
記住我



Total knee arthroplasty (TKA) is an effective surgical intervention to relieve pain, restore function, and improve the quality of life of patients with end-stage knee arthritis.1 Despite the popularity and effectiveness of TKA, patient dissatisfaction due to persistent pain and poor function continues to be a concern for approximately 20% of patients after primary TKA.2 Therefore, the optimization of TKA surgical methodology and perioperative protocols to improve patient outcomes remains a key area of research. Controversial topics in TKA optimization such as cruciate-retaining versus posterior stabilized implants, patellar resurfacing versus not resurfacing, press-fit versus cemented implants, and gap balancing versus measured resection approaches are areas of notable debate.3
An emerging topic of interest in the literature is the attenuation of the postoperative inflammatory response (PIR) after TKA. Multiple studies have demonstrated that decreasing postoperative serum and intra-articular levels of inflammatory biomarkers correlates with a reduction in acute postoperative pain after TKA.4–6 In light of this, there is a growing focus on interventions which prevent and modify the PIR to improve TKA outcomes. Strategies such as minimally invasive surgical techniques6 and reduced tourniquet time7 strive to prevent inflammation by reducing surgical trauma, soft-tissue damage, and physiologic stress while inflammatory modifying strategies such as pulsed electromagnetic fields,8 enhanced rehabilitation protocols,9 anti-inflammatory biomaterials,10 and immune-modifying medications 11 focus on mitigating the immune response.
To gauge the effect of anti-inflammatory interventions, researchers have attempted to quantify the degree of postoperative inflammation by using intra-articular and systemic inflammatory biomarkers, clinical inflammatory assessments, and imaging modalities.4,12,13 The natural post-TKA inflammatory biomarker response has been well defined in several observational studies.12,14,15 C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and interleukin-6 (IL-6) are the most common inflammatory biomarkers used in the literature.12 While CRP level and ESR are routinely monitored to screen for prosthetic joint infection after TKA, they are also useful to assess the magnitude of aseptic inflammatory response. CRP is a major acute-phase reactant that is produced in the liver in response to tissue damage, inflammation, infection, and malignancy.12 ESR is a nonspecific hematological test used as an indirect measure of acute-phase reactants.12 IL-6 is produced by monocytes, macrophages, and other cells after antigen activation. IL-6 is also responsible for the hepatic synthesis of CRP.12 These inflammatory markers can be measured systemically in serum or can be analyzed locally by sampling intra-articular fluid.4 Clinical assessments of post-TKA inflammation are less reliable and seldomly standardized. Several techniques for measuring joint swelling and temperature post-TKA have been described, but they lack a unified approach.16,17 Joint imaging is another potential method to quantify post-TKA inflammation; however, assessment of knee joint inflammation using imaging modalities is lacking in the literature.13
Despite the potential effect of the PIR on patient outcomes, inflammation is seldomly considered or investigated when comparing controversial topics in TKA. Therefore, the primary goal of this systematic review was to identify whether interventions which attenuated the PIR as quantified by inflammatory biomarkers, clinical inflammatory assessments, and imaging studies had an effect on postoperative pain and functional outcome measures. The secondary aim was to propose a framework for quantifying the PIR after TKA in future studies by analyzing the trends in inflammatory biomarkers and clinical inflammatory measures.
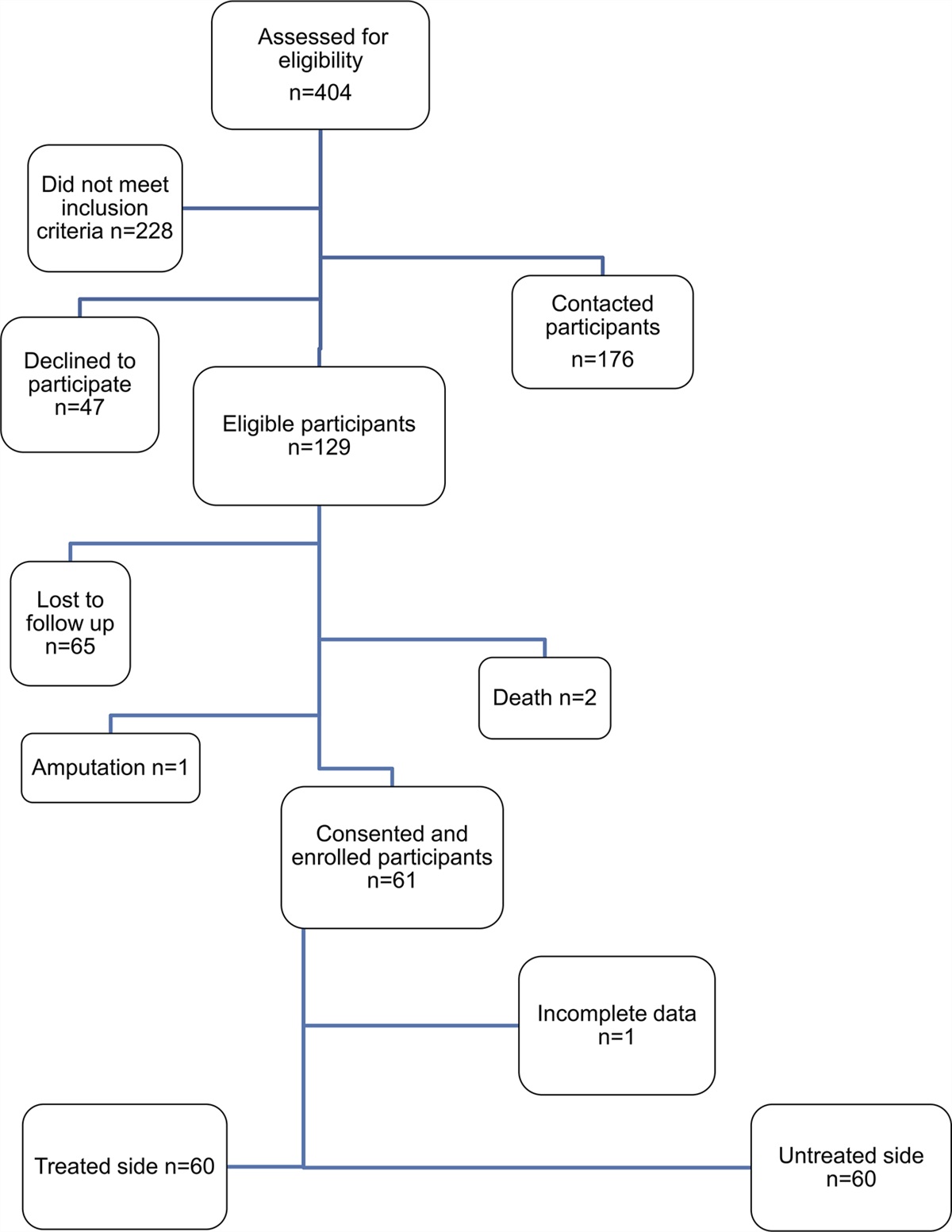
Methods Search StrategyUsing a predetermined search strategy, a systematic literature search of eight major databases and gray literature resources was completed using Medline and Embase (through OVID), Cochrane Library, SPORTDiscus, Web of Science, Scopus, Global Index, and PubMed. The search included studies published between inception and July 2021. The following research terms were used: total knee arthroplasty, total knee replacement, total knee joint replacement, knee joint replacement, synovitis, inflammation, joint inflammation, systemic inflammation, white blood cell count, erythrocyte sedimentation rate, C-reactive protein level, and interleukin 6 level. Studies reporting prospective randomized control trials, primary total knee arthroplasties, inflammatory markers, and presurgical radiographic evidence of osteoarthritis were included. Patient demographics, study interventions, surgical protocols, biomarkers, clinical swelling assessments, and imaging findings were also recorded. Articles were excluded owing to incorrect study design (case reports, systematic reviews), incorrect population studied (animal study, cadaver study), confounding inflammatory conditions (infection, metallosis, or aseptic loosening), administration of glucocorticoids perioperatively, incorrect surgical procedure (revision, bilateral, or unicompartmental arthroplasty), or articles not written in English. The titles and abstracts were screened by two reviewers. If a discrepancy was present, a third reviewer was consulted. Full-text articles were selected and extracted by three reviewers (Figure 1).
 Figure 1: Systematic review search results and study selection summarized in PRISMA flow diagram.18Data Analysis
Figure 1: Systematic review search results and study selection summarized in PRISMA flow diagram.18Data Analysis
The following patient demographic variables were collected: sex, age, body mass index (BMI), and study intervention. The following preoperative and postoperative variables were collected: surgical approach, anesthesia protocol, medication protocol, additional perioperative interventions, implant type, inflammatory biomarkers, clinical assessments of inflammation, imaging, and outcome measure scores. CRP, IL-6, ESR, and knee skin temperature data were extracted and displayed graphically for both the control and treatment arms for each study.
ResultsA total of 4,917 abstracts and titles were screened by two reviewers, and 122 full-text articles were assessed for eligibility (Figure 1). Eligible studies were reviewed, and details were reported using the 2020 PRISMA guidelines.18 A total of 14 studies were included.19–32 Risk of bias was assessed by two reviewers (Supplemental Table 1, https://links.lww.com/JG9/A330).
Patient Demographics and InterventionsThe study cohorts included in the analysis ranged from 30 to 275 participants, with a mean study size of 112.7 participants (SD = 80.08). Across the studies reviewed, 72% of participants (SD = 10.25) identified as female, the mean age was 67.25 (SD = 2.75) years, and the mean BMI was 27.52 (SD = 3.32). The interventions examined in these studies included antifibrinolytics, surgical approaches, perioperative anti-inflammatory agents, and materials. The risk of bias across all the studies was low (Supplemental Table 1, https://links.lww.com/JG9/A330).
Surgical ProtocolThe medial parapatellar approach with a measured resection technique using standard instrumentation was the most commonly used surgical approach (78.5%). Alternative approaches included midvastus arthrotomy and mini-midvastus approach. An even split was noted between studies on the use of intra-articular drainage (50%) and tourniquets (46%). General anesthesia was the most common anesthetic approach (29%). Alternative approaches used a combination of regional and neuraxial anesthesia (21%), general and neuraxial anesthesia (14%), and general or neuraxial anesthesia (7%), whereas the remaining studies did not specify the anesthetic approach (29%). Protocols for antibiotics, local anesthetics, NSAIDs, narcotics, antifibrinolytics, and anticoagulants vary widely. Most of the studies (64%) described using a ‘standardized’ rehabilitation protocol, some of which involved mechanical antithrombotic exercises (36%) and cold therapy (21%). The participants began mobilizing between POD0 and POD2 in all studies that reported this metric. Posterior stabilized implants were the most frequently used (78.5%), followed by cruciate-retaining implants (14.2%), with no reported noncemented implants (Supplemental Table 2, https://links.lww.com/JG9/A331).
Biomarkers, Clinical Assessments, and Outcome MeasuresSerum inflammatory biomarkers were reported in 86% of included studies. Of the biomarkers, CRP was the most frequently assessed (64% of studies), followed by IL-6 (57%) and ESR (43%). All biomarkers examined were obtained from serum, except for Memtsoudis et al,27 who examined the intra-articular levels of IL-6 and TNF-α. The most commonly reported clinical assessments of inflammation were circumferential girth measurement (43%) and knee surface temperature (KST) (29%). No studies have reported the use of imaging modalities to assess inflammation. Pain and functional outcome measures were assessed primarily using standardized tools, such as the visual analog scale (57% of studies), Knee Society Score (29% of studies), and Hospital for Special Surgery score (14% of studies). Range of motion (ROM) was also reported (36% of studies) (Supplemental Table 3, https://links.lww.com/JG9/A332).
Trends in C-Reactive Protein, Interleukin-6, and Erythrocyte Sedimentation RateThe mean CRP value peaked on POD2 and returned to baseline levels on POD28. Kayani et al 22 reported the highest maximum mean CRP at 170.1 mg/L on POD2. Significant differences in CRP levels between the control and treatment groups were found in four studies 22,29,30,32 (Figure 2). The mean IL-6 values peaked on POD1 and returned to baseline in most studies on POD7. Lin et al 25 reported the highest IL-6 level of 375 pg/mL on POD1. Significant differences in IL-6 levels between the control and treatment groups were found in five studies 22,25,29,30,32 (Figure 3). The mean ESR values peaked on POD7 and did not return to baseline in any of the studies. Most studies observed a marked reduction in ESR, with levels close to baseline by POD28. Wang et al and Xu et al reported the same maximum ESR mean of 95 mm/hr on POD1 and POD7, respectively.29,32 Significant differences in ESR between the control and treatment groups were found in three studies 22,29,32 (Figure 4).
 Figure 2:
Figure 2: A, Graph showing mean serum CRP levels in the control arms of the included studies. B, Graph showing mean serum CRP levels in the treatment arms of the included studies. C, Graph showing mean serum CRP compared between control and treatment groups of the included studies. PO = postoperative, POD = postoperative day, H = hours, CRP = C-reactive protein
 Figure 3:
Figure 3: A, Graph showing mean serum IL-6 levels in the control arms of the included studies. B, Graph showing mean serum IL-6 levels in the treatment arms of the included studies. C, Graph showing mean serum IL-6 compared between control and treatment groups of the included studies. PO = postoperative, POD = postoperative day, H = hours, IL-6 = interleukin 6
 Figure 4:
Figure 4: A, Graph showing mean ESR in the control arms of the included studies. B, Graph showing mean ESR in the treatment arms of the included studies. C, Graph showing mean ESR compared between control and treatment groups of the included studies. PO = postoperative, POD = postoperative day, H = hours, ESR = erythrocyte sedimentation rate
Trends in Knee Surface TemperatureThe KST was measured in four studies (29%), all of which used a digital infrared surface thermometer. In general, KST peaked from POD1 to POD3, with a variable return to baseline. Kayani et al22 and Lin et al25 reported a return of KST to baseline at POD28 and 6 months postoperatively, respectively, whereas Tanavalee et al28 and Xu et al32 reported no return to baseline temperatures at their terminal measurements at 26 months and 6 weeks postoperatively, respectively (Figure 5). Lin et al 25 and Xu et al 32 reported a significant difference between the control and treatment groups in KST (Figure 5).
 Figure 5:
Figure 5: A Graph showing mean KST in the control arms of the included studies. BGraph showing mean KST of the treatment arms of the included studies. C, Graph showing mean KST compared between control and treatment groups of the included studies. PO = postoperative, POD = postoperative day, H = hours, wk = weeks, KST = knee skin temperature
DiscussionThe major finding of this systematic review was that most of the studies 21,25,29,30,32 which demonstrated a statistically significant PIR attenuation, as quantified by inflammatory biomarkers and clinical inflammatory assessments, found improvement in pain scores and functional outcome measurements (Supplemental Table 3, https://links.lww.com/JG9/A332). Whereas studies that showed no notable difference in inflammatory biomarkers or clinical inflammatory assessments 20,23,28 observed no improvement in clinical outcome measures. An exception was Memtsoudis et al,26,27 who found an improvement in visual analog scale scores in their treatment group despite no difference in CRP, IL-6, TNF-α, thigh circumference, or physical therapy milestones. The interventions that successfully attenuated the PIR after TKA were tranexamic acid, reduced tourniquet time, and celecoxib (Supplemental Table 3, https://links.lww.com/JG9/A332) while the bioabsorbable bone agent, triclosan-coated suture, and synovectomy interventions had no effect on the PIR (Supplemental Table 3, https://links.lww.com/JG9/A332). The association found in this review between inflammatory biomarkers, clinical inflammatory assessments, and outcome measures concurs with findings in the literature. Si et al4 found a direct correlation between acute postoperative pain and serum CRP and IL-6 levels. Furthermore, Holm et al33 found a relationship between knee swelling during the initial post-TKA recovery period and loss of knee extension strength.
Given the association between PIR attenuation and improved early pain and functional outcomes, it is reasonable to hypothesize that TKA approaches, techniques, and perioperative protocols which prevent and mitigate the PIR will lead to enhanced patient outcomes. However, caution must be taken when examining inflammation in isolation. It is possible that approaches or techniques which increase the PIR may improve other variables such as alignment or stability and ultimately lead to better long-term patient outcomes.34 Indeed, it remains unclear whether PIR attenuation plays a role in long-term outcomes at all.6,35 Within our review, few articles examined long-term outcomes such as anterior knee pain, functional recovery, patient satisfaction, and revision surgery rates (Supplemental Table 3, https://links.lww.com/JG9/A332) Of our included studies, only Adravanti et al19 assessed for long-term pain outcomes; they found that every subject in their control group who reported pain in the first 2 months postoperatively also reported of pain at a 3-year follow-up. Whereas their treatment group who experienced reduced knee joint swelling in the postoperative period only had one patient complain of pain at the 3-year mark. In the literature, Fontalis et al6 examined the effect of local PIR attenuation on long-term outcomes at the 2-year mark in their work involving minimally invasive surgical techniques. They found no relationship between early PIR attenuation and passive range of motion or quality of life scores at 2 years postoperatively. Therefore, both this study and the literature are inconclusive on the long-term benefit of transient early PIR attenuation.
Despite these uncertainties, given the link to early TKA recovery,4–6 the PIR may be an important variable for future research when determining superiority in controversial topics within TKA such as patellar resurfacing versus not resurfacing, cruciate-retaining versus posterior stabilized, and robotic vs standard jig.3 As PIR attenuation is investigated within these contexts, additional clarity on its importance and role in long-term outcomes may be elucidated.
The secondary aim of this review was to investigate current approaches to PIR quantification after TKA. At present, there is no consensus on an ideal framework for PIR quantification, and significant heterogeneity to quantification approaches is apparent in the literature (Supplemental Table 3, https://links.lww.com/JG9/A332). Approaches to PIR quantification can be subdivided into inflammatory biomarker measurement, clinical inflammatory assessments, and imaging studies.
When quantifying the PIR using inflammatory biomarkers, researchers must consider which biomarkers to use, whether they will take intra-articular or serum measurements, and what time points to collect biomarker measurements. In our review, CRP, IL-6, and ESR were the most commonly used inflammatory biomarkers. CRP and IL-6 are acute-phase reactants that increase rapidly and quickly return to baseline during the initial TKA postoperative period, whereas ESR exhibits prolonged temporal changes.12 Based on our results, IL-6 and CRP seemed to be good indicators of the PIR because significant differences in these biomarkers were mirrored by corresponding changes in clinical inflammatory assessments and improved clinical outcomes (Supplemental Table 3, https://links.lww.com/JG9/A332). ESR was a less sensitive measure of the PIR because only three studies noticed a notable difference between treatment groups using this marker.22,29,32 Several alternative biomarkers have been investigated in the context of measuring the PIR after TKA. Indeed, Cao et al21 found that attenuating the levels of serum tumor necrosis factor alpha (TNF-α), C-C motif chemokine ligand 2 (CCL2), prostaglandin E2, superoxide dismutase 1, and myoglobin resulted in significant improvements in functional outcomes in their study (Supplemental Table 3, https://links.lww.com/JG9/A332). In the literature, Langkilde et al35 found a relationship between IL-10 and decreased long-term functional outcomes. Therefore, although our findings suggest IL-6 and CRP are efficacious in PIR quantification, additional research is warranted to explore the utility of alternative inflammatory biomarkers.
Another consideration is the decision to measure inflammatory biomarkers from serum or intra-articularly. Ugras et al argued that the local inflammatory response is more important than the systemic inflammatory response. In their study, there was a direct correlation between increased intra-articular IL-6 levels and slower post-TKA recovery. They found no correlation between serum inflammatory biomarkers and post-TKA recovery.5 By contrast, within this review, several studies have demonstrated a significant difference in serum inflammatory biomarkers, which led to improvements in clinical outcome measures (Supplemental Table 3, https://links.lww.com/JG9/A332). Thus, both intra-articular and serum measurements of inflammatory biomarkers appear adequate to assess the PIR after TKA. It remains unclear whether local or systemic responses are more important. One disadvantage of intra-articular collection is the ethical concerns of preoperative measurements.6 Preoperative baseline measurements of inflammation are crucial to contextualize changes in the PIR because patients may have notable differences in preoperative inflammation based on disease progression.12,14,15 Furthermore, serum collection may be more practical for serial collection for both patients and investigators.
Sequential measurement of inflammatory biomarkers is required to interpret the entire PIR. In our review, there was notable heterogeneity in the postoperative time point selection for inflammatory biomarker measurements between our included studies. This time point discrepancy makes comparing trends in inflammatory biomarkers within this review challenging. Overall, the mean CRP values peaked on POD2 and returned to baseline approximately 4 weeks postoperatively (Figure 2). This aligns well with the literature, as Park et al15 demonstrated a mean CRP max on POD2 and a return to baseline on POD19. Maniar et al14 found mean CRP max at POD2 but did not return to baseline until 1 month postoperatively. Honsawek et al12 reported a mean CRP max on POD1 with a similar return to baseline on POD14. Therefore, CRP in the immediate postoperative period seems to reach its peak between POD1 and 3, with a return to baseline between 2 weeks and 1 month postoperatively. The mean IL-6 level reached its maximum on POD1 and returned to baseline on POD7 (Figure 3). Maniar et al14 observed a mean IL-6 peak value at 12 hours postoperatively, with a return to baseline on POD14. Honsawek et al12 demonstrated a mean IL-6 peak on POD1 with a return to baseline on POD14. Therefore, IL-6 reaches peak postoperative levels somewhere between 12 hours postoperatively and POD2 with a return to baseline between POD7 and POD14. Despite this trend, in our review, only Memtsoudis et al26 measured IL-6 levels at the 12-hour postoperative time point (Figure 3). It is possible that the remaining studies did not capture peak IL-6 concentrations because they lacked a measurement time point in the initial 12-hour postoperative-POD1 period. Mean ESR levels peaked at POD7 and were markedly reduced by POD28 but did not return to baseline levels in any study. Honsawek et al12 reported the mean ESR max on POD14, which returned to baseline at 26 weeks postoperatively. Park et al15 described the mean ESR max at POD5 and return to baseline at 3 weeks postoperatively. In this review, the study by Tanavalee et al28 was the only one that extended postoperative ESR measurements to 26 weeks; however, no return to baseline levels was observed (Figure 4). Generally, ESR seems to peak between 1 and 2 weeks postoperatively, and it remains inconclusive when a return to baseline should be expected. Despite heterogeneity in study design, biomarker measurement time points, and intervention type, in general, the trends in CRP, IL-6, and ESR (Figures 2–4) found in this review were consistent with the trends established in the literature. It can be inferred that the trends of these inflammatory biomarkers after primary TKA in patients with OA are universal and reproducible. The ideal time points for sequential measurements of inflammatory, however, remain unknown.
When determining the optimal biomarker measurement time points, the stimulus-response relationship between inflammatory biomarkers and clinical outcomes is a crucial consideration. At this time, it is unclear whether attenuating the peak biomarker values, average biomarker values, or biomarker values at a specific time point during the PIR is most important in improving clinical outcomes. In addition, each inflammatory biomarker exhibits a unique trend after TKA (Figures 2–4). Based on our findings, we suggest measurements should at minimum be obtained preoperatively to generate a baseline, an expected peak value, and when values are expected to return to baseline. For instance, CRP should be measured preoperatively, between POD1 and POD2 to capture the peak value, and at its anticipated return to baseline ∼ POD28 (Figure 2). IL-6 should be measured preoperatively, between 12 hours postoperatively and POD1 for the peak value, and ∼POD14 to capture the anticipated return to baseline (Figure 3). Finally, ESR may be a less reliable biomarker to use because there is no established consensus on an expected return-to-baseline time line after TKA (Figure 4). Additional measurement time points between baseline and return to baseline measurements may be beneficial; however, the optimal number and specific timing remain uncertain given the current data.
Approaches to clinical inflammatory assessments to quantify the PIR vary widely among researchers. Adravanti et al19 used the Soderberg scale, a system that involves several predetermined girth measurements of the lower extremities in relation to the knee joint line.36 Wang et al29 and Xie et al30 measured knee circumference at the poles of the patella (Supplemental Table 3, https://links.lww.com/JG9/A332). Cao et al21 and Memtsoudis et al27 measured thigh circumference; however, Cao et al21 measured thigh circumference at a point 10 cm above the patella while Memtsoudis et al27 measured thigh circumference at the midpoint between the patella and anterior-superior iliac spine (Supplemental Table 3, https://links.lww.com/JG9/A332). Lachiewicz et al24 evaluated the presence of effusion using subjective surgeon assessments (Supplemental Table 3, https://links.lww.com/JG9/A332). Evidently, there is a lack of a standardized approach for measuring swelling both subjectively and using circumferential girth measurements.
The KST is a more uniform quantitative clinical inflammatory measure. In this review, four studies (29%) measured the KST after TKA. All studies used a digital infrared surface thermometer to measure the skin temperature. The general trend demonstrated a peak knee skin temperature between POD1 and POD3. The return to baseline diverged across studies (Figure 5). Kayani et al22 and Lin et al25 reported a return of KST to baseline at POD28 and 6 months postoperatively, respectively, whereas Tanavalee et al28 and Xu et al32 did not observe a return to baseline KST at their terminal measurements at 26 weeks and 6 weeks postoperatively, respectively (Figure 5). This is consistent with the established literature, as Haidar et al17 found that KST peaks at POD3 and returns to baseline over months. Mehra et al37 found peak KST at POD5-7 with a return to baseline in their study at 18 weeks postoperatively. Overall, KST seemed to peak on POD3-7 with a prolonged return to baseline over weeks to months.
No study included in this review used imaging to measure the PIR (Supplemental Table 3, https://links.lww.com/JG9/A332). Yet, such imaging techniques have been reported in the literature. Yau et al38 argued that MRI is the most accurate noninvasive method for detecting knee effusion after TKA. However, the authors noted that MRI is typically reserved for assessing complications such as infection, joint loosening, wear, and malalignment. Furthermore, it would likely be cost-prohibitive and impractical to include MRI in larger studies as well as metal suppression protocols. To the best of our knowledge, no study has used MRI to assess normal PIR to TKA. Bioelectrical impedance spectroscopy and 3D scanning modalities are emerging technologies that may provide valuable insights into the inflammatory response to TKA.39 Imaging modalities used in combination with inflammatory biomarkers and clinical assessments may provide a more comprehensive picture of post-TKA inflammatory response.
This study had several limitations. First, the variety of study surgical protocols, interventions, medications, and rehabilitation protocols makes the comparison of the post-TKA inflammatory state between studies challenging. Each of these variables may directly influence the levels of inflammation; however, given the sparsity of the literature, it was not possible to control for these variables. A similar challenge was found in the heterogeneity of inflammatory biomarker time point selection between studies. The lack of consistency between time points prevented our ability to statistically compare biomarker responses in this study. Finally, there were varying levels of evidence and quality of reporting between studies, which is inherent to systematic reviews; however, this prevents definitive conclusions.
ConclusionThe local and systemic PIR after TKA may be a key metric in determining approach superiority within controversial topics in the TKA literature. This systematic review demonstrated that attenuation of the PIR, as quantified by inflammatory biomarkers and clinical inflammatory assessments, strongly correlated with the improvement of objective clinical outcomes. While there seems to be an association with PIR attenuation and early pain and functional outcomes, additional research is required to determine the effect of PIR attenuation on long-term TKA patient outcomes. We have found that IL-6 and CRP are efficacious in the quantification of PIR. Intra-articular and serum measurement of these biomarkers are both acceptable methods of collection. The ideal sequential measurements of these time points are unclear, but we suggest minimum CRP to be measured preoperatively, between POD1 and POD2, and ∼POD28 while IL-6 should be measured preoperatively, between 12 hours postoperatively and POD1, and on ∼POD14. Clinical inflammatory assessments such as KST and imaging may be useful adjuncts to inflammatory biomarkers in quantifying the PIR, but additional investigation is needed.
References 1. Gao J, Xing D, Dong S, Lin J: The primary total knee arthroplasty: A global analysis. J Orthop Surg Res 2020;15:1-12. 2. Gunaratne R, Pratt DN, Banda J, Fick DP, Khan RJ, Robertson BW: Patient dissatisfaction following total knee arthroplasty: A systematic review of the literature. The J Arthroplasty 2017;32:3854-3860. 3. van der Merwe JM, Mastel MS: Controversial topics in total knee arthroplasty: A 5-year update (part 1). J Am Acad Orthop Surgeons Glob Res Rev 2020;4:e1900047. 4. Si HB, Yang TM, Zeng Y, et al.: Correlations between inflammatory cytokines, muscle damage markers and acute postoperative pain following primary total knee arthroplasty. BMC Musculoskelet Disord 2017;18:265-269. 5. Ugraş AA, Kural C, Kural A, Demirez F, Koldas M, Cetinus E: Which is more important after total knee arthroplasty: Local inflammatory response or systemic inflammatory response? The Knee 2011;18:113-116. 6. Fontalis A, Kayani B, Asokan A, et al.: Inflammatory response in robotic-arm-assisted versus conventional jig-based TKA and the correlation with early functional outcomes: Results of a prospective randomized controlled trial. The J Bone joint Surg Am Volume 2022;104:1905-1914. 7. Tsunoda K, Sonohata M, Kugisaki H, et al.: The effect of air tourniquet on interleukin-6 levels in total knee arthroplasty. Open Orthops J 2017;11:20-28. 8. Moretti B, Notarnicola A, Moretti L, et al.: I-ONE therapy in patients undergoing total knee arthroplasty: A prospective, randomized and controlled study. BMC Musculoskelet Disord 2012;13:88-89. 9. Kim S, Hsu FC, Groban L, Williamson J, Messier S: A pilot study of aquatic prehabilitation in adults with knee osteoarthritis undergoing total knee arthroplasty - short term outcome. BMC Musculoskelet Disord 2021;22:1-11. 10. Wilairatana V, Sinlapavilawan P, Honsawek S, Limpaphayom N: Alteration of inflammatory cytokine production in primary total knee arthroplasty using antibiotic-loaded bone cement. J Orthops Traumatol 2017;18:51-57. 11. Yu Y, Lin H, Wu Z, Xu P, Lei Z: Perioperative combined administration of tranexamic acid and dexamethasone in total knee arthroplasty-benefit versus harm? Medicine 2019;98:e15852. 12. Honsawek S, Deepaisarnsakul B, Tanavalee A, et al.: Relationship of serum IL-6, C-reactive protein, erythrocyte sedimentation rate, and knee skin temperature after total knee arthroplasty: A prospective study. Int Orthops 2011;35:31-35. 13. Creteur V, De Angelis R, Absil J, Kyriakidis T, Madani A: Sonographic and radiographic evaluation of the extensor tendons in early postoperative period after total knee arthroplasty. Skeletal Radiol 2021;50:485-494. 14. Maniar RN, Navaneedhan G, Ranvir S, Maniar AR, Dhiman A, Agrawal A: What is the normal trajectory of interleukin-6 and C-reactive protein in the hours and days immediately after TKA? Clin Orthop Relat Res 2019;477:41-46. 15. Park KK, Kim TK, Chang CB, Yoon SW, Park KU: Normative temporal values of CRP and ESR in unilateral and staged bilateral TKA. Clin Orthop Relat Res 2008;466:179-188. 16. Jakobsen TL, Christensen M, Christensen SS, Olsen M, Bandholm T: Reliability of knee joint range of motion and circumference measurements after total knee arthroplasty: Does tester experience matter? Physiother Res Int J researchers clinicians Phys Ther 2010;15:126-134. 17. Haidar SG, Charity RM, Bassi RS, Nicolai P, Singh BK: Knee skin temperature following uncomplicated total knee replacement. The Knee 2006;13:422-426. 18. Page MJ, McKenzie JE, Bossuyt PM, et al.: The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int J Surg 2021;88:105906. 19. Adravanti P, Nicoletti S, Setti S, Ampollini A, De Girolamo L: Effect of pulsed electromagnetic field therapy in patients undergoing total knee arthroplasty: A randomised controlled trial. Int Orthop 2014;38:397-403. 20. Cao G, Xie J, Huang Z, et al.: Efficacy and safety of multiple boluses of oral versus intravenous tranexamic acid at reducing blood loss after primary total knee arthroplasty without a tourniquet: A prospective randomized clinical trial. Thromb Res 2018;171:68-73. 21. Cao Q, Wu Q, Liu Y, et al.: Effects of tourniquet application on faster recovery after surgery and ischemia-reperfusion post–total knee arthroplasty, cementation through closure versus full-course and nontourniquet group. J Knee Surg 2022;35:1577-1586. 22. Kayani B, Tahmassebi J, Ayuob A, Konan S, Oussedik S, Haddad FS: A prospective randomized controlled trial comparing the systemic inflammatory response in conventional jig-based total knee arthroplasty versus robotic-arm assisted total knee arthroplasty. bone joint J 2021;103-B:113-122. 23. Kim JK, Ro DH, Han SM, Lee MC, Han HS: Efficacy and safety of bioabsorbable bone hemostatic agent in total knee arthroplasty:
留言 (0)