
記住我



Supracondylar humerus fractures (SCHFs) are the most common pediatric elbow injury, accounting for 15% of pediatric orthopaedic consults and 12% of pediatric orthopaedic surgeries.1 Optimizing value in this well-studied high-volume injury will, therefore, largely affect costs and patient experience. The ratio of healthcare benefits to costs defines value. To maximize value, we must decrease cost without negatively affecting patient outcomes or experience and improve benefits without commensurately increasing direct and indirect costs.
Decreasing defensive medicine, unnecessary transfers, after-hours surgery, and advanced and repeated imaging will all decrease costs. Usually, modalities that decrease cost concomitantly improve both patient experience and outcomes, for example, reducing opioids, office visits, and therapy. Operational issues such as chronic staffing shortages and lack of hospital beds during surges are also improved by maximizing nonsurgical care, limiting outpatient visits, and minimizing inpatient surgical care in lieu of outpatient surgery when possible. Longer term environmental concerns, such as operating room (OR) waste generation and car pollution from travel to and from visits, should also be factored into decision making.
Many patients and caregivers are not well equipped to make value-based decisions.2 Even physicians are left with many gray zones for best practices. For example, the 2012 American Academy of Orthopaedic Surgeons clinical practice guidelines are inconclusive regarding timing of treatment with concomitant neurovascular injury, pin removal, immobilization, and radiographs. This study will guide cost-effective and resource-saving practices while maintaining high quality of clinical outcomes based on the available evidence and author's clinical experience.
Nonsurgical Care PreventionThe proverb ‘an ounce of prevention is worth a pound of cure’ comes to mind, as the best cost savings and decreased patient morbidity is fracture prevention. Vitamin D supplementation decreases the odds of fracture in children.3 Reduced sun exposure and obesity are risk factors for the potential need for supplementation.4 Just as the ‘Own the Bone’ campaign encouraged orthopaedic surgeons to play an active role in the bone health of elderly patients, families should be encouraged to improve the quality of children's diet, vitamin D intake, and activity levels while caring for pediatric fractures.
Nondisplaced and Minimally Displaced FracturesNonsurgical treatment is indicated for Type I (nondisplaced, nonangulated) fractures. Comprehensive nonsurgical fracture care consists of immobilization, serial radiographs to assess for displacement until stabilization around 3 weeks, and then allowing early range of motion during final fracture healing (around 6 weeks). Multiple studies of Type I fractures have confirmed long arm splinting to be noninferior to casting for safe immobilization during fracture stabilization,5,6 and the author's general preference is a long arm plaster splint (Table 1). Serial radiographs can sometimes be skipped because the risk of displacement is low, and in very young children under 8 years, there is good remodeling potential. The third week visit is often the last because only a sling is used thereafter. With full understanding that the sling may end up mostly off the elbow, it still serves as a small reminder of caution to patients during the last 3 weeks of healing.
Table 1 - Superiority of Splinting Over Casting Factor Splint (Long Arm Plaster) Cast (Long Arm Fiberglass) Fracture stability Posterior slab can extend further proximal to the fracture on the humerus Proximal extension limited by the axillary fold Material cost Plaster rolls $0.84 each Fiberglass roll $1.97, plus stockinette OR costs No separate Current Procedural Terminology code Separate CPT code Application time Plaster posterior and strut slabs prepared preoperatively, applied directly to Webril and covered with ACE wrap, can dry while patient waking up Stockinette application, fiberglass application, stockinette folding, and more fiberglass application +/− drying and uni/bivalving time while under anesthesia Room for swelling Noncircumferential splint allows room to swell Only possible with uni or bivalving, which requires more surgical time and risks cast saw injury in an anesthetized patient Postoperative visits None additional Often 1 week visit recommended for overwrapping bivalved cast, incurring additional visit, material cost, and time Removal Able to be unwrapped by medical assistants, and is less scary than using a cast saw Requires training in cast saw use, incurs risk of cast saw burns, and adds to patient anxiety Medicolegal risk If concerned for swelling and cannot be evaluated immediately, can be removed at home Requires specialized equipment for safe removal and incurs risk of cast saw burnsActivity restrictions are empirically lifted 6 weeks after injury because low nonunion and reinjury rates preclude the need for radiographs at this time point. This streamlined approach minimizes missed school and work for families along with travel, and orthopaedic offices and radiology services are freed up for other patients. Most importantly, children can enjoy the mental and physical benefits of being physically active without waiting for full return to motion or the subjective quantification of radiographic callus.
Nonsurgical Closed ReductionType II fractures (anterior cortical displacement > 2 mm with intact posterior hinge) are divided into IIa, with extension only, and IIb, which are additionally translated/rotated. Multiple studies of nonsurgical management of Type IIa fractures have shown over 70% rates of maintained closed reduction.7,8 Procedural sedation is associated with an 83% rate of successful nonsurgical management of Type IIa fractures compared with 56% in those without.7 One Level 1 trauma hospital found that their surgeons chose nonsurgical management in 75% of Type IIa fractures with a <5% need for surgical fixation.9 This was an exception to their overall 92% adherence to the 2014 American Academy of Orthopaedic Surgeons Appropriate Use Criteria (AUC), as the ‘appropriate’ recommendation for Type II fractures is surgical reduction with percutaneous pinning and reduction and casting is categorized as ‘may be appropriate,’ without distinction between IIa and IIb patterns.
While less than half of IIb fractures have a successful first reduction, and only 1/3 are able to complete nonsurgical care, those that do maintain successful alignment without surgery show no difference in clinical or radiographic outcomes compared with Type IIa fractures or compared with IIb fractures with surgical management.10 It is important to recognize that while surgery offers more consistent outcomes, in the setting of other factors that may increase the cost or morbidity of surgical management (distance, family resources, mobility, illness, lack of pediatric anesthesia), Type IIb fractures that are acceptably reduced and maintain their reduction at 1 week have similar outcomes to those treated surgically.10
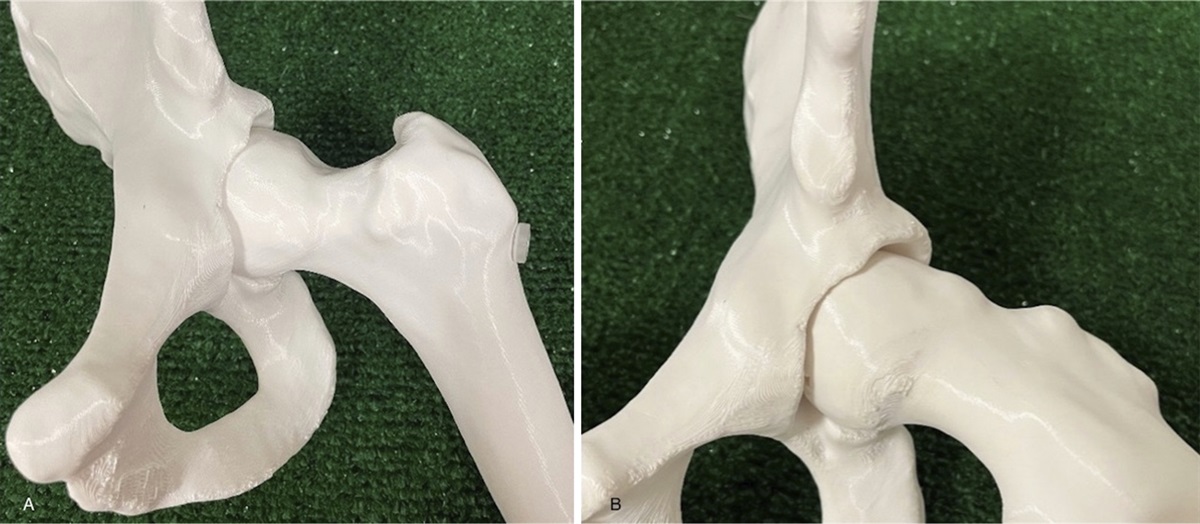
The proximity of SCHFs to the elbow joint, desire to restore near-full range of motion, and relatively limited distal humeral remodeling potential make most surgeons intolerant of all but near-anatomic reduction. It is generally accepted that the ossification of the capitellum should be anterior to the anterior humeral line on lateral radiographs. The author emphasizes the need for perfect lateral radiographs to assess sagittal alignment and often will request repeat laterals obtained with the beam directed from medial to lateral through the elbow with the patient supine and externally rotating the shoulder for optimal alignment (Figure 1).
 Figure 1:
Figure 1: A, Radiographs showing the three views of an elbow fracture referred for surgical management because the capitellar ossification center appears angulated posterior to the anterior humeral line, that is, a Gartland Type II. B, Recognizing that this is not a true lateral, because the patient was likely unable to tolerate a lateral due to discomfort, the patient was immobilized for comfort, and radiographs repeated with the patient supine and the shoulder externally rotated, with the beam directed from medial to lateral. This provides the perfect lateral, with the ‘hourglass’ sign, and demonstrates this to be a more anatomic Gartland Type I, precluding the need for reduction or surgery.
One study examining posterior malunions demonstrated complete or near-complete remodeling in 90% of their patients aged 2 to 8 years.11 It concluded that children younger than 5 years can remodel 100% displacement of their capitellum. This information should factor into decision making on the need for closed reduction, particularly if being considered with procedural sedation, which is associated with a higher rate of maintained alignment, but may be unnecessary if there is remodeling potential. In addition, as stated earlier, in children younger than 5 years with Type 1 fractures, weekly radiographs can be precluded because even in the event of angulation into extension, conversion to surgical management is unlikely.
Surgical Care Location and Surgeon TrainingClosed reduction and percutaneous pinning (CRPP) is currently indicated for most fully displaced fractures (Types IIb, III, and IV). Location, surgeon training, and timing of surgery have value implications. One teaching hospital charged an average of $6345 per CRPP.12 The cost breakdown in a descending order included the OR (67%), anesthesia (13%), fluoroscopy (11%), and implants (1%). One study comparing CRPP of mostly Type 2 fractures in a community hospital showed 44% cost savings over a teaching hospital, with over half of the savings coming from reduced OR costs and the remainder being from anesthesia, imaging, and supplies.13 Community hospitals are more likely to have non-pediatric orthopaedic specialists; however, outcomes are similar and satisfactory compared with pediatric fellowship-trained surgeons.14 The latter offers more efficient care, with pediatric surgeons having shorter surgical time (average 13 minutes), less fluoroscopic time, more delayed surgery over 12 hours, and fewer postoperative visits.14,15 One study also showed pediatric orthopaedic surgeons to have more optimal pin constructs and lower rates of iatrogenic nerve injuries (all of which resolved), but both groups ultimately had no differences in major loss of reduction.16 Another study found rates of open reduction, postoperative Baumann angle, and complications to be similar regardless of training background.15 Value is, therefore, not routinely improved by transferring patients to surgeons with pediatric training given the higher monetary and time costs of travel to further facilities for surgery and subsequent follow-ups. Despite the cost, however, transfers will continue to appropriate for certain situations to optimize patient care.
Timing of SurgeryTiming of surgery also has value implications. SCHF surgeries performed between 11pm and 6am are associated with more malunions despite equivalent rates of open reduction, surgical time, and complications,17 although importantly these ‘overnight surgeries’ tend to be on more severe fractures. There has been a shift toward outpatient treatment, which reduces surgical time and costs.18 In New York, outpatient management went from 23% in 2009 to 59% in 2018, with both immediate and delayed cost savings. Inpatient surgeries billed $16,097 vs outpatient costs of $9752. Outpatients had fewer return visits to the emergency department within 1 month.19 However, outpatient care requires a caregiver at home, the absence of serious medical problems, and reasonable proximity to a surgical center. Although these are not modifiable factors, knowing these resource requirements can prompt surgeons to enlist the help of ancillary support as necessary to optimize value (eg, care coordination for transportation).
Treatment within 18 hours is tracked as a quality metric for the US News and World Report pediatric hospital ranking, despite multiple studies demonstrating the safety of delay in most situations. A large multicenter study of patients with anterior interosseous nerve palsies who underwent CRPP at an average of 15 hours (range 2 to 36) demonstrated no cases of compartment syndrome, and the authors concluded that a delay up to 24 hours did not increase time to nerve recovery or other complications.20 A single institution reported performing 65% of their CRPPs of Type III and IV SCHFs the following day with an average delay of 12 hours and found that timing, vascular status, nerve injury, and lateral displacement did not correlate with complications21 (Figure 2). Their complication rate only correlated with younger ages. The authors proposed early treatment for abnormal neurovascular status and next-day treatment for the remainder. Interestingly, they found that surgeons in practice for less than 15 years were 14 times more likely to treat early versus those in practice longer, with no difference in their complication rates.21 Another study looked at surgery within 24 hours for Type III fractures and found that those treated before or after 12 hours had no difference in surgical time, reduction quality, or rate of opening.22 It is important to keep in mind that while a delay in treatment is acceptable, a delay in evaluation is not benign because without assessment for open injuries, concomitant fractures, compromised perfusion, and compartment syndrome, fractures may be inappropriately triaged.
 Figure 2:
Figure 2: Image showing significant skin puckering and displacement seen with this fracture, and while it is ideal to provide gentle traction during timely initial evaluation and splinting, emergent after-hours surgery has not been shown to improve outcomes.
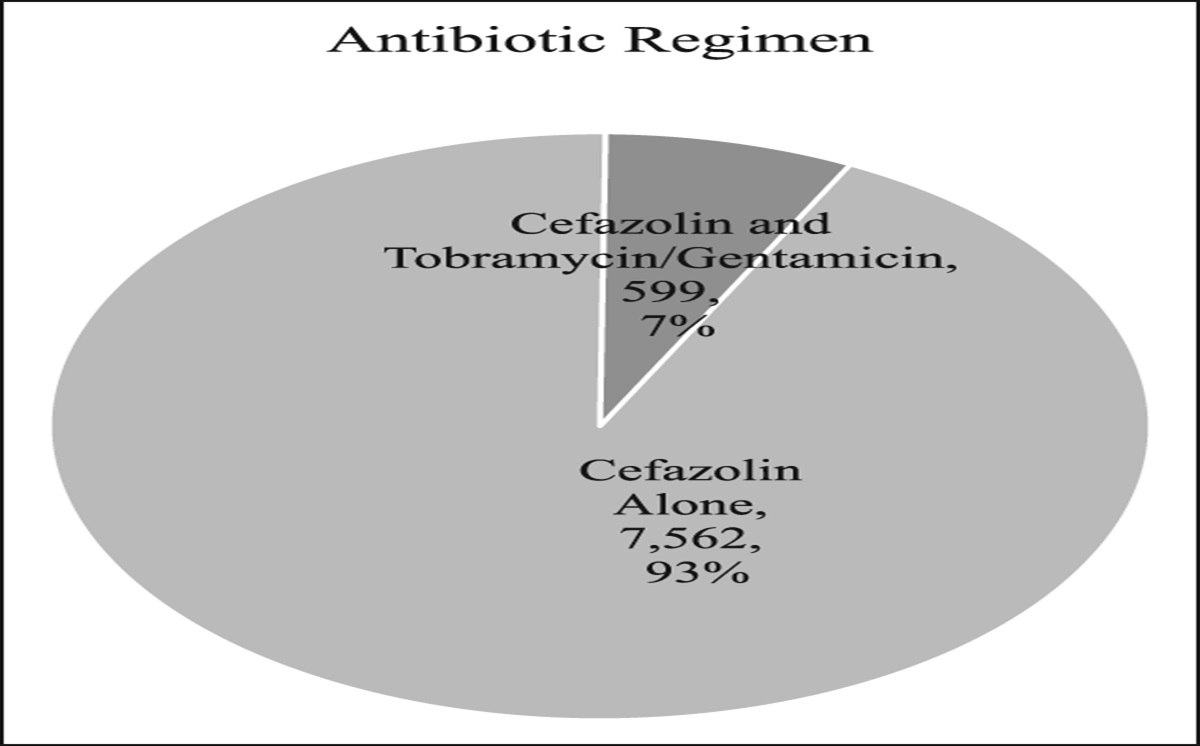
Surgical PreparationOR preparation can be optimized to minimize cost. It is the author's practice to avoid antibiotics in all CRPP cases. One study found an infection rate of 0.6% in 337 patients who received antibiotics and 0.4% in those who did not.23 Another series of infections after CRPP demonstrated 1/3 to be associated with a wet cast;24 therefore, effort should be directed at counseling families on the importance of cast care. Use of a semisterile technique using sterile gloves and towel draping, forgoing gowns and drapes, is safe, with no pin site infections in over 300 cases.25 This saves on setup time, environmental waste, and OR costs. The author has incorporated this by positioning an undraped mini-C-arm under the elbow at the start and prepping and towel draping the elbow atop the machine, which also precludes the cost and waste of the large plastic fluoroscopy drape (Figure 3). A small prep table containing a ‘pin set,’ or a few individually opened instruments, is set up, with additional instruments available but not open should the case become more complex (Figure 4). As preference card editing has been well established as one of the most effective ways to cut down on operating room monetary and environmental costs, Table 2 lists the instruments and supplies to be open for a typical CRPP case.
 Figure 3:
Figure 3: Images of the patient positioned supine with the arm abducted and extended onto a regular arm board. The mini-fluoroscopy is positioned atop the arm board with the laser localizer at the fracture line, which precludes the need for a radiolucent board or positioning the patient at the edge of the bed, which keeps their head safely positioned more centrally on the OR table. After prepping the arm atop the undraped fluoroscopy unit, two blue towels are placed longitudinally under the arm, and one towel is placed to cover the patient’s shoulder and face (A). When the elbow is flexed, the proximal towel keeps the hand from being contaminated (B).
 Figure 4: Photographs showing supplies for a minimal setup (A), specifically the three-quarter drape to cover the prep table, sterile blue towels, gloves, Xeroform, felt, and a ‘pin set,’ with the relevant instruments listed in Table 2. Prep bowls and gauze are also helpful so that saline can be used to clean the elbow before splinting, and a local anesthetic can be injected about the pin sites and fracture (B).
Table 2 -
Preference Card Sample for a Supracondylar Humerus Fracture Closed Reduction And Percutaneous Pinning Minimalist Setup
Instruments
Supplies
Prep bowls (for saline, local, etc.)
Three-quarter sheet (to drape prep table)
Power driver and pin collets
Saline
Wires (smooth)
Blue towel pack
Wire cutter
Sterile gloves
Needle driver or plier
Prep stick
Xeroform/felt
Gauze
Syringe/needle (for local anesthetic injection)
Sterile Webril
Figure 4: Photographs showing supplies for a minimal setup (A), specifically the three-quarter drape to cover the prep table, sterile blue towels, gloves, Xeroform, felt, and a ‘pin set,’ with the relevant instruments listed in Table 2. Prep bowls and gauze are also helpful so that saline can be used to clean the elbow before splinting, and a local anesthetic can be injected about the pin sites and fracture (B).
Table 2 -
Preference Card Sample for a Supracondylar Humerus Fracture Closed Reduction And Percutaneous Pinning Minimalist Setup
Instruments
Supplies
Prep bowls (for saline, local, etc.)
Three-quarter sheet (to drape prep table)
Power driver and pin collets
Saline
Wires (smooth)
Blue towel pack
Wire cutter
Sterile gloves
Needle driver or plier
Prep stick
Xeroform/felt
Gauze
Syringe/needle (for local anesthetic injection)
Sterile Webril
The surgical technique varies, yet literature does exist to guide various aspects. Closed reduction should be performed whenever possible, with validated reduction maneuvers being pronation for posterior and posteromedial displacement and supination for posterolateral displacement (Figure 5). Risks of requiring open reduction include flexion types (IV) and coronal displacement >7 mm,26 so while these fractures are still predominantly treated with CRPP, the potential need for opening could be anticipated and factored into a more standard prep-and-drape setup. Loose bone fragments on x-ray are seen in 2.6% of patients and are not an indication for opening because these fragments absorb or reunite eventually.27
 Figure 5:
Figure 5: Anteroposterior and lateral radiographs of a Gartland Type III fracture with posterolateral displacement and rotation is demonstrated. Supination and traction will improve axial and coronal alignment, respectively, before flexing the fracture to restore the sagittal plane.
Divergent retrograde oblique pins, at least two for Type II injuries and three for Types III and IV, are ideally placed from the lateral side (Figure 6). Medial pinning carries a 4% risk of iatrogenic ulnar nerve palsy, and although 90% of palsies recover,28 this is stressful for both families and physicians and can increase the number of visits. The author avoids medial entry pins except when medial column comminution precludes adequate bicortical purchase for all the lateral entry pins. On these occasions, at least two lateral entry pins should still be used to stabilize the reduction in flexion, and then the elbow can be extended for medial pin entry. In cases where wires skive off the second cortex and travel up the humeral shaft, a larger caliber lateral wire is used instead of switching to a medial pin. Pins should be bent and cut to rest outside the skin and wrapped with Xeroform to minimize pin-skin interface motion. Buried pins back out less but are associated with more skin irritation, outpatient visits, costs, and burdens.29
 Figure 6:
Figure 6: Three lateral entry divergent pins stabilized this Type III fracture for 3 weeks. Purchase in the olecranon fossa provided additional fixation compared with bicortical purchase alone. With the callus now present, there is enough stability such that pins can be removed in clinic because they were cut and bent to rest outside the skin percutaneously.
ImagingIntraoperative and postoperative imaging should be optimized to reduce cost and radiation exposure. One study found that fluoroscopy time and radiation dose were not affected by resident participation, instead it varied based on the fracture type, number of pins, and operating surgeon.30 For this reason, although the author provides hands-on teaching to trainees, the mini-C-arm pedal is always controlled by the attending surgeon to minimize exposures to only those that are necessary to guide safe pin placement and ensuring the elbow is held steady and centered with laser guidance to avoid blurry or suboptimal shots. In addition, the author makes a point to save views that demonstrates the maximum residual displacement and angulation. Some amount of nonanatomic reduction is acknowledged to be present and acceptable, and any subsequent postoperative radiographs, for example, after a fall or report of new pain, can be truly assessed for a change in alignment warranting a return to the OR for revision versus a different view but unchanged alignment from index surgery.
Mini-fluoroscopy offers several advantages over large-C-arms because staff over 3 feet away do not require lead shielding, a fluoroscopy technician is not needed during the case, and pulsed dose settings minimize exposure to both patients and surgeons. Additional intraoperative fluoroscopy after pinning and immobilizing does not change management.31 Finally, either pre or post-pin removal radiograph can be ordered, but doing both does not add value or change management.
Pain ManagementPain management plays an important role in patient experience and can influence the number of phone calls and unexpected follow-ups to the surgeon's office. Intraoperative ketorolac reduces pain and inpatient opioid use and length of stay by 50%, along with lower inpatient hospitalization, resulting in a 34-fold return-on-investment cost savings, with no difference in complications.32 Postoperative acetaminophen is as effective as narcotics after CRPP, but with fewer adverse effects.33 Pain should be discussed postoperatively, both to set reasonable expectations and to know what is concerning for pain out of proportion, which could indicate compartment syndrome. Strategies to minimize opioid use include preoperative informed consent for opioids34 and standard order sets.35 The author's practice is to avoid prescribing opioids, using intraoperative bupivacaine injection about the fracture and pin sites along with ketorolac administration, in conjunction with education about combining acetaminophen and ibuprofen for maximum nonopioid analgesia. Elevation above the level of the heart and active finger movement to pump edema back can mitigate postoperative swelling and pain, which is why the author avoids routine sling use, which discourages both elevation and finger movement.
ImmobilizationAnother postoperative factor that can play a large role in improving value is the type of immobilization. The author has a strong preference for plaster splinting over fiberglass casting for both nonsurgical and postoperative immobilization (see Table 1) because a splint allows for more proximal immobilization up the posterior humerus while the proximal extent of a cast is limited by the axillary fold. Plaster splinting also decreases direct costs with lower material costs and less OR time. Plaster slabs can be prepared ahead of time while fiberglass needs stockinette application, layered wrapping, folding of stockinette edges, additional wrapping, and then drying time before valving. Experts recommend a curing time of 10 minutes for fiberglass and 12 minutes for plaster36 before cast saw use, and still the risk of burns is higher than baseline because patients are under anesthesia. Patients with valved casts often have a separate visit for fiberglass overwrapping and later are subjected to a loud/scary cast saw for removal. The use of postoperative splinting over casting improves the flow of clinic as cast beds are not necessarily needed, and staff without cast saw knowledge can unwrap the splint.
Multiple studies have shown no difference in unscheduled returns or secondary displacement with splinting versus casting.37,38 The author has had good success with ∼10 layers of plaster for a posterior splint supplemented with a ∼5-layered lateral slab to cover pins, with an ACE wrap applied directly onto the plaster while drying to make it harder to remove.
Postoperative CarePostoperative care should ensure appropriate clinical recovery and radiographic healing with the least burden to patients, caregivers, healthcare facilities, and the entities paying for the incurred costs. The author has previously published an algorithm for streamlining postoperative care.39 Routine fractures receive only one postoperative visit around 3 to 4 weeks for a 2-view radiograph, pin removal, instruction on a home exercise program, three additional weeks of activity restriction and sling use, and counseling on the expected course and when/why to contact the office for additional visits. Because patients have high anxiety regarding pin removal, this is performed at the end of the visit so that children can then leave the clinic and recover in a more comfortable environment. This is why we radiograph children out of their splint before pin removal, and no post-pin removal radiographs are repeated because they do not change management. We avoid visits for motion checks because families can assess for this themselves or demonstrate their motion through telemedicine. Therapy referral is not routinely used because worse 9 and 15-week post-injury scores and higher 9-week anxiety scores have been demonstrated with therapy.40 Patients with a home exercise program have similar return time to activities of daily living and sports with no difference in elbow motion compared with those who do therapy. If families specifically request therapy, they are counseled on these data, but we also encourage families to contact the office for a referral if motion is not near-normal by 4 months post injury.
SummaryThis article seeks to provide evidence-based recommendations for improving patient outcomes and experience while decreasing healthcare costs associated with pediatric SCHFs. Fracture prevention is ideal, which is why orthopaedic surgeons should appropriately counsel patients on vitamin D intake and the importance of having healthy body weight. Nonsurgical care should be used in nondisplaced and successfully closed reduced SCHFs. While routine management consists of immobilization and weekly radiographs for 3 weeks, with conversion to surgical management for loss of reduction, fractures with sagittal plane remodeling potential, particularly in children younger than 5 years, can forgo some of this for efficiency.
For surgical management, the cost of routine transfer to pediatric fellowship-trained surgeons and specialty hospitals is not justified given the similar outcomes. Outpatient surgery offers cost savings over inpatient management. Emergent after-hours surgery in the setting of Type III and IV injuries, even in the setting of nerve injury or diminished pulse, is not required as long as the hand is well perfused and closely monitored.
It is safe and economical to forgo preoperative antibiotics, gowns, and full drapes. Using a semisterile technique, surgeon-operated mini-C-arm, and lateral pins when possible will improve surgical efficiency. Subcutaneous local, intravenous ketorolac, and oral acetaminophen and ibuprofen should preclude the need for narcotics. A plaster long arm splint provides strong protection at a lower cost and higher safety profile compared with a fiberglass long arm cast. Routine postoperative care can be streamlined to a single visit and radiograph for pin removal.
References 1. Schultz JD, Rees AB, Wollenman LC, et al.: Factors that drive Annual variation in pediatric elbow fracture occurrence, severity, and resource utilization. J Pediatr Orthop 2021;41:e755-e762. 2. Bozic K, Wright JG: Value-based healthcare and orthopaedic surgery. Clin Orthop Relat Res 2012;470:1004-1005. 3. Anderson LN, Heong SW, Chen Y, et al.: Vitamin D and fracture risk in early childhood: A case-control study. Am J Epidemiol 2017;185:1255-1262. 4. Williams K, Hughes D, Horan M: Vitamin D trends in the pediatric orthopaedic population: A survey. J Pediatr Orthop 2020;40:e58-e62. 5. Cuomo AV, Howard A, Hsueh S, Boutis K: Gartland type I supracondylar humerus fractures in children is splint immobilization enough. Pediatr Emerg Care 2012;28:1150-1153. 6. Siu C, Farrell S, Schaeffer EK, et al.: Long - arm splinting versus above - elbow casting for type 1 supracondylar fractures of the humerus in children: A randomized controlled trial. SN Compr Clin Med 2023;5:72. 7. Ojeaga P, Wyatt CW, Wilson P, Ho CA, Copley LAB Jr, Ellis HB Jr: Pediatric type II supracondylar humerus fractures: Factors associated with successful closed reduction and immobilization. J Pediatr Orthop 2020;40:690-696. 8. Mccartney CC, Thompson S, Waller G, et al.: Gartland type IIa supracondylar humerus fractures: Outcomes of attempted nonoperative management. J Pediatr Orthop 2022;42:314-320. 9. Douleh DG, Carry P, Sanders JS, Rhodes JT: Pediatric supracondylar humerus fracture AAOS appropriate use Criteria: Does treatment at a pediatric level I trauma center comply. J Pediatr Orthop 2022;42:470-473. 10. Sisman A, Avci O, Cepni SK, Cullu E: Is there a chance to treat modified Gartland type IIB pediatric supracondylar humerus fractures with closed reduction and casting. J Pediatr Orthop 2022;42:821-827. 11. Gamble JG, Vorhies JS: Remodeling of sagittal plane malunion after pediatric supracondylar humerus fractures. J Pediatr Orthop 2020;40:903-909. 12. Su AW, Lee MC: The cost and educational experience of treating supracondylar humerus fractures: A pilot analysis on standardizing surgical care. J Am Acad Orthop Surg Glob Res Rev 2020;4:e20.00063. 13. Shasti M, Li T, Case AL, Hariharan A, Jauregui JJ, Abzug JM: Cost analysis of treating pediatric supracondylar humerus fractures in community hospitals compared with a tertiary care hospital. J Am Acad Orthop Surg 2020;28:377-382. 14. Fisher BT, Chong ACM, Flick T, Forness M, Sauer BR, Peterson JB: Does surgeon subspecialty training affect outcomes in the treatment of displaced supracondylar humerus fractures in children? Brandon J Am Acad Orthop Surg 2021;29:447-457. 15. Bram JT, Defrancesco CJ, Pascual-leone N, Gross PW, Doyle SM, Fabricant PD: Impact of pediatric orthopaedic fellowship training on pediatric supracondylar humerus fracture treatment and outcomes: A meta-analysis. J Pediatr Orthop 2023;43:e86-e92. 16. Sullivan MH, Stillwagon MR, Nash AB, et al.: Complications with surgical treatment of pediatric supracondylar humerus fractures: Does surgeon training matter. J Pediatr Orthop 2022;42:8-14. 17. Paci GM, Tileston KR, Vorhies JS, Bishop JA: Pediatric supracondylar humerus fractures: Does after-hours treatment influence outcomes. J Orthop Trauma 2018;32:215-220. 18. Rider CM, Hong VY, Westbrooks TJ, et al.: Surgical treatment of supracondylar humeral fractures in a freestanding ambulatory surgery center is as safe as and faster and more cost-effective than in a children’ s hospital. J Pediatr Orthop 2018;38:343-348. 19. Modest JM, Brodeur PG, Lemme NJ, Testa EJ, Gil JA, Cruz AI Jr: Outpatient operative management of pediatric supracondylar humerus fractures: An analysis of frequency, complications, and cost from 2009 to 2018. J Pediatr Orthop 2022;42:4-9. 20. Barrett KK, Skaggs DL, Sawyer JR, et al.: Supracondylar humeral fractures with isolated anterior interosseous nerve injuries: Is urgent treatment necessary. J Bone Jointt Surg Am Vol 2014;96:1793-1797. 21. Mahan ST, Miller PE, Park J, Sullivan N, Vuillermin C: Fully displaced pediatric supracondylar humerus fractures: Which ones need to go at night. J Child Orthop 2022;16:355-365. 22. Okkaoglu MC, Ozdemir E, Ozdemir E, Karaduman M, Ates A, Altay M: Is there an optimal timing for surgical treatment of pediatric supracondylar humerus fractures in the first 24 hours. J Orthop Surg Res 2021;16:484-486. 23. Bloomer AK, Coe KM, Brandt AM, Roomian T, Brighton B, Scannell BP: Hold the antibiotics: Are preoperative antibiotics unnecessary in the treatment of pediatric supracondylar humerus fractures? J Pediatr Orthop 2022;42:474-479. 24. Ezeokoli EU, Borici N, Serrano E, Inneh I, Shenava V, Smith BG: Early postoperative infections after closed reduction and percutaneous pinning in type II and type III pediatric supracondylar humerus fractures. J Pediatr Orthop 2022;42:732-735. 25. Iobst CA, Spurdle C, King WF, Lopez M: Percutaneous pinning of pediatric supracondylar humerus fractures with the semisterile technique the Miami experience. J Pediatr Orthop 2007;27:17-22. 26. Latario LD, Lubitz MG, Narain AS, Swart EF, Mortimer ES: Which pediatric supracondylar humerus fractures are high risk for conversion to open reduction. J Pediatr Orthop B 2023;32:569-574. 27. Yang L, Yang P, Li L, Tang X: The outcome of loose bone fragments in pediatric supracondylar humerus fractures: A retrospective study. J Pediatr Orthop B 2022;31:12-17. 28. Ho CA, Gottschalk H, Samora JB, et al.: Diagnosis and management of nerve injuries caused by pediatric upper extremity fractures. J Pediatr Orthop Soc North America 2023;5:708. 29. Suganuma S, Tada K, Shingo T, Hidetoshi Y, Shimanuki K, Shinmura K, et al.: Comparing exposed and buried kirschner wires in fi xation for pediatric supracondylar humerus fractures: A propensity score-matched study. J Orthop Sci 2022;30:1-7. 30. Schmucker A, Chen R, Vachhrajani S, Martinek M, Albert M, Albert M: Radiation exposure in the treatment of pediatric supracondylar humerus fractures. Arch Orthop Trauma Surg 2020;140:449-455. 31. Flood MG, Bauer MR, Sullivan MP: Radiographic considerations for pediatric supracondylar humerus fractures. J Pediatr Orthop B 2023;32:110-116. 32. Adams AJ, Buczek MJ, Flynn JM, Shah AS: Perioperative ketorolac for supracondylar humerus fracture in children decreases postoperative pain, opioid usage, hospitalization cost, and length-of-stay. J Pediatr Orthop 2019;39:447-451. 33. Swanson CE, Chang K, Schleyer E, Pizzutillo P, Herman M: Postoperative pain control after supracondylar humerus fracture fixation. J Pediatr Orthop 2012;32:452-455. 34. Williams BA, Magee LC, Makarewich CA, Swarup I, McNeely L, Shah A: Preoperative opioid informed consent and prescribing practices in children undergoing orthopaedic trauma surgery. J Am Acad Orthop Surg Glob Res Rev 2022;6:e21.00309-8. 35. Goodloe JB, Bailey EP, Luce LT, et al.: A standardized order-set improves variability in opioid discharge prescribing patterns after surgical fixation of pediatric supracondylar humerus fractures. J Surg Educ 2021;78:1660-1665. 36. Steiner SRH, Gendi K, Halanski MANK, Noonan KJ: Efficiency and safety: The best time to valve a plaster cast. J Bone Jointt Surg 2018;100:e49. 37. Lee HA, Buczek MJ, Talwar D, Horn BD, Davidson RS: Post-operative splinting versus casting of pediatric supracondylar humerus fractures. Cureus 2021;13:e17635. 38. Azzolin L, Angelliaume A, Harper L, Lalioui A, Delgove A, Lefèvre Y: Optimal postoperative immobilisation for supracondylar humeral fractures. Orthop Traumatol Surg Res 2018;104:645-649. 39. Patel HA, Chaudhry S, Lee MC, Solomito M: Streamlining postoperative care after pediatric supracondylar humerus fractures: Is follow-up after pin removal routinely needed? J Pediatr Orthop 2021;41:e464-e469. 40. Schmale GA, Mazor S, Mercer LD, Bompadre V: Lack of benefit of physical therapy on function following supracondylar humeral fracture: A randomized controlled trial. J Bone Joint Surg Am Vol 2014;96:944-950.
留言 (0)