Today, the importance of cancer is becoming more significant. Despite all new treatment approaches, death from cancer is still the second cause of all deaths in developed countries [12, 13]. Among women, breast cancer (BC) is the most fundamental reason for cancer-related deaths [14]. It has been known that women with BC cases in their families have a higher risk of BC development. Furthermore, it has been shown that genetic predisposition is an essential factor for breast, ovarian, colon and some other types of cancer [15]. While ovarian cancer has a lower prevalence compared to breast cancer, its lethality surpasses it by threefold. Projections suggest a significant increase in the mortality rate of ovarian cancer by 2040. This heightened mortality is attributed to the asymptomatic and indolent growth of tumors, delayed symptom onset and the absence of effective screening methods leading to diagnoses at advanced stages. Consequently, ovarian cancer has earned the moniker “silent killer” [16]. Our knowledge about the etiology of familial ovarian cancer has increased as we defined the mutations of tumor suppressor genes on BRCA1 and BRCA2 in hereditary breast/ovarian cancer patients and by determining the DNA wrong coupling repair genes such as MSH2 and MLH1 in Lynch syndrome. It is reported that the mutations in BRCA1 and BRCA2 genes are responsible for 90% of familial ovarian cancer cases, and individuals carrying these mutations possess 60–70% more risk for ovarian cancer throughout their life span [11].
Changes in the BRCA1/BRCA2 in 350 Swedish breast–ovarian cancer patients and a control group consisting of 70 individuals with no familial or separate breast–ovarian cancer were examined in a study with DHPLC due to its effectiveness and speediness. Eventually, 80 previously defined mutations (51 in BRCA1, 29 in BRCA2), 61 clinically significant unknown changes (36 in BRCA1, 25 BRCA2) and 23 new mutations (2 meaningless, 12 wrong meaningful, three frameshifts, six intronic changes) were observed. Because two of the newly detected changes were more than 1% in the control group, these changes were evaluated as polymorphism [17].
DHPLC investigated mutations in the BRCA1 and BRCA2 genes in a study conducted in Korea with 1020 BC patients and 167 control subjects without a familial history of breast cancer. Again, we see that the DHPLC method was used in this study because the individual number was high, facilitating the procedure. Consequently, 78 mutations were observed. These changes were 14 deletions, 38 wrong meaningful and 26 polymorphisms. Three of the 14 deletions were reported as new mutations in the BRCA1, and three were reported as new mutations in the BRCA2. Two of the newly detected changes were found to be more than 1% in the control group, and therefore, they were evaluated as polymorphism [18].
In the previous study that was conducted in our department, all exons of both genes were scanned with protein truncation test (PTT) and denaturing gradient gel electrophoresis (DGGE) methods in the DNA of 75 patients, including 26 familial breast and/or ovarian cancer patients, six bilateral BC patients, three breast and ovarian cancer patients, 32 early-stage BC patients, five early-stage ovarian cancer patients and three male BC patients. The missense mutations, polymorphisms and intronic region changes of these genes, whose biological significance was unknown entirely, and first-detected modifications were found. These seven detected changes were H513L, H816P and S1577Y changes in the BRCA1 gene and S326R, G258P, E2903K and N2742S changes in the BRCA2 gene [11].
Despite having this knowledge about these changes, more studies are necessary with healthy individuals to understand whether these changes are polymorphisms specific to the Turkish population or pathological mutations. DNA samples from 150 healthy women individuals with a clear familial cancer history were studied in the present study to determine this. When the threshold value between mutation and polymorphism is taken as 1%, the DNA sequence alterations seen in 1% or more than 1% of the population are referred to as polymorphism; on the other hand, when they are detected in less than %1 of the population, they are called a mutation. According to this information, in this study conducted with a control group of 150 individuals, the H513L, H816P and S1577Y changes were not detected in the BRCA1 gene, and S326R, G258P, E2903K and N2742S changes in the BRCA2 gene. Hence, their incidence is less than 1%, and they have not been mentioned in the literature before. As a result, it is possible to argue that these are the new mutations observed for the first time.
A study was conducted in Turkey on BRCA1 and BRCA2 genes with only some exons in 53 familial BC and 52 early-stage breast cancers in 105 Turkish women. In this study, the exons 2, 11, 14 and 20 of the BRCA1 and exon 11 of the BRCA2 gene were scanned with PTT (protein truncation test) or the heteroduplex analysis. In the BRCA1 gene, two 5382 insC mutations were detected—one in breast cancer and one in ovarian cancer patients. Also, in the BRCA1 gene 1623delTTAAA, 2139delC, 3819delGTAAA, 247delT, 4508delC, IVS-14 + 1delG mutations and in BRCA2 5295insC, 6656delC mutations were spotted in each of the different individuals [19]. In another study, exons 2, 5, 11, 13, 20 and 24 of the BRCA1 gene and exon 11 of the BRCA2 gene were scanned in 6 hereditary, seven familial, 27 early-stage and ten males with high-risk breast or ovarian cancer in a total of 50 Turkish individuals. In 23 individuals, in addition to previously defined changes, five different polymorphisms, 3034delAAAC and 6880insG mutations in the BRCA2 gene of 2 individuals and other patients 1201insA and 2080A--> G mutations in the BRCA1 gene were spotted [20].
Studies that focus on all exons of BRCA1 and BRCA2 are insufficient. In one study, all exons of BRCA1 and BRCA2 genes of 15 individuals with high-risk group breast and/or ovarian cancer were scanned with PTT or CSGE (Conformation Sensitive Gel Electrophoresis), and 3414delTCAG mutation of BRCA2, 5622C--> T and 5382insC mutations of BRCA1 were spotted [21]. In another study on 15 familial and 87 non-familial ovarian cancer patients, mutation scanning of these genes was performed using the PTT method. The results showed mutations in 17 individuals [22]. Another study with 87 breast and/or ovarian cancer patients was carried out with DNA sequence analysis; and 5382insC mutation and a new polymorphism (3663C--> A) in the BRCA 1 gene, two new mutations (9329insC and 9934insG), a new intronic polymorphism 7069 + 41(TTTT-- > AAAG) and an early reported polymorphism (1093A--> C) were found [23].
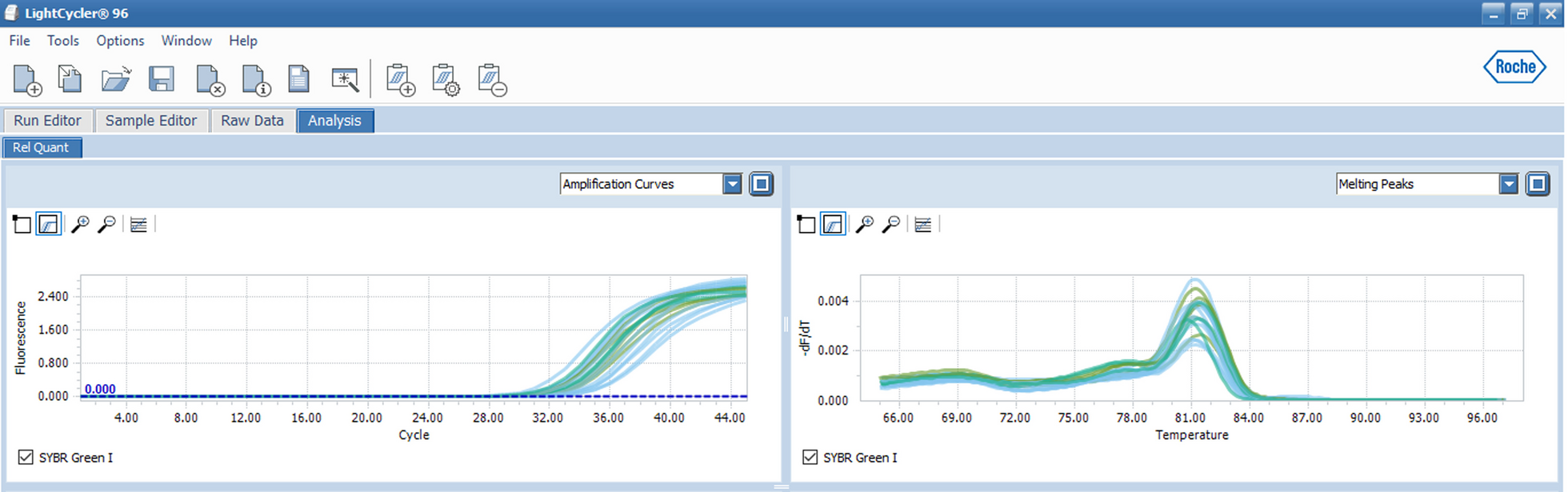
In this study, DHPLC was used due to its effectiveness. First, samples representing different peaks were analyzed again using the same experimental conditions as the present study. After this second analysis, for the samples still representing other peaks, the PCR, denaturation and hybridization processes were repeated and worked with the DHPLC device again. At the same time, the working conditions of the device were optimized by cooling the room temperature. The device may face a problem while studying the samples. The DHPLC device is a sensitive tool. When the temperature of the working environment is high, the stability of the device might deteriorate, and different peaks can be obtained. Another reason for different peaks can be the incorrect mixing of the test samples and reference samples with different amounts. Different peaks might also be observed if the PCR protocol is not optimized well.
Recent studies have detected that de novo mutations of BRCA1 and BRCA2 are increasing; therefore, correctly defining the molecular scanning strategies is becoming more critical. Necessary studies must be carried out on the other members of mutation-detected individuals or families, physicians must be informed and provided with the results of these studies, and an entirely correct genetic consultation must be served by defining all risks.
Because of the location of our country and the lack of funding mutations as in other hereditary diseases, it is crucial for early diagnosis and treatment to screen for changes in these genes in breast, ovarian and prostate cancer risk groups with the DHPLC method, which is a reliable method, and to provide counseling after the risks are determined. Furthermore, when it is considered that new mutations related to these genes will continue to be found for the first time in our population, which is a heterogeneous society, we think it would be helpful to include control groups in future studies.

留言 (0)