
記住我



Patellar tendon ruptures are relatively rare injuries that disrupt the distal aspect of the extensor mechanism. The injury is most commonly seen in men in their third or fourth decade of life and in those with systemic conditions that compromise tendon integrity.1 Primary repair is the mainstay of treatment of complete patellar tendon ruptures. Historically, this was primarily achieved with transosseous tunnels; however, suture anchors can also be used and have been reported to be gaining in popularity.1 In acute or chronic tears where the tendon cannot be adequately repaired, reconstruction can be achieved with various allograft and autograft options.
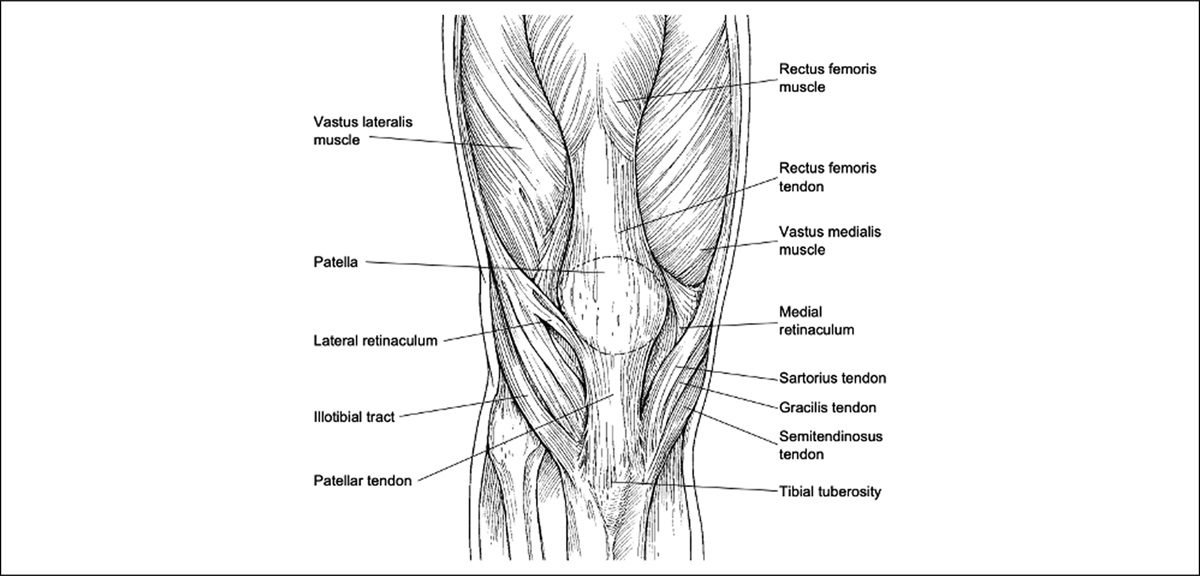
AnatomyThe patellar tendon comprises the distal aspect of the extensor mechanism and extends from the inferior pole of the patella to the tibial tubercle (Figure 1). By definition, it is a ligament rather than tendon because it extends from bone to bone rather than muscle to bone. However, it is commonly referred to as a tendon because it represents the quadriceps tendon extension distally before insertion in the tubercle.1
 Figure 1:
Figure 1: Image showing normal anatomy of the patella and surrounding structures.
The proximal width of the tendon is that of the inferior patella, and it narrows distally before inserting in the tibial tubercle. In a series of 53 patients in which the patellar tendon was harvested as a graft, the mean patellar length and central width were 39 mm and 32 mm, respectively.2 Reports of the tendon's thickness ranged between 4.0 mm and 10.9 mm with tendinopathy indicated with measurements greater than 7.0 mm.3 The blood supply comes from three main sources: the inferior-lateral genicular artery, an anastomotic arch between the inferior medial genicular artery and anterior tibial recurrent artery, and retropatellar from Hoffa fat pad. Compared with the well-vascularized midportion, the proximal and distal aspects of the tendon are relatively avascular and are consequently the most common sites of rupture.4
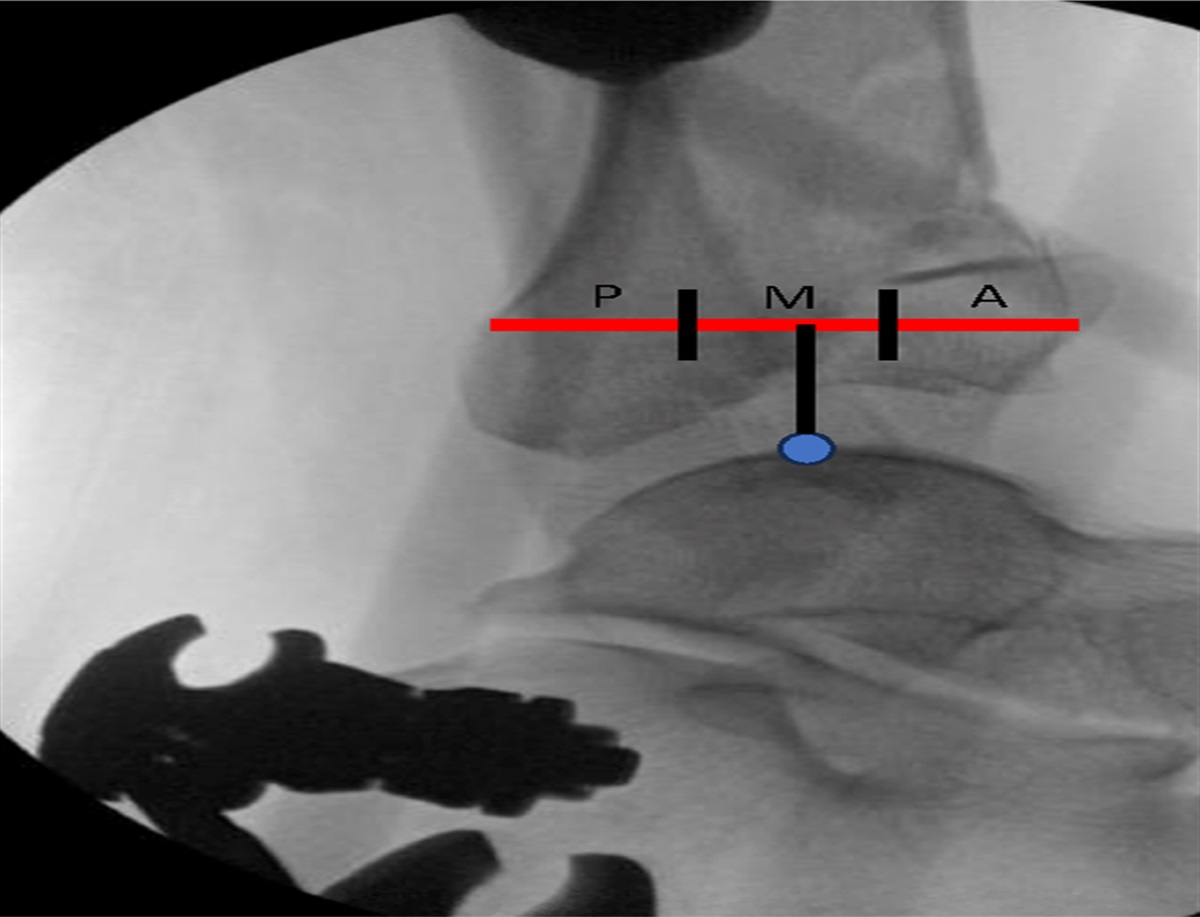
BiomechanicsDuring active knee extension, force is transferred from the quadriceps muscle group to the tibia through the patellar tendon and retinaculum. Increasing flexion is associated with a more proximal patellofemoral contact point, causing the patellar tendon to take on greater stress than the quadriceps tendon. Consequently, most patellar tendon ruptures occur with the knee in flexion.1 Several studies have evaluated the differences in tendon strength and stress based on location. In a cadaveric study, tensile stresses were shown to increase in the anterior portion and decrease in the posterior aspect of the tendon throughout knee flexion.5 Correspondingly, a biomechanical study of young healthy men showed the anterior portion of the tendon has markedly greater peak and yield stress when compared with the posterior fibers.6 In the sagittal plane, the end regions of the tendon near the bony insertions undergo strain that is three to fourfold higher than the mid-substance, which may explain the higher rate of tears near osseous insertion.7
It is estimated that a force of 17.5 times an individual's body weight is required to rupture the tendon in the absence of preexisting tendon degeneration.8 Ruptures of the patellar tendon occur in response to extensor mechanism tensile overload, most commonly involving a knee flexion force against an eccentrically contracted quadriceps muscle. In professional athletes, ruptures have also been associated with ankle plantarflexion and knee valgus.9
Epidemiology and Risk FactorsSeveral risk factors for acute patellar tendon rupture have been reported. Systemic medical conditions that compromise tendon integrity, such as connective tissue disorders, chronic renal failure, systemic lupus erythematosus or rheumatoid arthritis, as well as corticosteroid use increase the risk of tendon rupture.10,11 Although the US Food and Drug Administration issued a warning of elevated risk of tendon rupture after use of fluoroquinolone antibiotics,12 several studies have shown that tendon rupture after fluoroquinolone exposure is rare and not clinically meaningful.13,14 Increasing age and black race have also been identified as risk factors in the military population.15 For local factors, intratendinous corticosteroid injection is believed to stimulate bony or adipose formation within the patellar tendon, predisposing it to rupture.10 However, there are limited data or case reports of this related to the patellar tendon specifically. Another local risk factor involves repeated overuse and microtrauma, particularly in jumping athletes, which can lead to patellar tendinopathy. This is otherwise known as “jumper's knee” and may predispose to partial or complete rupture.16 ln the general population, the reported incidence of patellar tendon ruptures ranges between 0.48 and 1.09 per 100,000 person-years.17,18 However, in the active military population, the incidence reaches as high as six per 100,000 person-years.15 The incidence of the injury is reported to be increasing and can potentially be explained by a more active aging population.18
Diagnosis and Radiological WorkupA history of complete patellar tendon ruptures classically involves a sudden pain and popping sensation during loaded eccentric knee flexion. On clinical examination, patients typically present with tense knee hemarthrosis and an inability to bear weight on the affected extremity. Notable findings more supportive of patellar tendon rupture compared with intra-articular injury (eg, an anterior cruciate or meniscus tear) include lack of active knee extension or inability to perform an active straight leg raise. High-riding patella or palpable tendon gap may also be evident. Importantly, if retinacular tissues remain in continuity, the patient may be able to maintain a straight leg raise despite a ruptured patellar tendon. Partial patellar tendon tears are more of an indolent process and are commonly seen in athletes after continued activity in the setting of patellar tendinopathy.19
Workup can include radiographs, ultrasonography, or magnetic resonance imaging (MRI). On the lateral radiograph, patella alta can be evident and confirmed with an Insall-Salvati20 ratio greater than 1.2, Blackburne-Peel21 ratio greater than 1.0, or Caton Deschamps22 ratio greater than 1.3 (Figure 2). The merchant view can also reveal a bare appearing trochlear groove, or “Empty Merchant Sign”, which has a higher reported specificity and positive predictive value than lateral radiographs (Figure 3).23
 Figure 2:
Figure 2: Radiographs showing the measures of Insall-Salvati, Blackburne-Peel, and Caton Deschamps ratios.
 Figure 3: Images demonstrating the “empty merchant” sign. White dotted line outlines the patella retracted proximally, out of the groove and tilted with the inferior pole pointing anteriorly. From Mirzayan et al. with permission.19
Figure 3: Images demonstrating the “empty merchant” sign. White dotted line outlines the patella retracted proximally, out of the groove and tilted with the inferior pole pointing anteriorly. From Mirzayan et al. with permission.19High-resolution ultrasonography can be used to examine both partial and complete patellar tendon injuries.1 With an acute rupture, sagittal images display a confluent area of hypoechogenicity along the hyperechoic patellar tendon. Disruption of the normal echo pattern traversing the full thickness of the tendon indicates a complete tear. Similarly, partial tendon ruptures can be quantified by measuring the length of the hypoechoic lesion through the hyperechoic tendon in longitudinal projection.24 Although ultrasonography is convenient and cost-effective, it is operator dependent, and concerns exist regarding its reliability to diagnose patellar tendon ruptures.1
Evaluation with MRI is the most sensitive modality and can help determine partial versus full thickness tears, the location of tear, tendon degeneration, and concomitant soft-tissue injuries.25 The normal patellar tendon demonstrates homogeneous low signal intensity and smooth and distinct anterior and posterior margins. By contrast, wavy and discontinuous tendon fibers are visualized after acute rupture.1 An increase in signal intensity on sagittal T2-weighted images can also be indicative of rupture.26 With a partial tear, MRI can be used to accurately measure the percentage of tendon torn and guide treatment decisions.19
Partial Thickness RupturesPopkin and Golman provide a classification for partial patellar tendon tears that boasts a high interrater and interrater reliability.19 The tear classification is based on tendon anterior-posterior thickness and the percentage of tendon torn. The authors also propose that the classification can be used to assist treatment decision making, with surgical débridement and possible repair recommended for grade 4 tears that fail 6 months of conservative treatment (Table 1).
Table 1 - Popkin-Golman Classification Grade Definition Treatment 1 No tear, tendon thickness < 8 mm Bracing treatment, PT, +/− NSAIDs 2 Tear thickness <25% Bracing treatment, PT, +/− NSAIDs, PRP, ESWT 3 Tear thickness 25-50% Bracing treatment, PT, +/− NSAIDs, PRP, ESWT, dry needling 4 Tear thickness >50% Bracing treatment, PT, +/− NSAIDs, PRP, ESWT, dry needling, surgery after 6 monthsPopkin-Golman classification for partial thickness patellar tendon ruptures. PT, physical therapy; NSAIDs, nonsteroidal anti-inflammatory medication; PRP, platelet-rich plasma; ESWT, extracorporeal shock wave therapy.
Partial thickness ruptures are usually managed with nonsurgical strategies. Acute incomplete ruptures with intact extensor mechanisms are typically treated in immobilization in full extension with weight bearing in a hinged knee brace. For rehabilitation, Karlsson et al24 reports a protocol that progresses through three phases: the acute phase, the rehabilitation phase, and the return-to-activity phase. The acute phase lasts 0 to 14 days and aims to mitigate the effects of immobilization through isometric quadriceps exercises and stretching. Rehabilitation and return-to-activity phases are integrated, lasting 3 to 6 months. The rehabilitation phase involves full mobilization, concentric and eccentric exercises, and jogging exercises. In the return-to-activity phase, dynamic exercises are added to stimulate elasticity of the tendon and improve coordination. In addition to rehabilitation, dry needling, percutaneous ultrasonic débridement, and extracorporeal shockwave therapy have been reported with variable efficacy.27–29
Select investigations have quantified the rate at which partial patellar tendon tears require surgical intervention. In the Golman et al19 series of 56 partial patellar tendon tears, 11 (20%) patients underwent surgery. Of them, nine underwent débridement alone, and two underwent suture anchor fixation. As all 11 surgical patients had a tear >50% tendon thickness, the authors report that a tear greater than 55% of tendon thickness is predictive of need for surgical treatment. Karlsson et al24 report on a separate series of partial ruptures that comprised 91 knees. Altogether, 27 (29.6%) knees were treated with surgery involving débridement and curettage where necessary. In this series, partial ruptures were graded according to length of tear as measured on ultrasonography: Grade 1 < 10 mm, grade II 10 to 20 mm, grade III >20 mm. Overall need for surgery was highest in grade III (38.5%) and lowest in grade I (6.6%). The authors conclude that failure of conservative management can be predicted to some degree by measuring tear length. Outcomes of partial patellar tendon repair are limited; however, in the Karlsson series, short-term results were excellent or good in 25 (92.5%) of surgical patients. The ideal timing of surgery in cases of partial tears remains unknown.
Complete Thickness Rupture TechniqueThe standard treatment of complete patellar tendon ruptures is surgical repair to afford restoration of the extensor mechanism and thus return to function. Most complete patellar tendon ruptures occur near its insertion point on the inferior patella.7 However, they can also occur at the mid-substance, which predisposes to a more challenging repair because of poorer tissue quality.30 Regardless of rupture location, repair is indicated for patients of all ages irrespective of the activity level. Furthermore, repair is recommended to be performed as soon as possible after recognition of the injury to facilitate the healing and rehabilitation process.1 There are numerous fixation, augmentation, and technique options when considering repair.
Although many repair techniques have been reported, repair with transosseous tunnels is the most popular.31,32 This technique typically includes two to four bone tunnels through which sutures are passed and tied (Figures 4 and 5). Suture fixation into the tendon is critical for adequate repair, and various suture techniques have been reported. The most reported suture techniques include the Mason Allen, Bunnel, and Krackow suture techniques.33,34 The Krackow method is commonly reported and uses locking running suture through the tendon. Despite its many throws, the Krackow technique has been shown to not markedly alter the vascularity of the tendon on advanced imaging.35
 Figure 4:
Figure 4: Images illustrating the surgical technique involving patellar bone tunnels and their locations.
 Figure 5:
Figure 5: Image illustrating the fixation technique using patellar bone tunnels plus Krackow suture fixation.
To avoid transosseous tunnels, repair can also be performed using suture anchors in place. Capiola et al describe a technique using suture anchor fixation to the inferior pole of the patella with tendon fixation using a 6-strand Krackow technique.36 Reported benefits of this technique include less invasive exposure, decreased risk of penetrating patellar articular cartilage, shorter surgical time, and more accurate recreation of the patellar tendon footprint on the inferior patella.36 A modified technique has also been reported using cortical buttons instead of suture anchors to afford a stronger repair.37
In cases of frayed tendon edges or tendon gapping limiting the strength of the above techniques, augmentation can be performed with suture, cable wire, allografts, or autografts. Reported benefits of augmentation include decreased strain across the repair, which may result in earlier knee motion and less tendon gapping.38 Augmentation with hamstring autograft is a commonly reported technique and involves a doubled hamstring graft that is inserted into the distal patellar pole socket and sutured to the native tendon (Figure 6). In the revision setting or cases involving poor tendon quality, a cerclage wire can be placed circumferentially around the patella and fixed to the tubercle to support repair. Transosseous repair with woven surgical mesh augmentation has also been reported to increase resistance to gap formation after repair.39
 Figure 6:
Figure 6: Image illustrating patellar tendon repair using suture tendon repair augmented by semitendinosus autograft.
Internal bracing treatment is another method for acute patellar tendon repair. This technique uses high strength suture tape and knotless anchors to provide biomechanical stability of the repaired tendon.40 A modified technique has also been described using bone tunnels in the patella and cortical buttons on the tibia with suture tape whipstitched through the tendon.41 Enhanced fixation, immediate postoperative mobilization, and early functional recovery are reported benefits of internal bracing treatment techniques.40,41
Platelet-rich plasma (PRP) and the application of engineered tissue are more recently evaluated techniques to improve patellar tendon tissue regeneration and functionality in the instance of tendon injury.42 In 2012, Almeida et al43 showed that PRP had a beneficial effect on patellar tendon healing and pain postoperatively after harvest for anterior cruciate ligament reconstruction. Since this time there have been several studies and systematic reviews that have demonstrated mixed results regarding the use of PRP for patellar tendinopathy.44–46 In the acute tear setting, it remains unknown if PRP offers any benefit. However, a case in which rupture occurred after PRP use for chronic tendinopathy has been reported.47 Additional studies will contribute to understanding the role and expectations of PRP in the management of acute patellar tendon tears. Collagen and fibrin gel scaffolds have also been reported as treatment options and have nearly replicated the native tendon tensile strength.42 However, long-term clinical outcomes of synthetic scaffolds have exhibited high rates of implant rupture and synovitis.48 To date, tissue scaffolds and biomaterials remain unable to fulfill the complex physical, mechanical, and morphological requirements of native tendons.
Postoperative RehabilitationHistorical postoperative protocols after repair called for long periods of immobilization. However, more recent protocols have emphasized early range of motion to avoid stiffness, patella baja, persistent pain, and weakness associated with prolonged immobility.49 Furthermore, early joint range of motion is recognized to stimulate tendon healing and perhaps shorten the overall rehabilitation time. To achieve early range of motion, augmentation strategies have been developed to increase the strength of repair and limit gapping with early stress to the repair.
Various early range of motion protocols have been reported. Outcomes have demonstrated that early range of motion is safe, feasible, and decreases the time to full range of motion and strength.50 The optimal postoperative protocol remains unknown, although West et al51 report a protocol that was associated with device-free ambulation at an average of 7.7 weeks in their series on 30 patients undergoing patellar tendon repair. In this series, patients kept their leg elevated for 48 hours after surgery. A hinged knee brace was used for the following 5 to 7 days with daily wound checks. From this time point until week 6, daily active range of motion between 0 and 55 degrees of flexion was performed. During this time, patients were permitted to weightbear as tolerated with locked extension. At 6 weeks postoperatively, patients were allowed to perform full active knee flexion and ambulate without the brace.
Biomechanical OutcomesSeveral biomechanical studies have evaluated differences between repair techniques. In 2006, Bushnell compared suture anchors and transosseous tunnels on 12 cadaveric knees and found markedly less gap formation after 250 cycles in the suture anchor group.52 In a larger cohort of 30 knees, Ettinger et al reported markedly greater ultimate failure loads in addition to less gap formation after cyclic loading in the absorbable as well as titanium suture anchor cohorts when compared with transosseous tunnels.53 The authors noted that failure was typically a result of failure of the eyelet in the absorbable anchor group and suture rupture in the titanium group. These findings were further corroborated by Lanzi et al54 in a study on 24 porcine specimens that found markedly less gap formation and higher load to failure with suture anchor versus transosseous tunnels. In a systematic review and meta-analysis of seven studies and a total of 128 cadaveric knees, Imbergamo et al32 found markedly less gap formation in the suture anchor cohort but did not reveal any notable difference in ultimate load to failure. In a separate meta-analysis, suture anchors again demonstrated favorable biomechanical properties in terms of gap formation when compared with transosseous tunnels.55 The authors also found most suture anchor failures were in cases of titanium anchors.
Biomechanical studies have also been performed on specific technique modifications. Ode et al37 compared cyclic gap formation and failure rate between transosseous, suture anchor, and cortical button fixation in 23 cadaveric knees. The cortical button group demonstrated markedly less gap formation than the suture anchor and suture repair groups, up to 20 cycles and 250 cycles, respectively. In addition, the cortical button knees demonstrated markedly higher loads to failure. The authors conclude that there is a clear biomechanical advantage of cortical button fixation although investigations have not yet proven any clinical benefit.
A number of biomechanical studies have evaluated the impact of augmentation strategies. In an investigation of 60 porcine models, Schliemann et al56 noted markedly higher maximal loads and less tendon elongation of both polydioxanone suture and cable wire augmentation strategies when compared with suture anchor repair alone. Black et el found a 68% increase in gap formation in the standard repair group compared with figure-of-eight suture augmentation on transosseous fixation at 250 cycles.38 The suture augmentation group also demonstrated a markedly higher mean load to failure. Similarly, Gould et al57 reported markedly less displacement in suture tape augmentation up to 1,000 cycles compared with standard transosseous repair, although there were no difference in load to failure. A notable increase in yield load has been noted with supplemental fixation using suture anchor internal brace with suture tape.58 In this series of 32 cadaveric knees, the augmented group demonstrated comparable strength to augmentation with an 18-gauge wire. Additional study is needed to determine benefit of these augmentation strategies, although it is hypothesized that a stronger repair can prevent loss of reduction, reduce failure, and allow for earlier postoperative mobilization.
Clinical OutcomesOutcomes after primary repair are generally favorable. Specifically, excellent outcomes can be expected with early repair, with poorer outcomes in cases of delayed repair.59 Belhaj et al60 report the longest-term follow-up of patellar tendon suture anchor repair in their series of 25 patients. At a median of 75-month follow-up, patients demonstrated markedly improved Knee Society pain and function scores and decreased pain compared with preoperative scores. However, knee extension strength was markedly lower on the surgical versus nonsurgical side. There was no extension deficit, which has also been shown in smaller retrospective series.50 Reported risk factors for poorer outcomes after repair include female sex, non-White race, and lower preoperative function. Overall failure rates between techniques were compared in a systematic review that included 503 patients across 41 manuscripts.61 They found that in the acute setting, primary repair with augmentation with either cables or suture resulted in the best clinical results with an overall failure rate of 2%. In the chronic setting, autograft reconstruction markedly outperformed primary repair.61
Fredericks et al15 report on a large series of 504 patients who underwent primary patellar tendon repairs in the military population. Fixation method was 81% bone tunnels, 7% suture anchors, and 12% were unknown. Overall return to previous activity occurred in 76% of patients, with 15% returning on a limited basis. Rerupture occurred in 3% of the series, with identified risk factors of Black race and age between 35 to 44 years. Not surprisingly, return to work is reported to be higher in the nonmilitary population with a review of 757 patellar tendon repairs noting an overall return to work rate of 95.8%.62
Clinical outcomes and return to sport have specifically been evaluated in a number of studies in the athletic population. A systematic review of athletes who underwent patellar tendon repair of any surgical method found an overall return to recreational activity of 88.9%.62 However, only 70.9% of professional athletes were able to return to preinjury level of sport in this series. Boublik and colleagues63 evaluated the outcomes of 24 patellar tendon tears in National Football League athletes. In 79.2% of cases, the athlete was able to return to at least one game. The authors note that although the injury is typically season ending, acute surgical repair generally results in good functional outcomes. Nguyen et al performed a separate analysis of 103 professional baseball, basketball, American football, and soccer athletes.64 They found that football athletes had the lowest return to sport rate overall, had the worst postoperative outcome, and demonstrated the greatest decrease in career lengths. Basketball athletes played less games the subsequent season after injury, and soccer athletes showed a temporary decrease in performance that normalized by postoperative season two.
Clinical studies comparing patellar repair techniques are somewhat limited. O'Dowd et al17 performed a retrospective review of 374 knees that underwent primary repair of patellar tendon rupture. The cohort included 321 transosseous and 53 suture anchor repairs over a 10-year span. The suture anchor group demonstrated notable decrease in rerupture rate as compared with the transosseous group (7.5% vs. 0%). There were otherwise no detectable differences in revision surgery rate, infections, or time to release from medical care between the cohorts. The authors conclude that their findings are compatible with biomechanical studies and that suture anchors may be a preferred technique owing to the benefit of decreased rerupture rates. Additional randomized controlled trials are needed for more rigorous analysis between the two techniques. In addition, insight may be gained from further analysis of technique modifications and various augmentation strategies.
ConclusionPatellar tendon rupture can be a devastating injury if not managed properly. Partial tears can often be managed successfully with temporary immobilization in extension, followed by progressive rehabilitation. Surgical repair is the mainstay of treatment of complete ruptures and can involve a variety of techniques. Suture anchor fixation and augmentation strategies are growing in popularity and have demonstrated favorable biomechanical results when compared with bone tunnels alone. However, any clinical benefit of these techniques remains unknown. The ideal rehabilitation strategy remains in question although early range of motion protocols appear to be safe and effective. Although professional athletes may have their careers shortened as a result of patellar tendon tears, return to activity in the general population remains high.
References 1. Matava MJ: Patellar tendon ruptures. J Am Acad Orthopaedic Surgeons 1996;4:287-296. 2. Zooker C, Pandarinath R, Kraeutler MJ, Ciccotti MG, Cohen SB, DeLuca PF: Clinical measurement of patellar tendon: Accuracy and relationship to surgical tendon dimensions. Am J Orthop (Belle Mead NJ) 2013;42:317-320. 3. Nishida Y, Nishino T, Tanaka K, Onishi S, Kanamori A, Yamazaki M: An Objective measure of patellar tendon thickness based on ultrasonography and MRI in University athletes. J Clin Med 2021;10:4092. 4. Scapinelli R: Studies on the vasculature of the human knee joint. Acta Anat (Basel) 1968;70:305-331. 5. Almekinders LC, Vellema JH, Weinhold PS: Strain patterns in the patellar tendon and the implications for patellar tendinopathy. Knee Surg Sports Traumatol Arthrosc 2002;10:2-5. 6. Haraldsson BT, Aagaard P, Krogsgaard M, Alkjaer T, Kjaer M, Magnusson SP: Region-specific mechanical properties of the human patella tendon. J Appl Physiol 2005;98:1006-1012. 7. Woo S, Maynard J, Butler D, et al.: Ligament, tendon, and joint capsule insertions to bone, in Woo SL-Y, Buckwalter JA, eds: Injury and Repair of the Musculoskeletal Soft Tissues. Park Ridge, Ill, American Academy of Orthopaedic Surgeons, 1988, pp 133-166. 8. Zernicke RF, Garhammer J, Jobe FW: Human patellar-tendon rupture. J Bone Joint Surg Am 1977;59:179-183. 9. Yüce A, Yerli M, Mısır A: The injury mechanism of knee extensor mechanism rupture in professional athletes: A video analysis study. Indian J Orthop 2022;56:1737-1744. 10. Zhang J, Keenan C, Wang JH-C: The effects of dexamethasone on human patellar tendon stem cells: Implications for dexamethasone treatment of tendon injury. J Orthop Res 2013;31:105-110. 11. Pritchard CH, Berney S: Patellar tendon rupture in systemic lupus erythematosus. J Rheumatol 1989;16:786-788. 12. van der Linden PD, Sturkenboom MCJM, Herings RMC, Leufkens HGM, Stricker BHC: Fluoroquinolones and risk of achilles tendon disorders: Case-control study. BMJ 2002;324:1306-1307. 13. Ross RK, Kinlaw AC, Herzog MM, Jonsson Funk M, Gerber JS: Fluoroquinolone antibiotics and tendon injury in adolescents. Pediatrics 2021;147:e2020033316. 14. Baik S, Lau J, Huser V, McDonald CJ: Association between tendon ruptures and use of fluoroquinolone, and other oral antibiotics: A 10-year retrospective study of 1 million US senior medicare beneficiaries. BMJ Open 2020;10:e034844. 15. Fredericks DR, Slaven SE, McCarthy CF, et al.: Incidence and risk factors of acute patellar tendon rupture, repair failure, and return to activity in the active-duty military population. Am J Sports Med 2021;49:2916-2923. 16. Lian OB, Engebretsen L, Bahr R: Prevalence of jumper’s knee among elite athletes from different sports: A cross-sectional study. Am J Sports Med 2005;33:561-567. 17. O'Dowd JA, Lehoang DM, Butler RR, Dewitt DO, Mirzayan R: Operative treatment of acute patellar tendon ruptures. Am J Sports Med 2020;48:2686-2691. 18. Lyons JG, Mian HM, Via GG, Brueggeman DA, Krishnamurthy AB: Trends and epidemiology of knee extensor mechanism injuries presenting to United States emergency departments from 2001 to 2020. Phys Sportsmed 2023;51:183-192 19. Golman M, Wright ML, Wong TT, et al.: Rethinking patellar tendinopathy and partial patellar tendon tears: A novel classification system. Am J Sports Med 2020;48:359-369. 20. Insall J, Salvati E: Patella position in the normal knee joint. Radiology 1971;101:101-104. 21. Blackburne JS, Peel TE: A new method of measuring patellar height. J Bone Joint Surg Br 1977;59:241-242. 22. Caton J, Deschamps G, Chambat P, Lerat JL, Dejour H: [Patella infera. Apropos of 128 cases]. Rev Chir Orthop Reparatrice Appar Mot 1982;68:317-325. 23. Mirzayan R, Hill PS, Batech M, Suh BD, DeWitt DO, Heckmann N: The “Empty Merchant Sign” in acute patellar tendon ruptures. Clin Imaging 2021;70:25-32. 24. Karlsson J, Kälebo P, Goksör LA, Thomée R, Swärd L: Partial rupture of the patellar ligament. Am J Sports Med 1992;20:390-395. 25. Swamy GN, Nanjayan SK, Yallappa S, Bishnoi A, Pickering SAW: Is ultrasound diagnosis reliable in acute extensor tendon injuries of the knee? Acta Orthop Belg 2012;78:764-770. 26. Yu JS, Petersilge C, Sartoris DJ, Pathria MN, Resnick D: MR imaging of injuries of the extensor mechanism of the knee. Radiographics 1994;14:541-551. 27. Thijs KM, Zwerver J, Backx FJG, et al.: Effectiveness of shockwave treatment combined with eccentric training for patellar tendinopathy: A double-blinded randomized study. Clin J Sport Med 2017;27:89-96. 28. van Leeuwen MT, Zwerver J, van den Akker-Scheek I: Extracorporeal shockwave therapy for patellar tendinopathy: A review of the literature. Br J Sports Med 2009;43:163-168. 29. Zhang ZJ, Lee WC, Fu SN: One session of extracorporeal shockwave therapy-induced modulation on tendon shear modulus is associated with reduction in pain. J Sports Sci Med 2020;19:309-316. 30. Jain S, Jain AK, Dhammi IK, Modi P: Neglected patellar tendon rupture treated by trans-osseous encirclage wire and turn-O-flap: Case report. J Orthop Case Rep 2014;4:5-8. 31. Massey PA, Myers M, McClary K, Brown J, Barton RS, Solitro GF: Biomechanical analysis of patellar tendon repair with knotless suture anchor tape versus transosseous suture. Orthop J Sports Med 2020;8:2325967120954808. 32. Imbergamo C, Sequeira S, Bano J, Rate WR, Gould H: Failure rates of suture anchor fixation versus transosseous tunnel technique for patellar tendon repair: A systematic review and meta-analysis of biomechanical studies. Orthop J Sports Med 2022;10:23259671221120212. 33. Krackow KA, Thomas SC, Jones LC: Ligament-tendon fixation: Analysis of a new stitch and comparison with standard techniques. Orthopedics 1988;11:909-917. 34. Gaines RJ, Grabill SE, DeMaio M, Carr D: Patellar tendon repair with suture anchors using a combined suture technique of a Krackow-Bunnell weave. J Orthop Trauma 2009;23:68-71. 35. Page BJ, Stevens TT, Barth KA, et al.: Krackow suture technique effect on patella tendon vascularity: Quantitative-MRI analysis. J Orthopaedic Trauma 2023;37:407-411 36. Capiola D, Re L: Repair of patellar tendon rupture with suture anchors. Arthrosc J Arthroscopic Relat Surg 2007;23:906.e1-906.e4. 37. Ode GE, Piasecki DP, Habet NA, Peindl RD: Cortical button fixation: A better patellar tendon repair? Am J Sports Med 2016;44:2622-2628. 38. Black JC, Ricci WM, Gardner MJ, et al.: Novel augmentation technique for patellar tendon repair improves strength and decreases gap formation: A cadaveric study. Clin Orthop Relat Res 2016;474:2611-2618. 39. Gould HP, Rate WR, Harrell RA, Abbasi P, Fillar AL: Effect of poly-L-lactic acid mesh augmentation on cyclic gap formation in transosseous patellar tendon repair: A biomechanical study. J Knee Surg 2023;36:1224-1229 40. Fukuda A, Nakazora S, Nishimura A, Kato K: Repair of acute patellar tendon rupture using an internal brace technique. Case Rep Orthop 2021;2021:1086625. 41. Sanchez G, Ferrari MB, Sanchez A, et al.: Proximal patellar tendon repair: Internal brace technique with unicortical buttons and suture tape. Arthrosc Tech 2017;6:e491-e497. 42. Ruiz-Alonso S, Lafuente-Merchan M, Ciriza J, Saenz-Del-Burgo L, Pedraz JL: Tendon tissue engineering: Cells, growth factors, scaffolds and production techniques. J Control Release 2021;333:448-486. 43. de Almeida AM, Demange MK, Sobrado MF, Rodrigues MB, Pedrinelli A, Hernandez AJ: Patellar tendon healing with platelet-rich plasma: A prospective randomized controlled trial. Am J Sports Med 2012;40:1282-1288. 44. Barman A, Sinha MK, Sahoo J, et al.: Platelet-rich plasma injection in the treatment of patellar tendinopathy: A systematic review and meta-analysis. Knee Surg Relat Res 2022;34:22. 45. Liddle AD, Rodríguez-Merchán EC: Platelet-rich plasma in the treatment of patellar tendinopathy: A systematic review. Am J Sports Med 2015;43:2583-2590. 46. Zayni R, Thaunat M, Fayard J-M, et al.: Platelet-rich plasma as a treatment for chronic patellar tendinopathy: Comparison of a single versus two consecutive injections. Muscles Ligaments Tendons J 2015;5:92-98. 47. Redler A, Proietti L, Mazza D, et al.: Rupture of the patellar tendon after platelet-rich plasma treatment: A case report. Clin J Sport Med 2020;30:e20-e22. 48. No YJ, Castilho M, Ramaswamy Y, Zreiqat H: Role of biomaterials and controlled architecture on tendon/ligament repair and regeneration. Adv Mater 2020;32:e1904511. 49. Marder RA, Timmerman LA: Primary repair of patellar tendon rupture without augmentation. Am J Sports Med 1999;27:304-307. 50. Bhargava SP, Hynes MC, Dowell JK: Traumatic patella tendon rupture: Early mobilisation following surgical repair. Injury 2004;35:76-79. 51. West JL, Keene JS, Kaplan LD: Early motion after quadriceps and patellar tendon repairs: Outcomes with single-suture augmentation. Am J Sports Med 2008;36:316-323. 52. Bushnell BD, Tennant JN, Rubright JH, Creighton RA: Repair of patellar tendon rupture using suture anchors. J Knee Surg 2008;21:122-129. 53. Ettinger M, Dratzidis A, Hurschler C, et al.: Biomechanical properties of suture anchor repair compared with transosseous sutures in patellar tendon ruptures: A cadaveric study. Am J Sports Med 2013;41:2540-2544.
留言 (0)