
記住我



Distal radius fractures (DRFs) are injuries that considerably affect the well-being of individuals of all ages. They account for 25% of fractures in the pediatric population and 18% of fractures in the elderly.1 According to studies over the past two decades, the incidence of DRFs continues to rise.1 These injuries may be treated surgically or nonsurgically depending on fracture characteristics and patient presentation but require management by a trained health provider to optimize outcomes. Nonsurgical management often involves manipulative reduction and immobilization with frequent follow-up to monitor alignment. Meanwhile, surgical fixation strategies vary but often necessitate open reduction and internal fixation to establish anatomic reduction. The appropriate care for DRFs involves appropriate imaging for diagnosis, access to health providers trained in managing these injuries, and surgical infrastructure for those requiring surgical intervention. Unfortunately, many seeking care for these injuries face difficulties accessing health care or the possibility of financial hardship due to the cost of treatment and time out of work.2 These challenges are especially evident in low- and middle-income countries (low- and middle-income countries) where access to safe and affordable orthopaedic care remains inadequate.3
Malawi is a low-income country in sub-Saharan Africa with an estimated population of 18.6 million with more than half of the population living on less than $1 USD per day. Most Malawians rely on subsistence farming, which can be markedly impaired by musculoskeletal disability.4 Access to trauma care is limited especially for the 84% of the population who lives in rural areas.5,6 Malawi has the world's fourth highest traffic-related mortality per capita and a high incidence of musculoskeletal injuries yet has only 14 orthopaedic surgeons all based in urban centers.7 There are no fracture care services offered in primary care facilities but are provided in secondary and tertiary care facilities. This results in difficulty in accessing fracture care for the majority rural population. In addition, the low ratio of orthopaedic surgeons to the population makes adequate access to surgery for most patients impossible. Orthopaedic clinical officers (OCOs) are nonphysician healthcare workers who provide nonsurgical musculoskeletal trauma care to most patients. In addition, access to tools needed for surgery such as k-wires, external fixators, implants for internal fixation, and radiography is limited.8 This has created a high dependance on donations to acquire tools and implants necessary for care of injured patients.8
In the context of high burden of trauma and limited capacity for surgical treatment, understanding the epidemiology and treatment of DRFs in Malawi is critical to optimize care and resource utilization. The purpose of this study was to describe the epidemiology and management of DRFs presenting to four public hospitals in Malawi.
Methods Study Design and SampleWe reviewed all adult patients with DRFs who had been prospectively enrolled in the Malawi Fracture Care Registry, which included patients with fractures of the appendicular skeleton who presented to four public hospitals in Malawi between September 1st, 2016, and March 31st, 2020. The hospitals included two rural district hospitals, Nkhata Bay Hospital and Mangochi Hospital, and two urban referral hospitals, Kamuzu Central Hospital in Lilongwe and Queen Elizabeth Central Hospital in Blantyre. Data were collected by OCOs and data clerks and underwent regular audits for validity. Quarterly meetings were held at each of the participating sites to review records and perform data verification. Furthermore, regular monitoring, identification of errors, and feedback were used to ensure validity and quality of data. A full description of the Malawi Fracture Care registry has previously been published.9
Data ElementsAll patients aged 18 years or older were eligible for review in our study. For each patient, we analyzed demographic factors such as age, sex, referral status, mechanism of injury, occupation, and highest level of education obtained. Age was analyzed as both a continuous and categorical (20 to 39, 40 to 59, 60+) variable. Referral status indicated whether patients were referred to the hospital of presentation by another health facility or self-referred to the hospital.
We also reviewed information on injury and management characteristics such as number of open fractures, number of patients with multiple fractures, types of surgical procedures, patient disposition, and initial healthcare provider encountered. Fracture descriptions including transverse, oblique, spiral, and comminuted were provided where available based on the primary fracture lines on orthogonal radiographs. For disposition, patients were either treated nonsurgically or sent home, admitted, or referred to a different facility. No deaths were recorded among included patients in our study. Initial healthcare providers included surgical registrars, OCOs, and orthopaedic surgeons.
Variables were compared between patients who presented to district and central hospitals as well as between patients who underwent surgical fixation and those managed nonsurgically. As there are no orthopaedic surgeons at district hospitals, the surgical versus nonsurgical analyses were done only for patients at the central hospitals. Orthopaedic clinical officers at district hospitals were able to perform irrigation and débridement for open injuries but did not perform surgical fixation of fractures. Patients with multiple fractures were also excluded from the analyses comparing surgical and nonsurgical management because we could not determine which fracture was managed surgically based on collected data.
Statistical AnalysisAll analyses were done using R Statistical Software. Individual continuous variables were compared using the Student t-test, and categorical variables were compared using the Chi-squared test. Bivariate and multivariate logistic regression was done to evaluate the association between variables and surgical management. All variables for patients with isolated DRFs underwent bivariate analysis. Notable variables were included in a multivariate regression. Multiple models were trialed by sequential addition with best fit determined by the Akaike Information Criterion and the Bayesian Information Criterion values. Statistical significance was defined as an alpha less than 0.05.
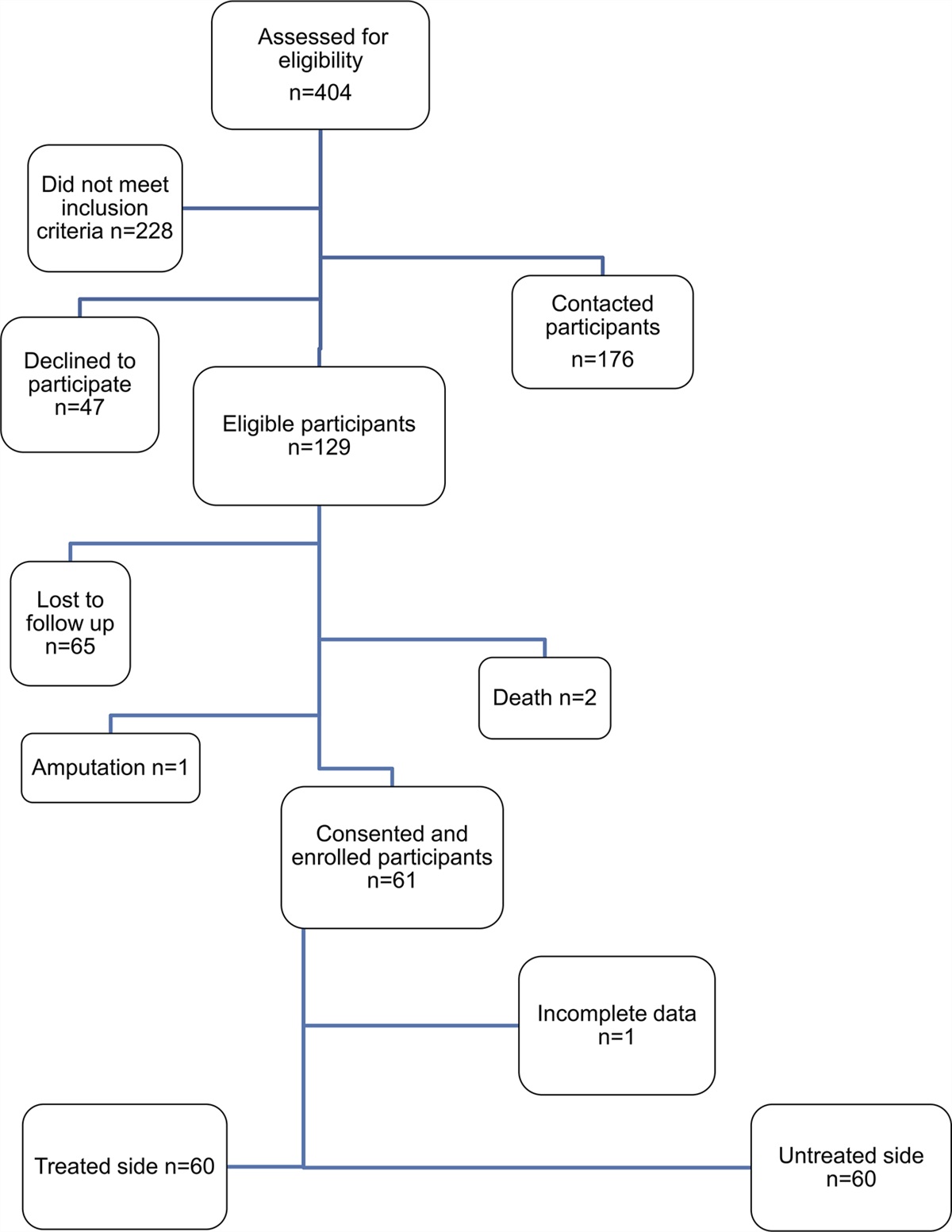
Results DemographicsBetween September 1st, 2016, and March 31st, 2020, there were 9917 adult patients recorded in the registry. Of these, 1.440 (14.5%) sustained an isolated DRF. The average age was 40.9 years (standard deviation 15.1), and the majority were male (n = 888, 62.0%). The most common cause was fall (n = 889, 61.7%) followed by motor vehicle incident (n = 264, 18.3%; Table 1). Patients presenting to district hospitals were more likely to be older, female, farmers, and less educated.
Table 1 - Demographic Variables for Patients with Distal Radius Fractures Demographic Variables DRFs N (%) Central Hospitals (n = 1214, 87.0%) District Hospitals (n = 226, 16.0%) P Age P < 0.01 20-39 718 (53.0%) 617 (54%) 101 (49.0%) 40-59 454 (33.5%) 393 (34%) 61 (29.5%) 60+ 182 (13.4%) 138 (12%) 44 (21.5%) Sex P < 0.01 Male 888 (62.0%) 780 (64.5%) 108 (48.0%) Female 545 (38.0%) 428 (35.5%) 117 (52.0%) Referral P < 0.05 Referred 906 (64.3%) 797 (65.5%) 109 (56.0%) Self-referred 503 (35.7%) 418 (35.5%) 85 (44.0%) Mechanism P < 0.01 Fall 889 (61.7%) 738 (62.0%) 151 (67.5%) Traffic-related 264 (18.3%) 219 (18.5%) 45 (20%) Other 265 (20.0%) 221 (19.5%) 22 (12.5%) Occupation P < 0.01 Farmer 324 (22.5%) 210 (19.0%) 114 (51.0%) Small business 290 (20.1%) 262 (23.5%) 28 (12.5%) Laborer 156 (10.8%) 140 (12.5%) 16 (7.0%) Student 96 (7.1%) 80 (7.0%) 16 (7.0%) Homemaker 92 (6.4%) 73 (6.5%) 19 (8.5%) Other 386 (33.1%) 356 (31.5%) 30 (14%) Education P < 0.01 Less than secondary school level 634 (59.2%) 492 (55.5%) 142 (75.0%) At least secondary school level 437 (40.8%) 390 (44.5%) 47 (25.0%)Seventy-three patients (5.1%) sustained open DRFs which were significantly less compared with fractures in other anatomic locations including tibial shaft fractures (N = 53, 15.0%), distal tibial fractures (N = 102, 13.0%), and foot fractures (N = 42, 10.5%; P < 0.01).
One hundred thirty-five patients (9.4%) with DRFs sustained multiple fractures. The most common associated injuries were distal tibia/fibula fractures (n = 25), supracondylar humerus fractures (n = 23), and ankle fractures (n = 13). Most fractures were extra-articular and either transverse or oblique in orientation. Most of the patients with isolated DRFs were treated nonsurgically (n = 1,285, 89.2%) and sent home after receiving treatment (n = 1,125, 78.1%; Table 2). Most patient underwent closed manipulation of their fractures (n = 974, 67.6%). Only 11 patients (1.1%) required surgical fixation after closed manipulation during their hospital encounter. Hospital admission was significantly associated with both open injuries and sustaining multiple fractures (P < 0.01). Most patients were managed by OCOs (n = 1,370, 95.0%) with only 55 (3.8%) evaluated by a trained orthopaedic surgeon. Patients with open fractures and those sustaining multiple injuries were more likely to be managed at a central hospital.
Table 2 - Injury Characteristics of Distal Radius Fractures Injury Characteristics Distal Radius Fracture N (%) Central Hospitals (n = 1,214, 87.0%) District Hospitals (n = 226, 16.0%) P Open Fracture 73 (5.1%) 65 (5.5%) 8 (3.5%) P = 0.25 Multiple fractures 135 (9.4%) 129 (10.5%) 6 (2.5%) P < 0.01 Fracture location P < 0.01 Extra-articular 1272 (92.8%) 1049 (91.5%) 223 (99.1%) Intraarticular 99 (7.2%) 97 (8.5%) 2 (0.9%) Fracture description P < 0.01 Transverse 688 (57.0%) 514 (52.5%) 174 (78.0%) Oblique 383 (32.0%) 340 (34.5%) 43 (19.0%) Comminuted 72 (6.0%) 72 (7.5%) 2 (1.0%) Spiral 58 (5.0%) 54 (5.5%) 4 (2.0%) Managementa P < 0.01 Surgical 122 (9.5%) 114 (10.5%) 8 (3.5%) Nonsurgical 1183 (90.5%) 971 (89.5%) 212 (96.5%) Disposition P = 0.20 Treated and sent home 1125 (78.0%) 939 (77.5%) 186 (82.5%) Admitted 311 (21.5%) 272 (22.5%) 39 (17.0%) Referred 4 (0.5%) 3 (0.5%) 1 (0.5%) Initial healthcare provider Nonsurgeon providers 1387 (96.0%) 1161 (95.5%) 226 (100.0%) — Orthopaedic surgeons 55 (4.0%) 55 (4.5%) 0 (0.0%) —aManagement variable was analyzed for patient sustaining isolated DRFs. Due to limitations in data collection, we were unable to determine which injuries were managed surgically in patients who sustained multiple fractures.
In total, 122 patients (9.5%) underwent surgical management (Table 3). Surgical capacity at district hospitals is limited because there are no trained orthopaedic surgeons at these locations. Eight patients with sustained open DRFs who presented to a district hospital, however, did undergo formal irrigation and débridement in the operating room. At the central hospital, 114 patients (10.5%) underwent surgical procedures (Table 4). The surgical rate for closed DRFs was 5.7%. Patients had lower odds of surgery if they were evaluated at Queen Elizabeth Hospital, presented after a fall, had less than a secondary level of education, sustained a closed injury, or were initially evaluated by a nonsurgeon provider. Multiple models were trialed by sequential addition with best fit corresponding to the model with all notable bivariate predictors. This demonstrated that hospital of presentation, age, mechanism, provider, fracture comminution, and open nature of fracture all remained notable predictors of surgical intervention.
Table 3 - List of Surgical Procedures and Fracture Descriptions Where Available Fracture Description Irrigation and Débridement N = 57 (47.0%) Open Reduction and Internal Fixation N = 52 (42.5%) Kirschner Wire Fixation N = 8 (6.5%) External Fixation N = 6 (5.0%) Transverse (N = 26) 10 13 2 2 Oblique (N = 25) 13 11 2 Spiral (N = 0) —t — — — Comminuted (N = 20) 6 10 4 1Patients may have undergone multiple procedures.
Our study reviewed the records of 9,917 adult trauma patients presenting to four hospitals in Malawi over a 3.5-year period. We found that 1,440 (14.5%) presented for management of a DRF making it the most common musculoskeletal injury encountered. The average age of an adult patient was 41, and falls followed by motor vehicle incidents were the most common etiologies. Surgery was done on 122 patients (9.5%), mainly in central hospitals. Patients presenting to Queen Elizabeth Hospital, patients presenting after a fall, and patients initially evaluated by an orthopaedic registrar or OCO had lower odds of receiving surgical treatment. Meanwhile, open injuries and comminuted fractures had the greatest odds of receiving surgery.
Distal radius fractures are the most common orthopaedic injury worldwide accounting for between 8% and 18% of fractures.10,11 This is consistent with our results demonstrating that DRFs accounted for 14.5% of all fracture registry entries. The incidence of DRFs typically follows a bimodal distribution with peaks in the pediatric population around the time of maximal skeletal development and again in the elderly population related to osteoporosis.1 DRFs are the third most common fragility fracture after vertebral body and pertrochanteric femur fractures. Studies from Thailand and South Korea have found that 60% and 52% of patients with DRFs had osteoporosis, while Western countries such as Germany, Norway, and Sweden reported a prevalence of 43%, 34%, and 37%, respectively.12–16 In our study sample, 13.5% of patients aged 60 years or older sustained a DRF; however, prevalence of osteoporosis is unknown. Osteoporosis prevalence has been inadequately quantified in sub-Saharan Africa.17 However, the aging population in many African countries, high prevalence of HIV, undernutrition, and socioeconomic inequalities are known risk factors for fragility fractures.18 Additional research is needed to better understand the role of osteoporosis in sub-Saharan communities and guide injury prevention efforts.
The average age in our study was 41 years, compared with studies performed in high-income countries that report an average age for adult DRF at around 67 years old.10,19 In addition, 62% of our patients were male, while most DRFs are seen in women, coinciding with a higher prevalence of osteoporosis.1 High rates of injuries among working age men in sub-Saharan Africa are often related to road traffic incidents; however, the most common etiology in our study was falls among laborers.20 Although our data lack details regarding these falls, many may have been from height and of higher energy. This may also account for the high rate of patients with multiple fractures observed in our cohort. Other possible causes for the lower average age include a younger Malawian population compared with most high-income countries especially in urban areas. Patients presenting to rural district hospitals were markedly older than those presenting to central hospitals. As our study was done at only two of the 27 district hospitals in Malawi and 84% of the Malawian population resides in rural areas, the true average age of patients with DRF in Malawi is likely older than reported.
Overall, 11% of patients presenting to a central hospital underwent surgical management. Only 54% of these procedures, however, were for surgical fixation. Treatment trends nationally are likely markedly lower because most patients present to district hospitals which do not employ full-time orthopaedic surgeons. The rate of surgical fixation is lower than reports from several high-income countries. For example, the United States has rates as high as 32% in patients ages 40 to 64 and 18% in patients 65 or older.21 Sweden has rates of 48% for complete articular fractures and 18% of extra-articular fractures.22 It is important to note that surgical management does depend on a number of factors including fracture characterization and demographic variables. Although we do report on basic fracture descriptions, we do not provide Arbeitsgemeinschaft fur Osteosynthesefragen (AO) classifications, which would be helpful to perform a direct comparison with other countries.
Several injury factors were markedly associated with surgical intervention. For example, 92% of open fractures underwent formal irrigation and débridement. Even in the district hospital setting which lacks orthopaedic surgical coverage, all patients presenting with an open injury underwent irrigation and débridement. We found that 5.0% of DRF in our cohort were open injuries and 47.0% of all procedures were irrigation and débridement. A national Swedish fracture registry found that only 1.2% of DRFs were open.22 The high rate of open fractures in our population also suggests that these injuries were likely the result of high energy mechanisms. Although AO classification was not included in our study, we did find that comminuted fractures had higher odds of surgical fixation. This demonstrates appropriate prioritization of these injuries because they are more likely to have poor outcomes with conservative treatment. In a prospective multicenter study, Wadsten et al23 found that comminution, regardless of exact anatomic location, was associated with a reduction in range of motion and functional outcomes.
Although open injuries were strongly associated with surgical intervention, several variables were associated with nonsurgical treatment. For example, referral status was not associated with surgical fixation. Our study found that most patients presenting to a central hospital were referred from another health facility. These patients, however, were just as likely to receive conservative management and be sent home. This may be due to a lack of resources or training of providers at the referring facilities.24 Unnecessary referrals to central hospitals may lead to additional costs and delays for patients as well as overburdening busy tertiary centers.
There is limited access to orthopaedic surgical care in Malawi with major challenges related to infrastructure and staffing.25 Only 8.7% of all patients underwent surgical intervention with 42.5% of these patients managed with open reduction and internal fixation. Meanwhile, rates of surgery in western countries are as high as 32% in patients aged 40 to 64 and 18% in patients 65 or older.21 Plate fixation is the most common procedure performed for DRFs with up to 55% of surgical patients managed with a volar locking plate.26 Although the rationale for treatment choice was not recorded in this study, treatment decisions likely related to access to implants, availability of surgical infrastructure, and surgeon capacity.27 Aside from these factors, our study found that patients evaluated by nonsurgical providers had markedly lower odds of receiving surgical care. This may be due to the triage of patients with more severe injuries toward surgeons or could be related to different surgical indications between surgeons and nonsurgeon providers. With only 14 orthopaedic surgeons to care for a population of 19 million, most patients will receive care by a nonsurgeon provider. Additional investigations pertaining to management decision for specific injuries, provider knowledge, and effect of treatment on outcomes are needed. This may be used to guide evidence-based decision making in the setting of constrained resources and standardize care among providers.
With limited access to surgery, reliable outpatient follow-up and monitoring are critical to ensure patients receive appropriate care. This involves evaluation by trained providers capable of performing closed manipulation and timely referral to an orthopaedic surgeon if acceptable reduction is lost. This is needed to prevent long-term sequela especially in a younger population within a predominantly agrarian society. Given the challenges with follow-up, there is concern for a high rate of malunions or nonunions, which can create long-term functional issues and economic hardship.28 Posttraumatic arthritis may be as high as 40% for intra-articular fractures managed nonsurgically, and elderly individuals are 50% more likely to have a functional decline.1,29 There must be a simultaneous effort to both improve nonsurgical treatment and increase surgical capacity. Initiatives are currently ongoing to increase the number of trained orthopaedic surgeons because provider shortages have been found to have a major effect on prolonged delays.25 Work must also focus on improving access to follow-up care. This may be done by increasing the
留言 (0)