
記住我


Despite high worldwide prevalence of chronic pain during childhood,30,41,47 there is a small evidence base to reduce uncertainty in commonly used pharmacological, psychological, physical, and integrative interventions for pediatric chronic pain.26 Many gaps remain in finding effective and safe treatments for specific populations and in accessing treatments in different settings.58 A major goal of the field is to improve assessment of pain and related experience.21 There has been considerable progress over the past 2 decades in pediatric pain assessment, which has produced many measures for different core outcome domains.22,37,48,51,61 In addition, several systematic reviews have been conducted to summarize the evidence base concerning the psychometric properties of measures for pediatric chronic pain outcomes including pain severity,7,10,71 pain impact,23 and sleep.16,45
Building on the work of the Ped-IMMPACT group,51 we updated a core outcome set (COS) for pediatric chronic pain clinical trials using stakeholder feedback from multidisciplinary providers, youth, and parents.60 The new COS includes 3 mandatory domains: pain severity, pain interference with daily living, and adverse events, and 4 optional domains: overall well-being, emotional functioning, physical functioning, and sleep quality.60 Although the original Ped-IMMPACT core outcome set included recommendations for measures, expert opinion was the principal methodology used to derive these recommendations. Those discussions took place in 2005 and do not reflect more recent contributions to pediatric chronic pain assessment. Thus, those recommendations need to be updated using more rigorous procedures for selecting outcome measures.
Our aim was to use a multiphased approach to identify and recommend patient-reported measures for each core outcome domain identified in our new COS for pediatric chronic pain. The intention of the recommendations is to offer guidance on specific measures that could be deployed across clinical trials of pharmacological, psychological, physical, and integrative interventions for pediatric chronic pain. We expected that we could identify responsive, valid, and reliable measures for chronic pain assessment in children and adolescents within each of the core outcome domains.
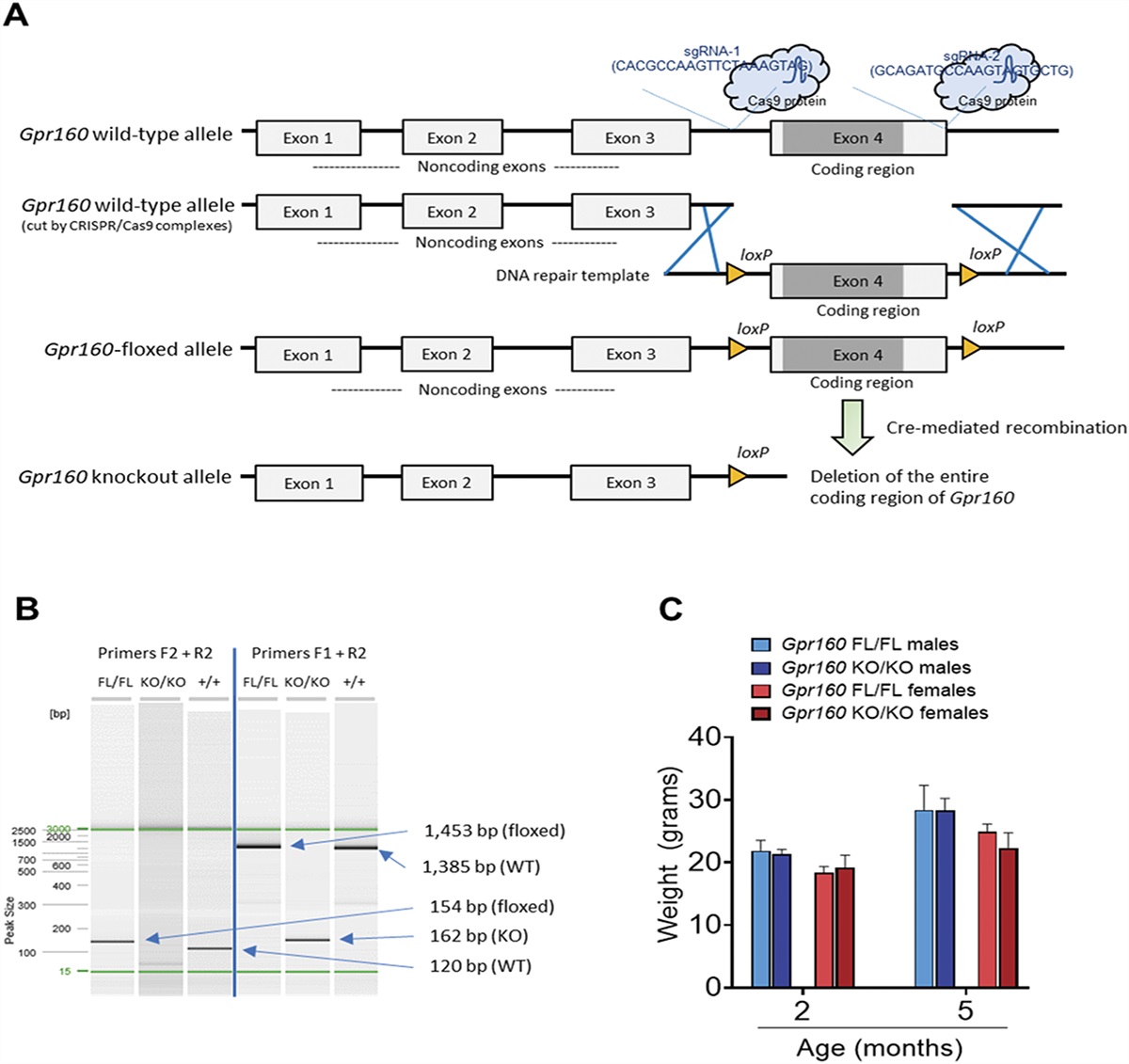
2. Methods 2.1. Study overviewSelection of patient-reported outcome measures for each of the 7 identified domains of the new COS for pediatric chronic pain trials was conducted in 3 phases. The overall approach to measure selection was guided by the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) initiative,52 with the greatest weight given to content validity, developmental appropriateness, reliability, responsiveness to change, and usability. Work was conducted in 3 phases: (1) a Delphi study of experts to identify candidate measures, (2) a review phase to gather evidence for measurement properties of the candidate measures, and (3) a consensus conference among our Core-OPPP steering committee to make final recommendations. See Figure 1 for the 3-phase process for deriving evidence-based recommendations. The study was approved by the institutional review board at the Seattle Children's Research Institute.
 Figure 1.:
Figure 1.: Summary of the 3-phase process for deriving evidence-based recommendations for patient-reported outcome measures for each core outcome domain of the core outcome set (COS) for pediatric chronic pain clinical trials.
2.2. Delphi studyWe identified candidate measures by conducting a 2-round Delphi study with experts in pediatric chronic pain interventions, defined as having served as a first or senior author on a published trial or systematic review of chronic pain interventions in children and adolescents. We identified 84 individuals and invited their participation in a 2-round Delphi poll. The study had institutional review board approval.
In the first round, experts generated a list of patient-reported measures they regarded as psychometrically sound for use in clinical trials of interventions for children and adolescents with chronic pain within each of the core outcome domains. Because the domain of Adverse Events in pain trials has been recently reviewed and did not include any pediatric-specific measures, we did not include the domain Adverse Events in our survey.57 We categorized all the responses verbatim and narrowed the list of measures to those reported by at least 2 experts.
We then sent out round 2 surveys to the experts who completed round 1. In this survey, experts were asked to rate individual measures (from the narrowed list) by their suitability and appropriateness on a 0 to 10 scale anchored by the phrases “Based on psychometric properties of the instrument and feasibility” and “How suitable/appropriate is the [index measure] for assessing the [index domain],” and to further identify one “best” measure for each core outcome domain. In determining the suitability and appropriateness, respondents were asked to consider the measurement properties of the instrument (eg, content validity, internal consistency [if appropriate], and factor structure) as well as the feasibility (eg, clinical utility, access, and length). For identifying the “best” instrument, investigators were asked to select 1 instrument that should be prioritized for each domain of interest. Domain definitions were provided at the beginning to facilitate the rating and selection process, and investigators were allowed to skip the rating for any instrument about which they lacked knowledge. There were open-ended fields to provide comments regarding each domain.
Following the 2-round Delphi poll, we performed an initial evaluation to further reduce the list of candidate measures. We excluded measures that were less likely to be recommended for use in pediatric chronic pain trials due to limitations in content fit, developmental appropriateness, or clinical utility. For content fit, we excluded measures not fitting the domain concept (eg, the Pain Catastrophizing Scale for Children is a cognitive/emotional process, potential mechanism, or coping strategy rather than an emotional functioning “outcome” measure) or measures of broad concept coverage that are less precise in representing the domain of interest and/or overlapping with other domains (eg, the PedsQL Generic Core Scales—Psychosocial Summary Score is a combination of the emotional, social, and school functioning subscales). For developmental appropriateness, we excluded measures that were developed among adult populations and have not been validated for children and adolescents (eg, the Graded Chronic Pain Scale). For clinical utility, we excluded lengthy measures that we judged burdensome for participants (eg, Revised Children's Anxiety and Depression Scale) when shorter measures were available.
2.3. Evidence synthesis for measurement propertiesWe gathered evidence regarding measurement properties for the candidate measures using multiple strategies. As per the COSMIN guideline,14 we searched the COSMIN database of systematic reviews of measurement properties for patient-reported outcomes. To increase the specificity and relevance of the search, we used a targeted search strategy by searching for individual candidate measures as identified from previous phases. The search was performed by R.L. in August 2021 using a combination of the target population (age 0-18 years), name of the measure, and/or the keyword “pain” (see Supplemental Table 1 [available at https://links.lww.com/PAIN/B953] for the detailed search strategy). All review studies published until that time were searched. The title, abstract, and full text (when appropriate) were screened, and reviews providing measurement information on any of the candidate measures were included. Additional reviews were referenced by the committee and searched on databases as relevant for the selection of measures for pediatric populations with chronic pain. An additional literature search was performed for individual measures if no evidence was available from these review articles.
After the abovementioned literature search, we determined that the Patient-Reported Outcome Measurement Information System (PROMIS) pediatric measures have not been systematically evaluated in any previously published reviews. Because a number of these measures were highly rated and strongly preferred by experts who participated in the Delphi study (Phase 1), we decided to conduct a separate COSMIN systematic review for all PROMIS pediatric measures with the purpose of evaluating their measurement properties in children and adolescents with chronic pain.46
Pooled evidence of measurement properties for all candidate measures, by domain, was compiled, including an overview of the key strengths and limitations. The summary tables were provided to the Core-OPPP steering committee in preparation for the consensus meeting as described further.
2.4. Expert consensus for measurement recommendationA virtual consensus conference was held with the Core-OPPP steering committee (T.M.P., G.A.W., S.K.Z., C.E., G.C., K.A.B., and A.L.S.) in June 2022 to present synthesized evidence, determine a set of criteria for measure recommendations, discuss appropriateness of measures, and discuss any domain-specific considerations. An additional literature review was conducted from discussion items raised at the consensus conference, and modifications were made to the evidence pool. The discussion items included (1) reconsidering a previously excluded measure for the domain of physical functioning, (2) gathering evidence for a newly proposed measure for the domain of overall well-being, (3) determining the appropriate anchors and instructions for a pain intensity measure, (4) considering condition-specific measures, and (5) highlighting the evidence for the most promising version for measures with multiple versions. A virtual voting within the steering committee took place between late July and early August 2022 to determine the final recommendations for outcome measures in each domain.
3. Results 3.1. Phase 1—Delphi studyWe sent emails to 84 experts identified from published trials and systematic reviews of pediatric chronic pain interventions to solicit participation in the Delphi study, and 43 (51%) completed the round 1 survey. Most were psychologists, with more than 10 years of experience in the field of pediatric chronic pain and had conducted clinical trials (mostly behavioral trials) for chronic pain intervention in youth (Table 1). Of the list of measures generated, 50 were mentioned by at least 2 experts, including 7 for pain severity, 5 for pain-related interference with daily living, 5 for overall well-being, 16 for emotional functioning, 8 for physical functioning, and 9 for sleep quality.
Table 1 - Characteristics of professionals who participated in the Delphi study (N = 43). Round 1 Round 1 Percentage Round 2 Round 2 Percentage Total 43 100 39 100 Profession Psychologist 33 77 29 74 Physician 7 16 8 21 Nursing 3 7 2 5 Years of experience 0-10 15 35 10 26 11-19 12 28 13 33 20+ 16 37 16 41 Clinical trial experience Yes 28 65 28 72 No 15 35 11 28Round 2 surveys were sent to experts who participated in the round 1 survey, of whom 91% (n = 39) responded. Average rating scores for the suitability/appropriateness and the priority rankings for all 50 measures are summarized in Table 2. The best scored and most preferred measures were the PROMIS Pediatric Pain Intensity and Numerical rating scale (0-10 NRS) for pain severity; the PROMIS Pediatric Pain Interference and Functional Disability Inventory (FDI) for pain-related interference with daily living; the Pediatric Quality of Life Inventory (PedsQL) Generic Core Scales and PROMIS Pediatric Profile 25 v.2.0 for overall well-being; the PROMIS Pediatric Emotional Distress Scales (Anxiety, Depression, Anger) for emotional functioning; the PROMIS Pediatric Physical Activity and Functional Disability Inventory (FDI) for physical functioning; and the PROMIS Pediatric Sleep Disturbance and Adolescent Sleep Wake Scale (ASWS) for sleep quality.
Table 2 - Professional ratings of the identified measures by domain (n = 39). Average rating (0-10) # Selected as top choice Pain severity PROMIS Pediatric Pain Intensity 8.34 10 Numerical Rating Scale (0-10 NRS) 8.03 10 Graded Chronic Pain Scale 6.69 4 Brief Pain Inventory (BPI) 7.85 3 Faces Pain Scale-Revised (FPS-R) 7.62 3 Visual Analogue Scale (VAS) 7.46 3 Varni Thompson Pediatric Pain Questionnaire 6.50 1 Pain-related interference with daily living PROMIS Pediatric Pain Interference 8.50 15 Functional Disability Inventory (FDI) 8.19 11 Bath Adolescent Pain Questionnaire (BAPQ) 7.56 3 Child Activity Limitations Interview (CALI) 7.45 3 Brief Pain Inventory (BPI) 6.21 0 Overall well-being PedQL Generic Core 7.94 17 PROMIS Pediatric Profile 25 v.2.0 7.32 9 PROMIS Pediatric Global Health 7.60 2 PROMIS Pediatric Life Satisfaction 6.64 2 KIDSCREEN 6.08 0 Emotional functioning PROMIS Pediatric Emotional Distress Scales (anxiety, depression, anger) 7.96 12 Revised Children's Anxiety and Depression Scale (RCADS) 6.70 4 Bath Adolescent Pain Questionnaire (BAPQ) 7.46 3 Child Behavior Checklist (CBCL) 6.20 2 Patient Health Questionnaire-9 (PHQ-9) 5.97 2 PedQL Generic Core—Psychosocial Summary Score 5.53 2 Behavior Assessment System for Children (BASC) 6.07 1 Child Depression Inventory (CDI) 6.86 1 PedQL Generic Core—Emotional Functioning Scale 6.15 1 PROMIS Pediatric Anxiety 7.30 1 PROMIS Pediatric Depression 7.33 1 Generalized Anxiety Disorder–7 (GAD-7) 6.09 0 Multidimensional Anxiety Scale for Children (MASC) 6.52 0 Pain Catastrophizing Scale for Children (PCS-C) 5.19 0 Revised Children's Manifest Anxiety Scale (RCMAS) 6.13 0 Screen for Child Anxiety–Related Disorders (SCARED) 6.52 0 Physical functioning PROMIS Pediatric Physical Activity 7.00 9 Functional Disability Inventory (FDI) 7.61 8 Bath Adolescent Pain Questionnaire—Physical Functioning Scale 7.12 3 Child Activity Limitations Interview (CALI) 6.94 3 PROMIS Pediatric Mobility 7.00 3 PedQL Generic Core—Physical Health Scale 6.80 2 PROMIS Pediatric Lower Extremity Function 6.43 0 PROMIS Pediatric Upper Extremity Function 6.17 0 Sleep quality PROMIS Pediatric Sleep Disturbance 8.05 6 Adolescent Sleep Wake Scale (ASWS) 7.88 6 PROMIS Pediatric Sleep-Related Impairment 8.06 2 Adolescent Insomnia Questionnaire (AIQ) 6.38 1 Insomnia Severity Index (ISI) 6.88 1 Pittsburgh Sleep Quality Index (PSQI) 6.53 1 Pediatric Sleep Questionnaire (PSQ) 6.93 0 Children's Sleep Habits Questionnaire (CSHQ) 6.65 0 Adolescent Sleep Hygiene Scale (ASHS) 6.33 0We excluded measures that we deemed as less likely to be recommended for use in pediatric chronic pain clinical trials due to limitations in content fit, developmental appropriateness, or clinical utility. See Supplemental Table 2, available at https://links.lww.com/PAIN/B953 for the measures excluded and reasons for exclusion. Based on results from the Delphi study and initial evaluation assessing content fit, developmental appropriateness, and clinical utility, the below measures were further considered as candidate measures:
Pain severity: the Numerical rating scale (0-10 NRS), Visual Analogue Scale (VAS), PROMIS Pediatric Pain Intensity,50 and Faces Pain Scale–Revised (FPS-R).34
Pain-related interference with daily living: the PROMIS Pediatric Pain Interference, Functional Disability Inventory (FDI), and Child Activity Limitations Interview (CALI).
Overall well-being: the PROMIS Pediatric Global Health and PROMIS Pediatric Life Satisfaction.
Emotional functioning: the PROMIS Pediatric Depressive Symptoms, PROMIS Pediatric Anxiety, PROMIS Pediatric Anger, Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder–7 (GAD-7), and Children's Depression Inventory (CDI).
Physical functioning: the PROMIS Pediatric Physical Activity, PROMIS Pediatric Mobility, and the Bath Adolescent Pain Questionnaire (BAPQ)–Physical Function Scale.
Sleep quality: the ASWS, PROMIS Pediatric Sleep Disturbance, and PROMIS Pediatric Sleep-related Impairment.
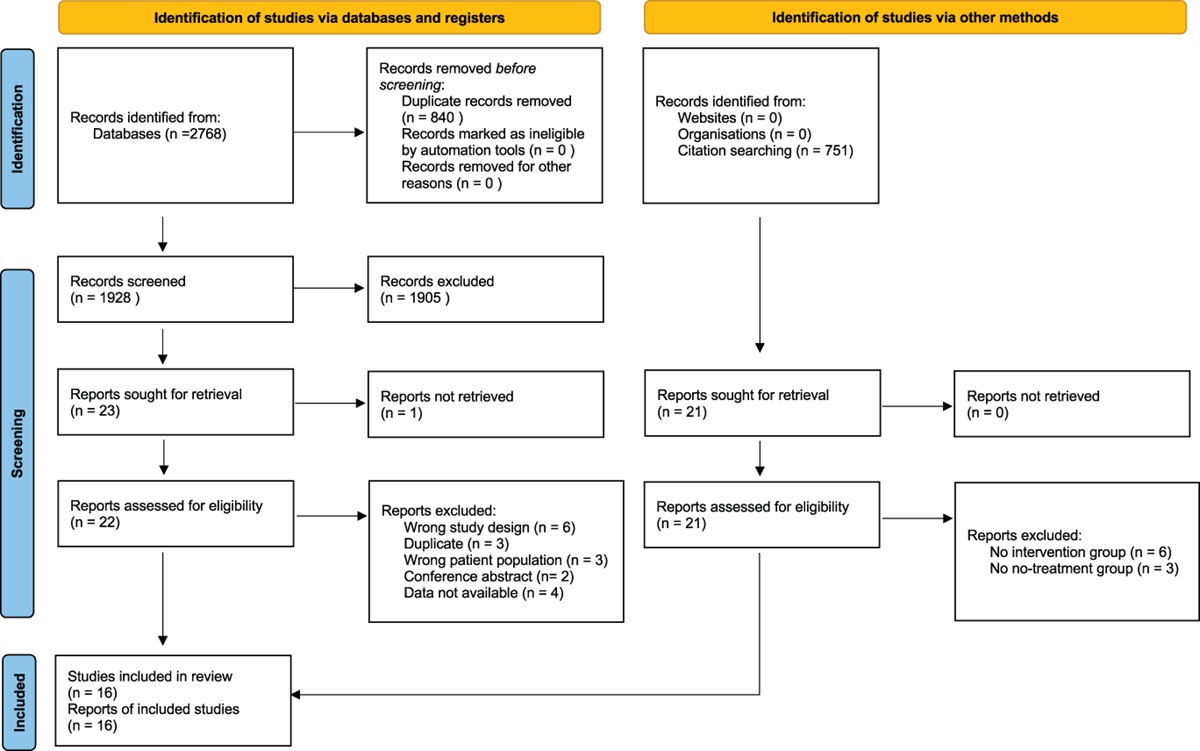
3.3. Evidence for candidate measuresThe evidence base for making recommendations for the candidate measures for each outcome domain was summarized by incorporating multiple sources of information, including systematic reviews and focused evaluations (ie, reviewing individual articles for specific measurement properties for measures) of non-PROMIS and PROMIS pediatric measures, feedback from the Core-OPPP steering committee, and an updated literature review (see Fig. 2 for the flow diagram of the process for evidence gathering). The list of candidate measures was further reduced to a few of the most promising measures for each domain, with the pros and cons highlighted to guide the final expert consensus. Tables 3–8 provide detailed evidence for measure selection for each COS domain.
 Figure 2.:
Figure 2.: Flow diagram for gathering evidence regarding measurement properties of the identified candidate measures for each core outcome domain of the core outcome set (COS) for pediatric chronic pain clinical trials.BAPQ, bath adolescent pain questionnaire; BASC, Behavior Assessment System for Children; BPI, Brief Pain Inventory; CALI, child activity limitations interview; CBCL, Child Behavior Checklist; CDI, Children's Depression Inventory; COSMIN, consensus-based standards for the selection of health measurement instruments; FDI, Functional Disability Inventory; FPSR, Faces Pain Scaley–Revised; GAD, generalized anxiety disorder; MASC, Multidimensional Anxiety Scale forChildren; NRS, numerical rating scale; PCS, pain catastrophizing scale; PHQ, Patient Health Questionnaire; PROMIS, Patient-Reported Outcome Measurement Information System; RCADS, Revised Children's Anxiety and Depression Scale; RCMAS, Revised Children's Manifest Anxiety Scale; SCARED, screen for Child Anxiety-Related Disorders; VAS, visual analogue scale.
Table 3 - Candidate measures for pain severity. Measure Age range Pros Cons Additional notes Parent proxy Key references Numeric Rating Scale (0-10 NRS) 6-18 y Widely usedVisual analogue scale (VAS) is not considered because the administration is variable and relatively burdensome; Faces Pain Scale–Revised (FPS-R) is not considered because it is less commonly used among adolescents.
IRT, item response theory; PROMIS, Patient-Reported Outcomes Measurement Information System.
ICC, intraclass correlation coefficient; PROMIS, patient-reported outcomes measurement information system.
PROMIS Pediatric Life Satisfaction is not considered because of the lack of validation among pediatric populations with chronic pain, poor concept fit, and inadequate understanding in younger children.
ICC, intraclass correlation coefficient; PedsQL, pediatric quality-of-life inventory; PROMIS, Patient-Reported outcomes measurement information system.
PROMIS Pediatric Anger is not considered due to inadequate measurement properties and poor fit with emotional functioning.
AUC, area under the curve; CAT, computer adaptive testing; CDI, Children's Depression Inventory; ICC, intraclass correlation coefficient; JIA, juvenile idiopathic arthritis; MID, minimally importance difference; MSK, musculoskeletal; PROMIS, Patient-Reported Outcomes Measurement Information System; RCI, reliable change index; SCD, sickle cell disease.
留言 (0)