
記住我



Fractures involving the ankle joint are common and span a wide spectrum of morphologies, ranging from low-energy unimalleolar ankle fractures to high-energy pilon fractures. The initial management of these injuries is dictated by patient characteristics, fracture morphology, and soft tissue condition. Although most stable, closed fractures can be successfully immobilized in a splint after satisfactory reduction, external fixation remains an integral temporizing treatment option for unstable fractures with a compromised soft tissue envelope.
Staged management with spanning external fixation (ex-fix) is the standard of care for most unstable tibial pilon fractures.1–6 Temporizing external fixation of pilon fractures allows for rigid maintenance of appropriate length, alignment, and rotation with minimal iatrogenic trauma to the soft tissue envelope. Once soft tissue swelling, blisters, and any open wounds have healed, performing open reduction and internal fixation poses a lower risk for soft tissue complications.7,8 Some authors are advocating for definitive management with hybrid ex-fix with limited internal fixation in select patients who are poor surgical candidates or with compromised soft tissue envelope.9–11
Temporizing ex-fix is becoming increasingly used for ankle and talar fracture dislocations where there is concern for loss of reduction. Previous studies found that up to 50% of ankle fracture dislocations immobilized with a plaster splint may require rereduction.12,13 Splints are often applied when the extremity is markedly swollen and may loosen as swelling dissipates.14 Loss of reduction has been associated with worsening pain, increased soft tissue complications, osteochondral lesions, and increased time to definitive fixation.12 These factors may contribute to the threefold increase in major complications seen in ankle fracture dislocations compared with simple ankle fractures.15
Although ankle-spanning ex-fix is a relatively low-risk procedure, poor technique and reduction can result in soft tissue complications, pin tract infections, and pin loosening and may necessitate revision application of the external fixator. Younger orthopaedic surgeons are often the ones applying the external fixator, and they might have less experience in the procedure. This population and the general orthopaedic community can benefit from research outlining ways to help prevent external fixator failure. Despite the extensive use of ankle-spanning external fixators, there is still a lack of research investigating the specific factors contributing to revision of external fixation after ankle and pilon fractures. The goal of this study was to examine radiographic and surgical factors associated with the need for revision ankle-spanning external fixation application. Our population includes mostly underserved populations in a community level I academic trauma center. The primary outcome measure was revision of external fixation within 30 days. To our knowledge, this is the first study to examine the radiographic risk factors for revision of an ankle-spanning external fixator. We hypothesize that poor initial reduction based on eccentric positioning of the talus beneath the tibia and lack of a forefoot pin would be associated with an increased rate of revision external fixation application.
MethodsIRB approval was obtained for this study. A retrospective chart review was conducted of all distal tibial, malleolar, and talar fractures and dislocations (OTA/AO 43A-C, 44A-C) treated during the index procedure with external fixation using a case report query for all cases including “application of external fixation device, lower extremity” during the years of 2019 to 2023.16 Exclusion criteria included external fixation for malunion, deformity, or infection management; configuration other than ankle-spanning external fixator; inadequate intraoperative fluoroscopic imaging; skeletal immaturity; and patients lost to follow-up within 30 days.
Patient charts were reviewed for patient demographics, injury characteristics, and surgical details. Injury radiographs were reviewed for fracture classification. Fluoroscopic imaging was reviewed for construct technique and intraoperative measurements. Postoperative progress notes, surgical notes, clinic notes, and emergency department notes were reviewed for instances of revision of the external fixator within 30 days of placement.
Surgical TechniqueThe following describes the surgical technique used for included cases. The patient was brought to the operating room and placed supine. Preoperative antibiotics were administered within 30 minutes of incision time. General anesthesia was given by the Anesthesia Department. The surgical lower extremity was then prepped and draped in the usual sterile way. Two 5-mm Schanz pins were placed into the anteromedial aspect of the tibia outside of the zone of fracture. One or two centrally threaded 6-mm Schanz pin(s) were placed from medial to lateral in the calcaneus. The addition of a first metatarsal Schanz was placed per the discretion of the surgeon. All pins were placed within their respective safe zones. The Synthes external fixation pin-bar clamps were then applied in a delta frame fashion. Traction and reduction were done. Once satisfied with reduction, final tightening was done.
During final radiographs, the ankle was placed in neutral dorsiflexion to obtain AP, mortise, and lateral views. The perfect lateral view was defined based on a true lateral of the talar dome such that the medial and lateral aspects of the talar dome were superimposed. Sterile dressings were applied, and the patient was awoken from anesthesia and brought the recovery unit. The patients were then admitted postoperatively and made non–weight bearing to the surgical lower extremity. A postoperative CT scan of the ankle was done. Daily rounds with clinical checks were done daily when the patient was in the hospital. After discharge from the hospital, clinic follow-up was scheduled for 2 weeks postoperatively or sooner if their wounds required closer monitoring.
Fluoroscopic MeasurementsAll radiographic measures for analysis were done by a single reviewer, blinded to whether the patient underwent ex-fix revision. Injury radiographs were reviewed for fracture and/or dislocation classification. Posterior malleolar size was measured on the postoperative CT scan. The talocrural angle and the talar tilt were measured on the intraoperative mortise view. The position of the talus beneath the distal tibial articular surface on the lateral view was determined by dividing the distal tibia into thirds, as described in the article by Cosgrove et al.17 The apex of the perfect lateral of the talar dome was then identified with a single point. A perpendicular line from this point to the line across the lateral distal tibia was then drawn. The positioning of the apex of the talar dome was then determined based on whether this line fell in the anterior, middle, or posterior thirds of the distal tibia. A good reduction was defined as a talus reduced within the middle third of the distal tibia (Figure 1). A poor reduction was defined as either anterior or posterior third positioning of the talus beneath the distal tibia (Figure 2).
 Figure 1: Radiograph showing an example of a good intraoperative reduction of the ankle joint. A true lateral of the talar dome is obtained, and the distal tibia is divided into anterior (A) middle (M), and posterior (P) thirds, similar to the method described by Cosgrove et al.17 The apex of the true lateral of the talar dome is identified (blue dot), and a perpendicular line is drawn from this point to the AP tibial line.
Figure 1: Radiograph showing an example of a good intraoperative reduction of the ankle joint. A true lateral of the talar dome is obtained, and the distal tibia is divided into anterior (A) middle (M), and posterior (P) thirds, similar to the method described by Cosgrove et al.17 The apex of the true lateral of the talar dome is identified (blue dot), and a perpendicular line is drawn from this point to the AP tibial line. Figure 2: Radiograph showing an example of a poor intraoperative reduction of the ankle joint. A true lateral of the talar dome is obtained, and the distal tibia is divided into anterior (A) middle (M), and posterior (P) thirds similar to the method described by Cosgrove et al.17 The apex of the true lateral of the talar dome (blue dot) falls in the posterior third of the AP tibial line. This patient ultimately required revision of their external fixator.Revisions
Figure 2: Radiograph showing an example of a poor intraoperative reduction of the ankle joint. A true lateral of the talar dome is obtained, and the distal tibia is divided into anterior (A) middle (M), and posterior (P) thirds similar to the method described by Cosgrove et al.17 The apex of the true lateral of the talar dome (blue dot) falls in the posterior third of the AP tibial line. This patient ultimately required revision of their external fixator.Revisions
A revision of the external fixator was defined as any formal operation or any adjustment on the hospital floor, clinic, or emergency department. If the patient returned to the operating room for management of a wound or other reason and the external fixator was temporarily loosened and reapplied, this was not counted as a revision. A revision event required a specific indication, which was recorded. Surgical and other clinical notes were reviewed for the method of revision and timing from the index procedure.
Statistical AnalysisDescriptive statistics were used to report all demographic and surgical factors in each cohort. Chi-squared tests were used to assess for notable differences between the revised and nonrevised cohorts. Univariate logistic regression analyses were done to assess the risk of revision for each variable. All variables were then included in a single multivariate logistic regression model to identify independent risk factors for revision after ex-fix placement. Statistical significance was defined as P < 0.050. All analyses were done using STATA (version 16.1; StataCorp).
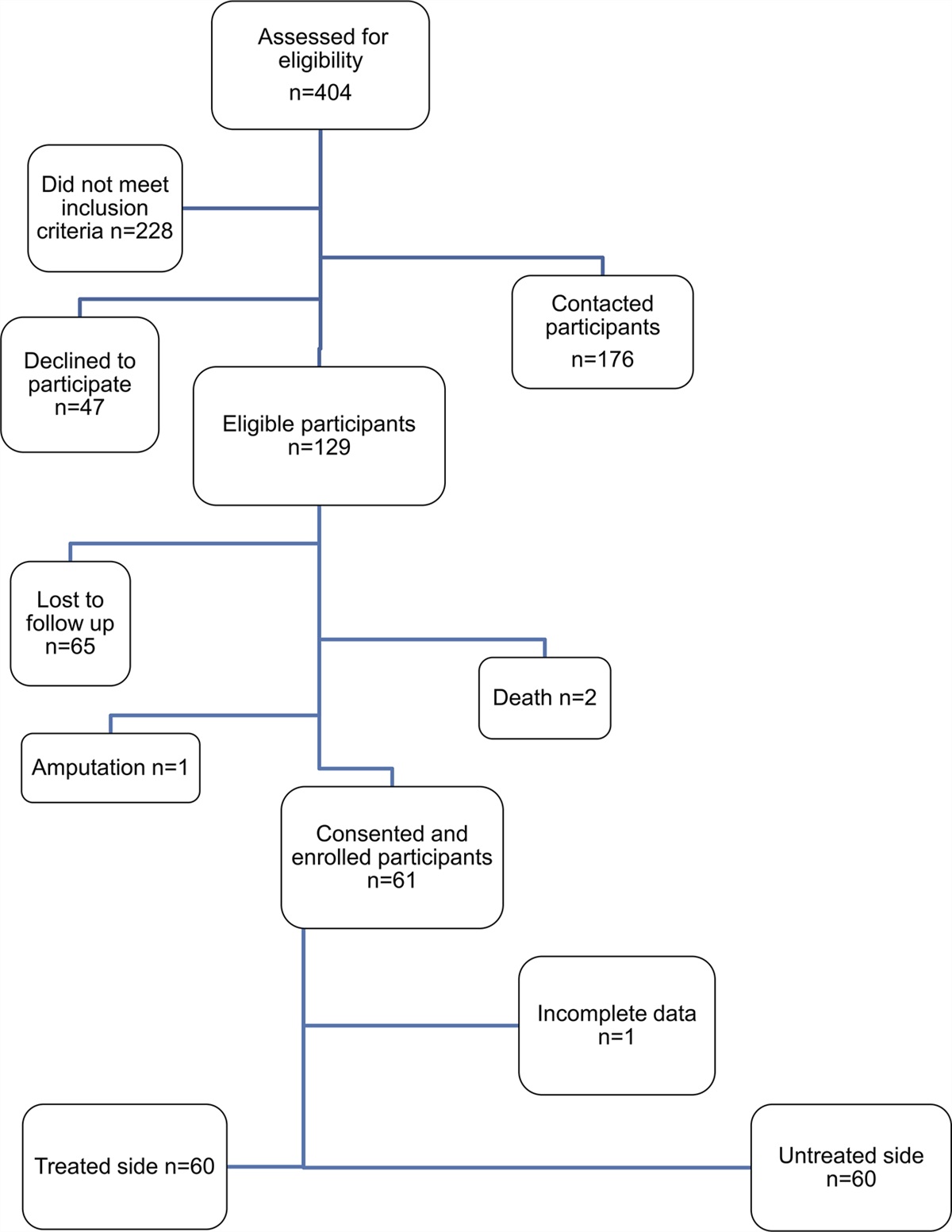
ResultsA retrospective chart review identified 152 initial cases for review. Excluded cases included wrong code (n = 32), poor intraoperative imaging precluding radiographic measurements for analysis (n = 20), and patient died before 30 days of the initial procedure (n = 3). Of the 97 cases who met inclusion criteria, 18 (18.6%) were revised within 30 days. The reason for revision in all cases was loss of reduction as shown in follow-up radiographs. The average time to revision was 5.3 days. Setting for revision included 15 surgical interventions, 1 retightening in the emergency department, 1 retightening at bedside, and 1 readjustment in clinic. Of the 15 surgical cases, nine had an addition of a forefoot pin to the construct. Figure 3 shows a consort diagram to summarize patient acquisition. No cases of secondary failure were observed after initial revision.
 Figure 3:
Figure 3: Consort diagram to summarize patient acquisition. ED = emergency department
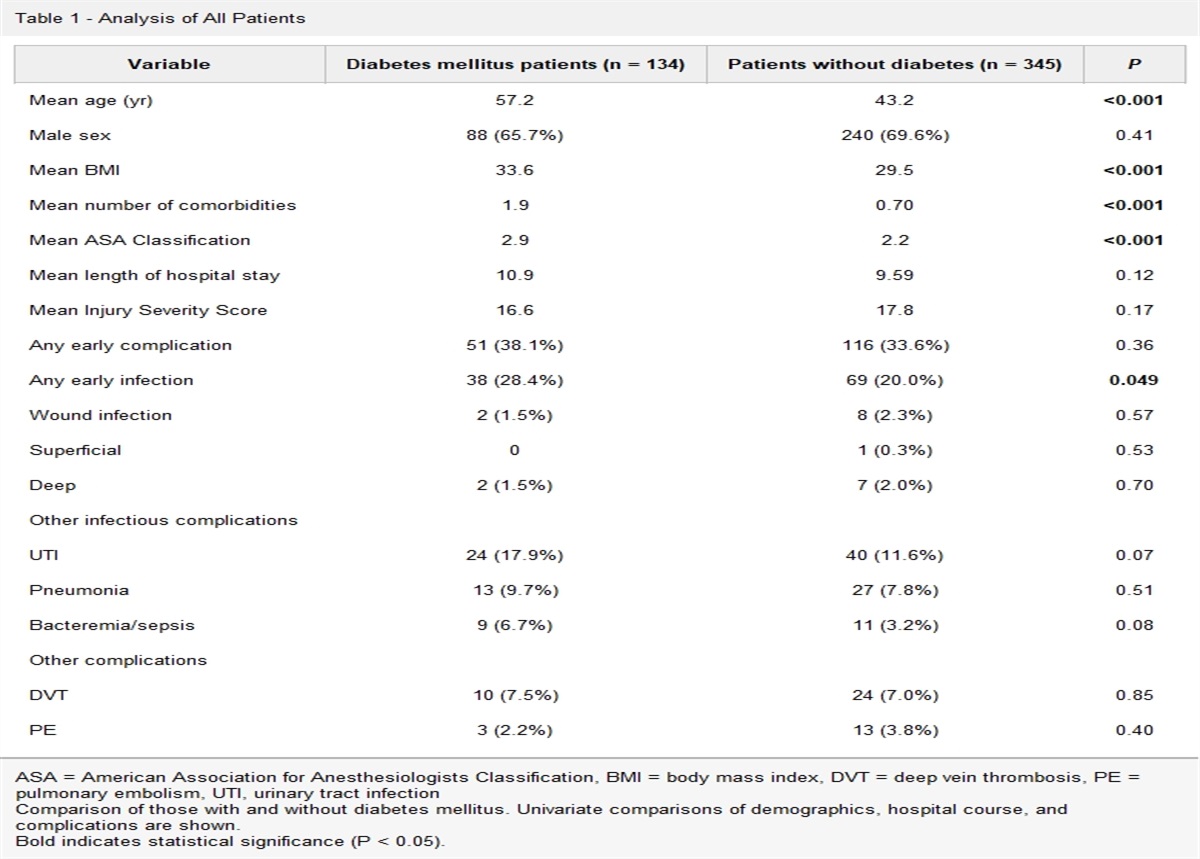
No differences were observed in age, sex, mechanism of injury, smoking history, intravenous drug use, diagnosis of diabetes, fracture type, or dislocation type between the revision group and the nonrevision group (Table 1).
Table 1 - Patient and Injury Characteristics of Patients Who Underwent External Fixation of Unstable Ankle Injuries Fcator No revision (n = 79) % Revised (n = 18) % P Mean age 43.35 48.72 0.178 SD 14.76 16.75 Sex Female 18 28.28 3 16.67 0.570 Male 61 77.22 15 83.33 MOI AvP 7 8.86 1 5.56 0.607 Crush 1 1.27 1 5.56 Fall from height 17 21.52 6 33.33 GLF 5 6.33 0 0.00 GSW 5 6.33 1 5.56 MCC 44 55.70 9 50.00 History of smoking Yes 20 25.32 3 16.67 0.436 No 59 74.68 15 83.33 History of DMII Yes 8 10.13 2 11.11 0.901 No 71 89.87 16 88.89 History of IVDU Yes 6 7.59 3 16.67 0.231 No 73 92.41 15 83.33 Open injury Yes 55 69.62 12 66.67 0.807 No 24 30.38 6 33.33 Fracture type 42A 5 6.33 1 5.56 0.387 42B 14 17.72 4 22.22 42C 6 7.59 0 0.00 44A 18 22.78 3 16.67 44B 10 12.66 5 27.78 44C 23 29.11 3 16.67 Talus 3 3.80 2 11.11 Dislocation type None 47 59.49 7 38.89 0.150 Posterior lateral 22 27.85 5 27.78 Posterior medial 8 10.13 5 27.78 Anterior 1 1.27 0 0.00 Subtalar 1 1.27 1 5.56AvP = automobile versus pedestrian, DMII = diabetes mellitus type II, GLF = ground-level fall, GSW = gunshot wound, IVDU = intravenous drug use, MCC = motor vehicle collision, MOI = mechanism of injury
No differences were observed in posterior malleolar size, staffed by a trauma trained attending, or surgery afterhours between the two groups (Table 2). The revised group had a significantly higher talar tilt (P < 0.001) and was more likely to lack a first metatarsal pin (P = 0.018) and have a poor talar reduction (P < 0.001).
Table 2 - Surgical Characteristics of Patients Who Underwent External Fixation of Unstable Ankle Injuries Factor No revision (n = 79) % Revised (n = 18) % P Posterior malleolar size 1.06 — 1.15 — 0.776 SD 0.89 — 1.23 — Trauma attending Yes 36 54.43 7 38.89 0.607 No 43 45.57 11 61.11 After 6 pm Yes 26 32.91 7 38.89 0.629 No 53 67.09 11 61.11 Configuration Standard 47 59.49 16 88.89 0.018 Standard + addition of forefoot pin 32 40.51 2 11.11 Talocrural angle 12.78 — 12.41 — 0.549 SD 2.21 — 3.12 — Talar tilt 0.16 — 1.65 — <0.001 SD 0.19 — 1.40 — Talar dome position <0.001 Anterior 0 0.00 4 22.22 Middle 79 100.00 13 72.22 Posterior 0 0.00 1 5.56No cases were observed with good (central) talar reduction on final intraoperative radiographs that went on to revision, compared with 5 of 18 revised external fixators (28%) which had poor (either anterior or posterior) talar reductions. Univariate and multivariate analysis could not be run with this factor because of the absence of any talar malreduction on any unrevised case. Of the 18 patients who required revision, 13 patients (72.2%) were initially well reduced in the operating room. Notes for the associated procedure for revision of these cases all noted loss of fixation due to loss of tightening of the ex-fix construct.
The significant risk factors for need for revision on univariate analysis included lack of a first metatarsal pin (odds ratio [OR], 5.56; 95% confidence interval [CI], 1.18 to 25) and talar tilt of >0.5° (OR, 23.08; 95% CI, 6.52 to 81.68).
Multivariate analysis revealed talar tilt >0.5° as a significant risk factor for requiring revision (OR, 22.62; 95% CI, 6.52 to 50.63). No other factors were found to be significant on multivariate analysis (Table 3).
Table 3 - Univariate and Multivariate Analysis of Risk Factors for Need for External Fixation Revision for Unstable Ankle Injuries Factor Univariate Analysis Multivariate Analysis OR P 95% Confidence Interval OR P 95% Confidence Interval Age >65 1.52 0.627 0.28-8.24 0.53 0.705 0.02-14.25 Male sex 1.45 0.571 0.38-5.67 1.29 0.789 0.19-8.76 Smoking 0.59 0.440 0.15-2.25 0.37 0.368 0.04-8.76 DMII 1.11 0.901 0.21-5.72 1.53 0.754 0.04-3.19 IVDU 2.43 0.243 0.55-10.83 0.94 0.961 0.05-17.50 Open injury 0.87 0.807 0.29-2.60 1.61 0.606 0.26-9.76 Fracture type 42 0.83 0.749 0.27-2.59 0.39 0.588 0.01-11.99 Fracture type 44 0.86 0.784 0.30-2.47 0.21 0.442 0.01-11.31 Dislocation 2.31 0.118 0.81-6.59 2.69 0.387 0.29-25.02 Posterior malleolar size >1 cm 0.51 0.271 0.16-1.68 1.51 0.747 0.12-19.79 Case after 6:00 pm 1.30 0.630 0.45-3.74 0.91 0.919 0.16-5.34 Trauma attending as primary surgeon 0.76 0.607 0.28-2.16 0.71 0.679 0.14-3.66 Lack of metatarsal pin 5.56 0.031 1.18-25 0.17 0.110 0.02-1.49 Talocrural angle (<8 or >15°) 0.96 0.959 0.28-3.31 0.26 0.182 0.04-1.86 Talar tilt >0.5° 23.08 <0.001 6.52-81.68 22.62 <0.001 6.52-50.63DMII = diabetes mellitus type 2, IVDU = intravenous drug use, OR = odds ratio
Ankle injuries become unstable when high-energy trauma dissipates energy throughout the limb, causing fracture comminution and shortening, stripping of ligamentous restraints, and damage to the soft tissue envelope. The external fixator is a critical technique to stabilize these injuries. When done properly, an ex-fix provides ligamentotaxis and restores length by spanning the zone of injury. General alignment can also be returned to prevent abnormal force distributions throughout the ankle. These temporizing strategies halt the cascade of damage to the articular surface and the surrounding skin and soft tissues.18 It is a technique that applies broadly throughout the orthopaedic surgery community because these are injuries commonly encountered when on call, regardless of a surgeon's specialty.
Few reports exist on the complications of this technique. An analysis of 59 cases by Oh et al19 reported complications such as failure to obtain 1 cm of length (2%) and medial calcaneal nerve injury (3%). The authors recommend for surgeons to carefully evaluate pin sites for infection because this can lead to failure of the external fixator. It seems that the most common complication is pin site infection, which often self-resolves.20 A more consequential risk is loss of reduction requiring revision of the external fixator. Although there is extensive literature on the use of ankle-spanning external fixation as the first stage in the management of pilon fractures, none took the opportunity to report the rate of revision during the first stage.5,21,22 The study by Barbieri et al23 found a revision rate of 9% for the less commonly used method of hybrid limited internal fixation with external fixation.
Two recent studies helped shed light on revision rates for ankle external fixation. Albagli et al24 found a 18.9% revision rate but failed to identify any notable predictive factors, including the addition of a first metatarsal pin to the delta frame construct. The study by Shah et al25 compared ankle external fixator placement in the operating room versus the emergency department and reported a 15% overall revision rate. The only predictor for revision found was the presence of an unstable ankle injury, as compared with a pilon fracture. Neither of these studies investigated intraoperative radiographic measurements.
Our study found that both increased talar tilt and eccentric positioning of the talus beneath the tibia on the lateral view at final fluoroscopic imaging were markedly associated with failure of external fixation requiring a revision. This agreed with our hypothesis. None of the patients with appropriate talar reductions went on to revision, while 5 of 18 revised external fixators (28%) had poor talar reductions. Talar tilt >0.5° was also a notable risk factor for revision on multivariate analysis.
Although these results may seem intuitive, they have not been reported in previous literature. It is the authors' experience that the technical considerations of external fixation are often underestimated, leading to the genesis of this study. By formally highlighting these findings, we hope to encourage a proper technique to avoid revision surgery. We hope to discourage the misconception that anyone can simply “ex-fix and send out.”
Our method of assessing the reduction of the talus beneath the tibia in intraoperative imaging was based on the idea of dividing the distal tibial metaphysis into an anterior, middle, and posterior segment on the lateral fluoroscopic image, as described by Cosgrove et al.17 It makes intuitive sense that a malreduced ankle joint predisposes the patient to failure of the external fixator system. Surgeons must be critical of the position of the talus beneath the distal tibia and should take the time to obtain a perfect lateral to make this judgement.
Of the 18 patients who required revision, 13 patients (72.2%) were initially well reduced in the operating room, which was defined as central positioning of the talus beneath the distal tibia. 4 of these had an addition of a forefoot pin, and nine had reduction and/or retightening in the clinic, emergency department, or operating room. These findings highlight the importance of ensuring that all components of the external fixator are appropriately tightened before leaving the operating room. Any micromotion from loose points in the construct will only exacerbate over time, leading to loss of reduction. This is a preventable problem when checks are made.
Previous reports have shown that posterior malleolar size can increase rates of loss of reduction with closed reduction and splinting of unstable ankle injuries.26,27 This correlation was not found in our study of external fixator revisions and agrees with the findings by Shah et al.25 Other uncontrollable factors of high-energy ankle fractures including soft tissue swelling, bone loss, and ligamentous instability might also contribute to loss of reduction; however, these are more difficult to quantify. Several methods exist to enhance stability of the external fixation construct, including increased pin diameter, multiplanar or bilateral configuration, increased pin spread, and decreased pin to fracture distance.28
In contrast to findings by Albagli et al, we found that the addition of a forefoot pin was associated with a lower revision rate. Although the lack of a forefoot pin to the standard delta frame configuration was a predictor for revision on univariate analysis, this association did not translate in the multivariate analysis. This agrees with the findings by Shah et al.25 Given the lack of significance on the multivariate analysis, we consider this finding to be in contrast with our initial hypothesis. It should be noted that the addition of a forefoot pin was a common intervention when patients required revision of their ex-fix.
Limitations of this study include its retrospective design, which can introduce bias. Additional studies are needed to prospectively evaluate various factors that might lower revision rates, ultimately focusing on the ideal construct stiffness. Although our method of assessing talar reduction beneath the plafond is not a validated one, it is based on a previously published radiographic study.17 Intraoperative measurements might have interobserver variances; however, one single reviewer completed all measurements for consistency. In addition, we had to exclude 20 of 97 patients who underwent ankle-spanning external fixation due to inadequate intraoperative views which included imperfect lateral and mortise views.
Despite the limitations, this article provides useful information about the rate of revisions of external fixation of high-energy i
留言 (0)