
記住我



Patients frequently ask when it is safe to resume driving after lower extremity surgery, but there is surprisingly little guidance on this topic from physicians' groups, governmental organizations, or driver advocacy organizations. In the United States, there is no policy or law that governs the ability of patients to drive after injury or surgery.1 The American Automobile Association does not give specific recommendations nor does the American Academy of Orthopaedic Surgeons. The question is further complicated because patients with osteoarthritis have decreased baseline braking performance compared with disease-free control subjects.2 The best evidence guiding decision making for when it is safe for patients to return to driving after THA is clinical studies using driving simulators. Multiple studies have investigated when patients return to safe braking times after various lower extremity surgical procedures including arthroplasty. The results of these studies are varied but suggest a return to baseline braking times between 2 and 6 weeks after right total hip arthroplasty.1,3–12 However, much of the data from these studies were collected over a decade ago, before modern THA surgical techniques and early rehabilitation protocols.
The advantages or disadvantages of different surgical approaches is another frequent preoperative question of patients undergoing THA and a topic that has dominated the orthopaedic arthroplasty literature over the past decade. Many studies have suggested early improved functional outcomes, improved pain scores, and less trauma to surrounding tissues with the DAA.13–17 Quarashi et al reported an earlier return to braking after a series of minimally invasive THA compared with previous THA braking studies; however, there was no control group for direct comparison. No study to date has evaluated the effect of surgical approach on the return to safe braking a vehicle. The aim of our study is twofold: (1) to determine if there is a difference in return to preoperative braking between the direct anterior and posterior surgical approaches and (2) to determine with modern surgical techniques and rehabilitation protocols when patients return to their preoperative braking ability after right THA.
MethodsInstitutional Review Board approval was obtained to perform this study. All patients undergoing elective right total hip arthroplasty from April 2018 to March 2020 were screened for enrollment. Inclusion criteria were adult patients undergoing elective right or bilateral primary THA who drive regularly and have an active driver's license. Exclusion criteria were patients undergoing unilateral left THA, those who did not drive, did not have an active driver's license, were undergoing revision surgery, or had preexisting physical or neurologic impairments that prevented them from driving effectively. Patients undergoing left THA were excluded because previous studies demonstrated little effect on brake reaction times when using an automatic transmission.6,18
All patients in the direct anterior approach (DAA) group underwent a standard direct anterior hip approach, and patients in the posterior approach (PA) group underwent a standard posterior hip approach, in both cases by a single experienced fellowship trained arthroplasty surgeon who routinely uses the respective approach. All patients in both groups underwent the same perioperative recovery pathway including preoperative medication, spinal anesthesia, pericapsular analgesic injection, and immediate postoperative physical therapy. All cases were done using noncemented femoral and acetabular components (Accolade II stem and Trident cup, Stryker).
On enrollment, patients completed a baseline HOOS JR form and underwent preoperative testing on a realistic driving simulator that has a dedicated program to measure braking time and force (DriveSafety RS 250 driving simulator; DriveSafety, Murray, UT; Figure 1). To assess braking performance, the subject would partially depress the gas pedal, which turns the stoplight on the screen green and simulates driving at a relatively constant velocity. The study personnel then uses a trigger to initiate the appearance of a red traffic light, on which the patient was instructed to depress the brake pedal as hard as possible.
 Figure 1:
Figure 1: A photograph of our DriveSafety RS 250 driving simulator (DriveSafety) used for the study. This is high fidelity simulator which features an authentic dashboard, steering column, seat, and pedals from a car.
Eight practice trials were done before collecting data at the preoperative session; at follow-up sessions, four practice trials were done to reacquaint the subjects with the protocol. Eight measured braking trials were done preoperatively, and again at 1, 2, and 4 weeks postoperatively. Postoperative HOOS JR scores were collected at the 1-, 2-, and 4-week follow-up as well. Each braking trial measured brake reaction time (BRT), defined as the time between appearance of the red light and a measurable force being detected on the brake, and brake pedal depression (BPD), which is the percentage of full depression achieved during braking. For analysis, the median of each set of trials was used to eliminate the effect of outlier data.
Statistical analyses were done in R (R Core Team). Mixed-effects models were used for the repeated-measures assessment of groups over time. Additional univariate analyses were done with Fisher exact tests for categorical data, and either t-tests or Mann-Whitney U tests as appropriate for continuous data.
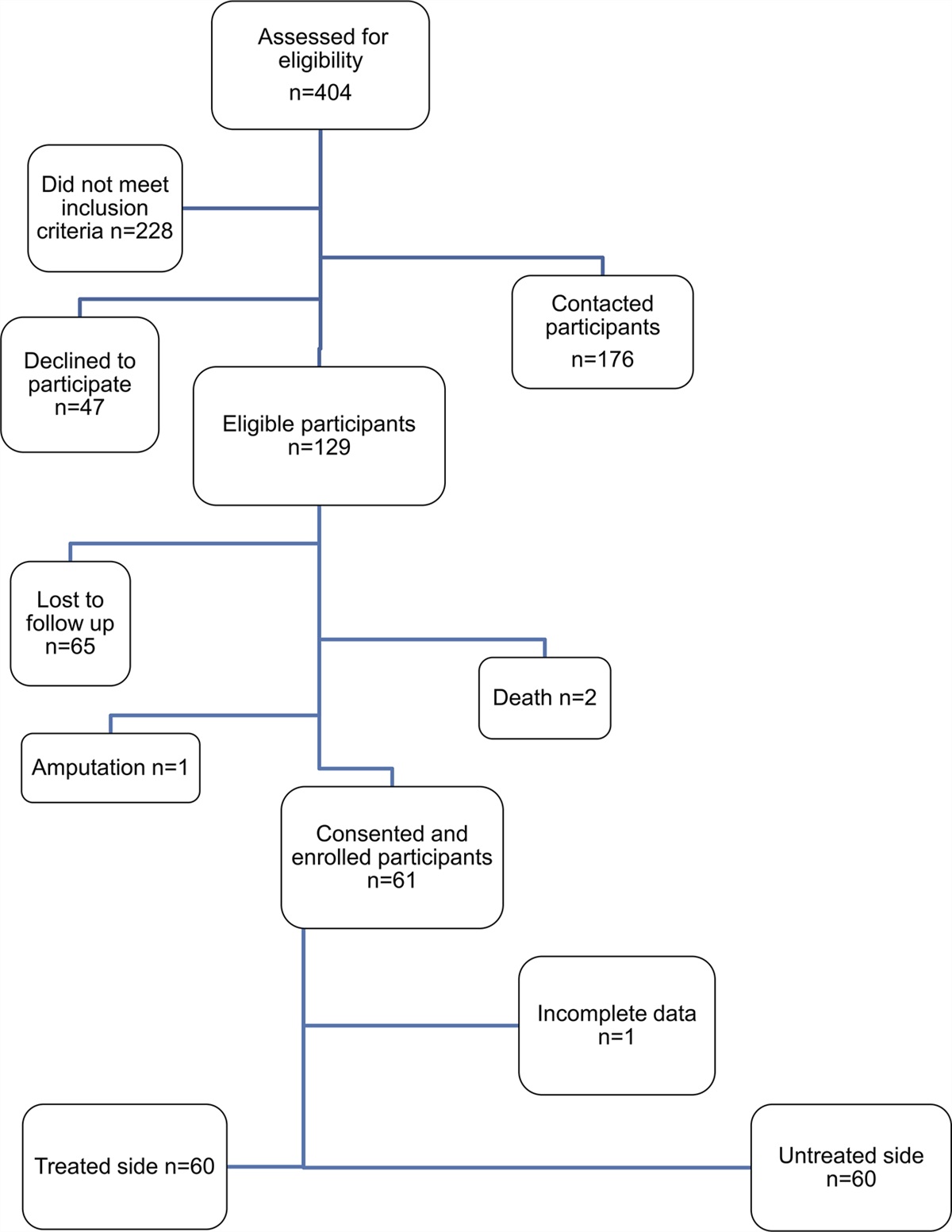
Results Baseline Patient CharacteristicsBaseline characteristics of each group are detailed in Table 1. We enrolled 65 patients who received right-sided primary THA at our institution from April 2018 to March 2020, 34 with a DAA and 31 with a posterior approach (PA). No notable differences were observed between groups in patient sex, age, preoperative HOOS JR score, or proportion undergoing bilateral surgery.
Table 1 - Baseline Characteristics Attribute Anterior (n = 34) Posterior (n = 31) Male sex 21 21 Age 55.8 57.8 Preoperative HOOS JR score 50.6 55.9 Bilateral surgery 7 2Preoperative BRT averaged 638 msec (95% CI 596 to 683) in the DAA group and 604 msec (95% CI 562 to 648) in the PA group (P = 0.31). At 1 week postoperatively, BRT was significantly prolonged compared with preoperatively in the DAA group (694 msec, 95% CI 647 to 744; P = 0.016), but not significantly prolonged in the PA group (633 msec, 95% CI 647 to 744; P = 0.307). At 2 weeks postoperatively, mean BRT in the DAA group was similar to preoperatively (621 msec, 95% CI 580 to 666; P = 0.682) and trended toward being faster than preoperatively in the PA group (562 msec, 95% CI 522 to 604; P = 0.062). Both groups were significantly faster at 4 weeks postoperatively than before surgery (DAA: 583 msec, 95% CI 544 to 626; P = 0.01; PA: 537 msec, 95% CI 499 to 578; P = 0.001). BRT times are presented in Table 2 and Figure 2.
Table 2 - Brake Reaction Time Time Point DAA BRT (msec) (95% CI) Delta From Preop (msec) P PA BRT (msec) (95% CI) Delta From Preop (msec) P Preop 638 (596-683) — 604 (562-648) — 1 week postop 694 (647-744) +56 0.016 633 (588-682) +29 0.307 2 week postop 621 (580-666) −17 0.682 562 (522-604) −42 0.062 4 week postop 583 (544-626) −55 0.01 537 (499-578) −67 0.001DAA = direct anterior approach, BRT = brake reaction time
 Figure 2:
Figure 2: Graph showing the average brake reaction time of the direct anterior and posterior approach groups over time.
Although the average BRT in both groups was markedly faster at 4 weeks compared with preoperatively, in total, there were 24% of patients who did not return to their preoperative BRT even by the 4-week follow-up. A categorical analysis of return to preoperative BRT between the DAA and PA groups is detailed in Table 3. Less patients in the DAA group returned to their baseline BRT or faster compared with the PA group at all periods. However, this difference was only significant at the 4-week follow-up (DAA group: 60%, PA group 93%; P = 0.005).
Table 3 - Return to Preoperative BRT Time Point Percentage DAA Percentage PA Total Percentage P 1 week postop 42% 44% 43% 1.0 2 weeks postop 56% 71% 63% 0.287 4 weeks postop 60% 93% 76% 0.005DAA = direct anterior approach, BRT = brake reaction time
Preoperative BPD averaged 79% (95% CI 70.2 to 87.7) in the DAA group and 84.9% (75.8 to 94.1) in the PA group (P = 0.34). BPD did not change significantly in either group at any time point (Table 4).
Table 4 - Brake Pedal Depression Time Point DAA BPD (%) (95% CI) Delta From Preop (%) P PA BPD (%) (95% CI) Delta From Preop (%) P Preop 79.0 (70.2-87.7) — 84.9 (75.8-94.1) — 1 week postop 75.2 (66.3-84.0) −3.8% 0.507 80.5 (71.1-89.8) −4.4% 0.421 2 weeks postop 75.2 (66.4-84.0) −3.8% 0.498 81.9 (72.6-91.2) −3.0% 0.683 4 weeks postop 79.9 (71.0-88.8) +0.9% 0.967 87.1 (77.8-96.4) +2.2% 0.832DAA = direct anterior approach, BRT = brake reaction time
Preoperative HOOS JR scores averaged 50.6 (95% CI 45.9 to 55.3) in the DAA group and 55.9 (95% CI 50.9 to 60.8) in the PA group (P = 0.165). Improvements from baseline were noted at each time point in the DAA group, whereas the increase was not significant at 1 week postoperatively in the PA group (P = 0.205) but was significantly higher at 2 and 4 weeks postoperatively. HOOS JR scores are detailed in Table 5.
Time Point DAA BPD (%) (95% CI) Delta From Preop (%) P PA BPD (%) (95% CI) Delta From Preop (%) P Preop 50.6 (45.9-55.3) — 55.9 (50.9-60.8) — 1 week postop 63.4 (58.5-68.3) +12.8 <0.001 60.9 (55.7-66.1) +5 0.205 2 weeks postop 72.5 (67.7-77.3) +21.9 <0.001 71.8 (66.8-76.8) +15.9 <0.001 4 weeks postop 77.0 (72.1-81.9) +26.4 <0.001 79.0 (74.0-84.0) +23.1 <0.001DAA = direct anterior approach, BRT = brake reaction time
The results of our study demonstrate a possible early functional benefit with the posterior approach compared with the DAA regarding brake reaction time. In addition, our results demonstrate that on average, patients in both study groups returned to baseline BRT by 2 weeks after surgery. To the best of the authors' knowledge, this is one of the first studies to evaluate the effect of surgical approach on postoperative braking of a vehicle. The PA group had no notable difference in BRT at 1 week compared with preoperative BRT. A notable increase was observed in BRT at 1 week in the DAA group. However, in both groups, the average BRT did return to baseline at the 2-week follow-up. Previous studies have shown that the primary muscle groups involved with braking a vehicle are the hip flexors and knee extensors.19 Given the anatomic proximity of these muscle groups to the DAA and relative separation from the PA, a greater impairment of these muscle groups could be expected from the DAA. Despite the average BRT returning to baseline by 2 weeks in both groups, 40% of patients in the DAA had not returned to their baseline BRT by 4 weeks compared with only 3% in the PA group. This suggests that there is decreased braking performance that persists beyond 2 weeks in the DAA group and is possibly related to persistent, mild weakness in the hip flexor or quadriceps muscle groups.
Despite the differences in BRT between the two groups, the results of our study did not find any notable difference in the BPD or HOOS JR scores between the two groups. This finding suggests that there is little overall functional difference in the maximum strength of the muscles in the lower extremity regarding braking a vehicle. The differences related to approach seem to be more likely related to the coordinated ability to quickly transfer from the gas pedal to the brake as observed in BRT. This finding is consistent with previous studies which have shown few differences in overall muscle strength between the DAA and PA in the postoperative period.20,21
Although our results demonstrate a statistically significant improved braking performance with the PA group, the clinical significance of this difference may be less clear. Operating a motor vehicle is a multifaceted process which requires complex visual, auditory, and neuromuscular coordination. There are many factors outside of BRT alone that can impair a patient's ability to safely operate a vehicle in the postoperative period, including age, pain, nausea, opioid, or other pain medications and neuraxial anesthesia. The difference between the return to baseline BRT observed between the two groups at the 1-week follow-up alone may not translate to the ability to safely operate a motor vehicle at that time. A study by Green et al. demonstrated that on average, drivers who were aware of an impending stop could react to the brake within 0.7 seconds and unaware drivers could with 1.5 seconds. Nearly all patients in our study, regardless of surgical approach, fell within these guidelines.22
Alternatively, the failure to return to preoperative BRT by the 4-week follow-up, as observed with the DAA group, could have a profound clinical impact for some patients. Patients who are eager to return to work sooner, those who live in remote or rural areas, or patients whose occupations involve driving could be affected by these findings. In addition, although the differences between the groups are very small, millisecond differences on the brake pedal can translate to collisions on the roadway. For example, the difference of just 0.06 seconds can translate to the width of a crosswalk in stopping distance when traveling at 60 miles per hour. Ultimately, the decision to proceed with one surgical approach or another is multifactorial. The potential ability to return to driving 1 week sooner is unlikely to be the critical factor guiding these decisions; however, these results provide data for patients and surgeons to make informed decisions.
Independent of the surgical approach, the results of our study support that with modern surgical techniques and postoperative rehabilitation protocols, on average, patients return to baseline preoperative brake reaction times approximately 2 weeks after right THA. These findings are consistent with one other modern series which also evaluated BRT after right THA and found that 87% of patients returned to baseline braking 2 weeks after surgery.9 With a lack of specific guidance from laws, medical organizations, and insurance companies, patients and surgeons are left to themselves to decide when it is safe to return to driving after elective total hip arthroplasty. Clinical studies provide some guidance to aid in this decision-making process.
Previous studies suggested that underlying hip arthritis alone decreased braking performance and that patients did not return to safe, baseline braking times until approximately 6 weeks after hip replacement surgery. Advances in surgical techniques, multimodal pain management, and rehabilitation protocols likely account for the quicker return to preoperative braking times observed in recent studies. These updated data provide additional information to aid in deciding when it is safe to return to driving. The average preoperative braking times for the patients in both groups were within safe standards. Our results demonstrated that patients returned to this preoperative level sooner than previously thought and even exceeded it by 4 weeks. Ultimately, driving is a complex multifactorial process, and each patient requires a personalized approach to determine when they are safe to return to driving after total hip arthroplasty.
One potential limitation is the relatively young average age of our patient population. The average age of patients in the DAA group and PA group was 55.8 and 57.8, respectively. Younger patients recover more quickly after surgery and on average have better reaction times, likely contributing to the earlier return to braking observed in our study. This potentially makes our results less generalizable to the average population undergoing elective THA. However, there was no notable difference in baseline characteristics between the DAA and PA groups making any differences between the groups more likely attributable to the surgical approach. An additional limitation of our study is the relatively small sample size. Given the prospective design of the study and the need for frequent follow-up appointments, a notable number of patients who were eligible for the study elected not to participate. An additional limitation of the study is braking in a simulator that might not completely translate to safely braking a car in a real-world situation. We attempted to mitigate this by using a highly realistic driving simulator and standardized the testing protocol. Based on previous literature which suggested a return to preoperative BRT within 4 weeks of surgery, we chose to restrict follow-up to this period to avoid unnecessary burden on the study participants. However, despite the markedly faster BRT at 4 weeks overall, 40% of patients in the anterior group did not return to their preoperative BRT at this period.9,12 Additional follow-up testing would provide a more complete picture of when each individual patient returned to baseline but likely provides limited clinical significance.
In conclusion, with modern surgical techniques and rehabilitation protocols, patients can, on average, return to safely braking a vehicle approximately 2 weeks after right total hip arthroplasty. The posterior approach may provide an early functional benefit, but the clinical significance of this difference is modest at best.
AcknowledgementsThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors thank Dr. Sameer K. Saxena for his important contributions to the institutional review board protocol to make this project possible.
References 1. MacLeod K, Lingham A, Chatha H, et al.: “When can I return to driving?”: A review of the current literature on returning to driving after lower limb injury or arthroplasty. bone joint J 2013;95-B:290-294 2. Hofmann UK, Jordan M, Rondak I, Wolf P, Kluba T, Ipach I: Osteoarthritis of the knee or hip significantly impairs driving ability (cross-sectional survey). BMC Musculoskelet Disord 2014;15:20 3. Patel PV, Giannoudis VP, Palma S, et al.: Doctor when can I drive? A systematic review and meta-analysis of return to driving after total hip arthroplasty. Hip Int 2023;33:17-27 4. Qurashi S, Chinnappa J, Lord SJ, Nazha A, Gordon J, Chow J: Driving after microinvasive total hip arthroplasty. The J arthroplasty 2017;32:1525-1529 5. Bäcker HC, Krüger D, Spies S, Perka C, Kirschbaum SM, Hardt S: Effect of total hip arthroplasty on brake reaction time and braking force. Hip Int: J Clin Exp Res hip Pathol Ther 2022;32:51-55 6. Ganz SB, Levin AZ, Peterson MG, Ranawat CS: Improvement in driving reaction time after total hip arthroplasty. Clin Orthop Relat Res 2003;413:192-200 7. Huang H-T, Liang J-M, Hung W-T, Chen Y-Y, Guo L-Y, Wu W-L: Timeframe for return to driving for patients with minimally invasive knee arthroplasty is associated with knee performance on functional tests. BMC Musculoskelet Disord 2014;15:198 8. DiSilvestro KJ, Santoro AJ, Tjoumakaris FP, Levicoff EA, Freedman KB: When can I drive after orthopaedic surgery? A systematic review. Clin Orthop Relat Res 2016;474:2557-2570 9. Hernandez VH, Ong A, Orozco F, Madden AM, Post Z: When is it safe for patients to drive after right total hip arthroplasty? J arthroplasty 2015;30:627-630 10. Dalury DF, Tucker KK, Kelley TC: When can I drive?: Brake response times after contemporary total knee arthroplasty. Clin Orthop Relat Res 2011;469:82-86 11. McDonald EL, Pedowitz DI, Shakked RJ, et al.: When is it safe to drive after total ankle arthroplasty? Clin orthopaedics Relat Res 2020;478:8-15 12. van der Velden CA, Tolk JJ, Janssen RPA, Reijman M: When is it safe to resume driving after total hip and total knee arthroplasty?: A meta-analysis of literature on post-operative brake reaction times. bone joint J 2017;99-B:566-576 13. Goebel S, Steinert AF, Schillinger J, et al.: Reduced postoperative pain in total hip arthroplasty after minimal-invasive anterior approach. Int Orthop 2012;36:491-498 14. Restrepo C, Parvizi J, Pour AE, Hozack WJ: Prospective randomized study of two surgical approaches for total hip arthroplasty. J arthroplasty 2010;25:671-679.e1 15. Christensen CP, Jacobs CA: Comparison of patient function during the first six weeks after direct anterior or posterior total hip arthroplasty (THA): A randomized study. J arthroplasty 2015;30:94-97 16. Bergin PF, Doppelt JD, Kephart CJ, et al.: Comparison of minimally invasive direct anterior versus posterior total hip arthroplasty based on inflammation and muscle damage markers. The J bone joint Surg Am volume 2011;93:1392-1398 17. Cheng TE, Wallis JA, Taylor NF, et al.: A prospective randomized clinical trial in total hip arthroplasty—comparing early results between the direct anterior approach and the posterior approach. J arthroplasty 2017;32:883-890 18. MacDonald W, Owen J: The effect of total hip replacement on driving reactions. The J bone joint Surg Br volume 1988;70:202-205 19. Behr M, Poumarat G, Serre T, Arnoux P-J, Thollon L, Brunet C: Posture and muscular behaviour in emergency braking: An experimental approach. Accid Anal Prev 2010;42:797-801 20. Winther SB, Foss OA, Husby OS, Wik TS, Klaksvik J, Husby VS: Muscular strength and function after total hip arthroplasty performed with three different surgical approaches: One-year follow-up study. Hip Int 2019;29:405-411 21. Winther SB, Husby VS, Foss OA, et al.: Muscular strength after total hip arthroplasty. A prospective comparison of 3 surgical approaches. Acta Orthop 2016;87:22-28 22. Green M: “How long does it take to stop?” Methodological analysis of driver perception-brake times. Transportation Hum Factors 2000;2:195-216
留言 (0)