab./Hosp. b2. Neck and low back IMU No info provided Adults 66 0.00% 40.35 13.08 25 Alschuler 20114 Longitudinal Daily life b. Back pain Accelerometer No info provided Adults 20 0.00% 46.1 9.35 9 Aung 20166 Controlled Lab./Hosp. b. Back pain IMU, EMG, 3D capt. On request Adults 22 0.00% 50.5 14.6 15 Beebe 20217 Observational Lab./Hosp. a. General/unspec. 3D capture system No info provided Children 16 15.00% 13.8 2.2 13 Birch 20228 Observational Daily life a. General/unspec. EEG On request Adults 29 44.83% 50.2 — 12 Burch 20209 Controlled Lab./Hosp. c. Cancer Heart—HR/V No info provided Adults 38 10.53% 60 3 39 Carvalho 201711 Longitudinal Daily life b. Back pain Accelerometer No info provided Adults 130 8.46% 39.1 11.2 82 Cooper 201714 Controlled Daily life e. Osteoarthritis Accelerometer No info provided Adults 67 7.46% 60.5 10.3 36 Davis 201315 Observational Lab./Hosp. a. General/unspec. IMU No info provided Adults 235 5.11% 32 — 129 de Groot 200817 Controlled Daily life e. Osteoarthritis Accelerometer No info provided Adults 84 0.00% 61.7 11 84 de Oliveira Silva 201918 Observational Lab./Hosp. b4. other MSK 3D capture system No info provided Adults 40 0.00% 22.23 3.2 40 Devecchi 202219 Observational Lab./Hosp. b1. Neck/Shoulder IMU No info provided Adults 85 0.00% 33.3 9.4 55 Dubois 201421 Controlled Lab./Hosp. b. Back pain EMG No info provided Adults 52 0.00% 39.8 11.5 18 Evans 201323 Controlled Lab./Hosp. b. Back pain Heart—HR/V No info provided Children 48 12.50% 14.2 2.6 30 Fujii 202226 Controlled Lab./Hosp. b. Back pain 3D capture system On request Adults 31 0.00% 30.5 5.2 0 Fujii 202127 Observational Lab./Hosp. b. Back pain 3D capture system On request Adults 35 0.00% 30 Range 9 Geisser 199529 Longitudinal Daily life b. Back pain EMG No info provided Adults 25 16.00% 35.1 — 9 Greenberg 202033 Longitudinal Daily life a. General/unspec. Accelerometer No info provided Adults 95 16.84% 50.7 14.7 64 Grossman 201634 Controlled Daily life f. Fibromyalgia, CRPS, WSP HR/V, RR, acc. No info provided Adults 168 22.62% 54.1 9.1 130 Hallman 201236 Controlled Daily life b1. Neck/Shoulder Heart—HR/V, accel. No info provided Adults 23 17.39% 40.5 7.1 21 Hallman 201435 Controlled Daily life b1. Neck/Shoulder Heart—HR/V, accel. No info provided Adults 29 6.90% 41 10 13 Imai 202238 Observational Lab./Hosp. b. Back pain 3D capture system No info provided Adults 54 0 47.1 11.1 25 Imai 202239 Longitudinal Lab./Hosp. b3. other MSK Accelerometer No info provided Adults 20 0.00% 69.7 10.2 18 Jacobson 202140 Longitudinal Daily life f. Fibromyalgia, CRPS, WSP Accelerometer Public Adults 68 — 41.3 8.1 48 Jette 201641 Observational Lab./Hosp. a. General/unspec. IMU No info provided Adults 32 0.00% 32.9 7.83 19 Kashikar-Zuck 201042 Longitudinal Daily life f. Fibromyalgia, CRPS, WSP Accelerometer No info provided Children 104 0.00% 14.9 1.8 93 Kent 201543 Controlled Daily life b. Back pain IMU On request Adults 112 24.11% 39 12 61 Khan 202244 Observational Lab./Hosp. b. Back pain IMU No info provided Adults 121 0.00% 55 10 62 Kim 201745 Longitudinal Daily life a. General/unspec. Camera + PIR* No info provided Elderly 20 0.00% — — — Knox 200646 Controlled Lab./Hosp. b1. Neck/Shoulder Electrogoniometer No info provided Adults 9 0.00% 39 9 7 Korszun 200247 Controlled Daily life f. Fibromyalgia, CRPS, WSP Accelerometer No info provided Adults 22 0.00% 48 3 24 Lamoth 200648 Controlled Lab./Hosp. b. Back pain 3D capture system, EMG No info provided Adults 22 13.64% 38 — 13 Lewis 201250 Controlled Lab./Hosp. b. Back pain EMG No info provided Adults 42 9.52% 46.2 11.1 29 Liguori 202151 Observational Lab./Hosp. n. Parkinson Dis. IMU No info provided Adults 26 0.00% 65.4 8.7 8 Liikkanen 202252 Controlled Daily life b. Back pain VR set, EDA, acc. On request Adults 39 0.00% 54.7 — 34 Matheve 201854 Controlled Lab./Hosp. b. Back pain IMU On request Adults 54 18.52% 43 12 18 Mora 201259 Controlled Lab./Hosp. b3. other MSK EMG No info provided Adults 36 7.69% 27.4 6.8 28 Murphy 201360 Longitudinal Daily life e. Osteoarthritis Accelerometer No info provided Adults 172 18.60% 72 6 107 Nijs 200862 Observational Lab./Hosp. f. Fibromyalgia, CRPS, WSP HR/V, resp. rate No info provided Adults 36 0.00% 39 8 36 Nishi 202264 Controlled Lab./Hosp. b. Back pain Force plat., Elect. Gon. No info provided Adults 48 0.00% 54.46 13.08 36 Nishi 202165 Controlled Lab./Hosp. B. Back pain Accelerometer No info provided Adults 20 0.00% 54.05 10.76 9 Nordstoga 201967 Longitudinal Lab./Hosp. B. Back pain IMU No info provided Adults 44 31.82% 45.1 14.7 17 Osumi 201870 Observational Lab./Hosp. f. Fibromyalgia, CRPS, WSP 3D capture system Unclear Children 1 0.00% 13 — — Osumi 201971 Controlled Lab./Hosp. B. Back pain Electrogoniometer No info provided Adults 45 0.00% 56.23 10.61 Ozcan Kahraman 201872 Observational Lab./Hosp. b. Back pain Force platform No info provided Adults 51 0.00% 39 — 25 Reinen 202274 Observational Daily life b. Back pain Acc., microphone No info provided Adults 121 4.13% 59.4 — 70 Sarig Bahat 201477 Observational Lab./Hosp. b1. Neck/Shoulder VR set No info provided Adults 25 0.00% 39 12.7 19 Singh 201680 Observational Lab./Hosp. b. Back pain Acc., resp. rate No info provided Adults 15 — — — 10 Singh 201779 Observational Daily life b. Back pain Accelerometer No info provided Adults 4 0.00% — — 4 Svendsen 201383 Controlled Lab./Hosp. b. Back pain EMG No info provided Adults 12 0.00% 38.6 9.8 3 Thomas 200785 Observational Lab./Hosp. b. Back pain 3D capture system No info provided Adults 36 0.00% 26.85 6.68 23 Thomas 200886 Observational Lab./Hosp. b. Back pain
留言 (0)