
記住我



Hip fractures are some of the most common fractures encountered by orthopaedic trauma surgeons, with nearly 18% of women and 6% of men sustaining at least one in their lifetime.1,2 Globally, the yearly incidence of hip fractures is expected to rise to 4.5 million.1 These fractures most commonly occur at the femoral neck and in the intertrochanteric region.1 Currently, geriatric intertrochanteric fractures alone have an incidence of more than 150,000 per year in the United States, with a total healthcare cost burden of $6 billion yearly.3 In addition, between 6 and 60% of people who suffer from hip fractures require a stay at a long-term care facility, adding between $19,000 and $66,000 to their healthcare costs.1
In the current culture of value-based care, cost reduction is a priority. Value, as defined by Porter,4 is the patient outcomes per cost of care episode. An analysis of the cost of care for inpatient stay after geriatric intertrochanteric (IT) femur fractures demonstrated high variability among patients but averaged nearly $20,000 per patient.3 As implant costs have a linear correlation with total inpatient cost of care, implant cost reduction has become a prime target for cost containment in orthopaedic trauma.3
One way to reduce implant costs is the utilization of generic orthopaedic implants. In the United States alone, there is an average over $254 billion cost savings annually with the use of generic medications.5 Price decay after patent expiration often stabilizes at around 2 to 10% of the original drug cost over 3 years.5 With the $5.3 billion orthopaedic trauma implant market steadily growing,6,7 the implementation of generic implant use in this field presents a great opportunity for cost savings while maintaining the same standard for patient outcomes.
The purpose of this study was to compare 6-month outcomes and implant costs of intertrochanteric and subtrochanteric fracture fixation using cephalomedullary nails (CMNs) from a single name-brand vendor with fixation using generic CMNs. All patients were treated by a single surgeon at a single institution in a metropolitan area. The primary outcomes include implant cost and 6-month all-cause mortality, all-cause morbidity, and revision surgery rates. We hypothesize that there will be no notable difference in 6-month all-cause mortality, revision surgery, and all-cause complication rates between those treated with generic and brand CMNs.
MethodsThis retrospective matched cohort study was deemed to be exempt by the Institutional Review Board because of its observational nature. All acute, low-energy IT, or subtrochanteric fractures with CMN fixation from 2021 to 2022 at a single institution performed by a single surgeon were identified using current procedural terminology codes. Exclusion criteria were age <60 years, polytrauma, and history of prior trauma to the affected hip. After preliminary analyses, nearest neighbor 1:1 matching was conducted between patients with name-brand and generic implants based on (1) age, (2) American Society of Anesthesiologists (ASA) score, and (3) Charlson Comorbidity Index (CCI).
A total of 50 patients met inclusion criteria for this matched cohort study (25 name-brand versus 25 generic). Patient demographics including age, sex, BMI, ASA score, CCI, and fracture laterality were extracted through chart review of the electronic medical record (EMR) for each patient. CCI was chosen because it has been shown to have good correlation with other comorbidity indices, has excellent inter-rater reliability, and has demonstrated predictive validity.8,9 Outcomes of interest including all-cause mortality, complication rates, and revision surgery rates each at 90 days and 6 months were also collected through an EMR review. Fracture and fixation characteristics including Orthopaedic Trauma Association/AO Foundation classification, stability of fracture pattern, subtrochanteric extension, and calculated tip-apex distance (TAD) were determined based on preoperative and postoperative imaging. Surgical characteristics including time to surgery, surgical time, and type of anesthesia were obtained from the surgical note. Implant characteristics including implant company, implant model, and length of CMN were extracted from the patient EMR. Implant characteristics were then cross-referenced with the institutional chargemaster database to obtain accurate implant cost data. Disposable implant (ie, drill bits) information and cost for each procedure were also obtained from the institutional chargemaster database.
Statistical analysis was performed using Microsoft Excel (version for Microsoft 365; Redmond, WA) and Intellectus Statistics (Clearwater, FL). Descriptive statistics were provided for continuous and categorical variables and filtered by the implant company. Chi-square tests, Fisher exact tests, independent sample t-tests, and Mann-Whitney U-tests were conducted as appropriate to identify outcome and covariate differences between manufacturing cohorts. Statistical significance was defined as an alpha value ≤ 0.05.
ResultsA total of 50 patients were included in this matched cohort study; 37 were female (74%). The average age was 80.2 ± 9.9 years, and the average BMI was 24.2 ± 5.7. The average CCI was 1.2 ± 1.1. Fifteen patients had an ASA score of 2 (30%), with the rest having an ASA score of 3 (35, 70%). There were no statistically significant differences in age, CCI, and sex between the two cohorts (P = 0.588, P = 0.260, and P = 0.107, respectively) (Table 1). BMI did differ markedly between the two groups with an average BMI of 22.5 ± 4.9 for the generic cohort and 26.0 ± 6.0 for the name-brand cohort. Over the 6-month follow-up period, five patients (10%) returned to the emergency department for repeat falls with one patient refracturing the affected hip and one patient sustaining a fracture contralateral to the initially affected hip. There were 10 deaths within the 6-month follow-up period, with six of those deaths happening within the first 90 days after surgery.
Table 1 - Patient Demographics for Generic and Name-Brand CMN Cohorts (N = 50) Variable Name Brand (n = 25) Generic (n = 25) P Age (years) 81.0 ± 8.9 79.5 ± 11.0 0.588 Sex 0.107 Male 4 (16.0%) 9 (36%) Female 21 (84.0%) 16 (64%) BMI 26.0 ± 6.0 22.5 ± 4.9 0.027 CCI 1.4 ± 1.2 1.0 ± 1.1 0.260 ASA score 0.768 2 8 (32.0%) 7 (28%) 3 17 (68.0%) 18 (72%)ASA = American Society of Anesthesiologists, CMN = cephalomedullary nail, BMI = body mass index, CCI = Charlson Comorbidity Index.
Continuous variables are presented as mean ± S.D. Categorical variables are presented as N (%).
Bolded text indicates statistical significance.
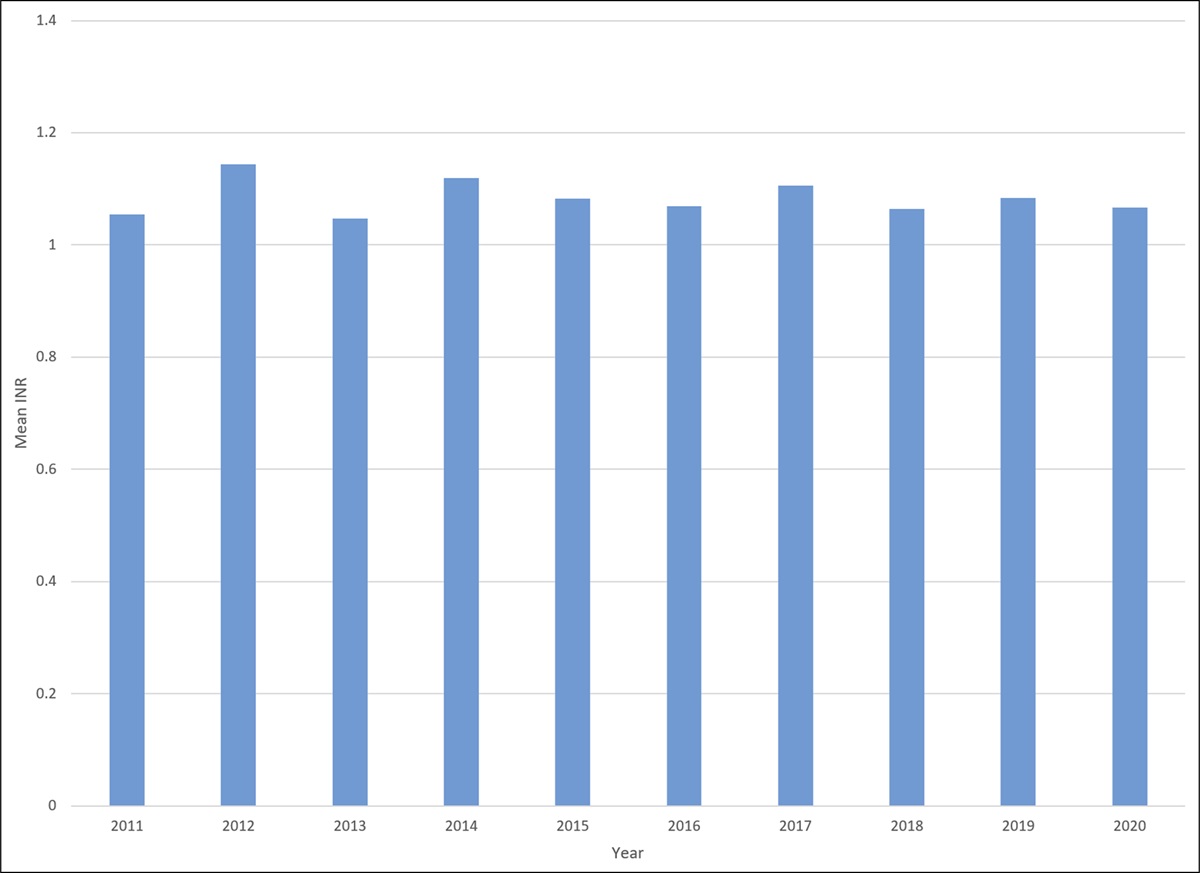
The most common type of fractures as classified by the Orthopaedic Trauma Association/AO Foundation classification system was 31A2 (30, 60%), followed by 31A1, 32A2, and 32B3(Figure 1). Seventy percent of the patients in this study had unstable fractures, with five patients (10%) having subtrochanteric fractures and 5 (10%) having subtrochanteric extension. Most patients (41, 82%) received intermediate-length CMNs with only 6 (12%) receiving long CMNs and 3 (6%) receiving short CMNs. The average cost for a generic CMN was $1614.56 ± $29.92 while a name-brand implant cost $3586.54 ± 105.31 on average (Figure 2). Disposable costs (costs of devices necessary for the procedure, but not implanted in the patient, ie, drill bit) also contributed to overall device cost variation between the two cohorts. The average cost of all disposables for a case using generic instrumentation was $108.72 ± 70.85 as contrasted by the costs of disposables for name-brand implant sets which averaged $916.36 ± 141.14 (Table 2). The average total cost difference between procedures in which generic instruments and implants were used and those using name-brand products was $2765.02 (Figure 3).
 Figure 1:
Figure 1: Graph showing distribution of fracture patterns between name-brand and generic implant fixation cohorts. AO Foundation/Orthopedic Trauma Association
 Figure 2:
Figure 2: A, Radiographs showing implanted name-brand long intramedullary nail. B, Radiographs showing implanted generic long intramedullary nail.
Table 2 - Implant, Disposable and Total Implant Costs for Generic and Name-Brand Systems Generic Name Brand P Cephalomedullary naila Short (n = 3) $1610 $3551.50 n/ab Intermediate (n = 41) $1610.81 ± 25.10 $3595.30 ± 116.64 <0.001 Long (n = 6) $1658.50 ± 65.89 $3551.50 ± 0.0 0.016 Disposables $108.72 ± 70.85 $916.36 ± 141.14 <0.001 Total average cost per case $1723.28 ± 84.78 $4488.30 ± 179.94 <0.001Continuous variables are presented in mean ± S.D. Categorical variables are presented in N (%).
Bolded text indicates statistical significance.
aShort = 170-195 mm, intermediate = 200-235 mm, long ≥ 235 mm.
bSample size too small to assess statistical significance.
 Figure 3:
Figure 3: Graph showing average cost of implants and disposables for each cohort. There is a statistically significant difference between name-brand and generic average costs for both disposables and implants.
Distribution of fracture patterns did not differ significantly between the two cohorts (P = 0.238) (Figure 1). There were no notable differences in 90-day and 6-month mortality, complications, and reoperations between the two cohorts (Table 3). Patients with generic implants had larger TAD than their counterparts with name-brand implants (20.7 ± 7.0 mm name-brand versus generic: 25.1 ± 4.0 mm; P = 0.043) although this did not correlate with worse outcomes in the cohort that received generic implants. There were two skin and soft-tissue infections occurring during the study period, one in each cohort. One nonunion occurred during the study period and was suffered by a patient who received a name-brand implant.
Table 3 - Matched Cohort Outcomes After CMN Fixation (N = 50) Variable Name Brand (n = 25) Generic (n = 25) P Tip-to-apex distance (mm) 20.7 ± 7.0 25.1 ± 4.0 0.043 Nonunion 1 (4.0%) 0 (0.0%) 1.000 90-day mortality 3 (12.0%) 3 (12.0%) 1.000 90-day revision surgery 2 (8.0%) 0 (0.0%) 0.490 90-day complication 3 (12.0%) 3 (12.0%) 1.000 6-month mortality 4 (16.0%) 6 (24.0%) 0.725 6-month revision surgery 2 (8.0%) 1 (4.0%) 1.000 6-month complication 3 (12.0%) 3 (12.0%) 1.000CMN = cephalomedullary nail
Bolded text indicates statistical significance.
Continuous variables are presented as mean ± S.D. Categorical variables are presented as N (%).
The purpose of this retrospective matched cohort study was to compare 6-month outcomes and implant costs of intertrochanteric and subtrochanteric fracture fixation using CMNs from a single name-brand vendor to fixation using generic CMNs. We hypothesized that there would be no notable difference in 90-day and 6-month mortality, complication, and revision surgery rates between the two cohorts despite notable differences in implant cost. Ninety-day and 6-month mortality between the two cohorts did not differ significantly (P = 1.000 and P = 0.725, respectively). Both reoperations that occurred within 90 days of initial fixation were on patients that received name-brand fixation, although this did not reach statistical significance. Overall complication rates between the two groups were identical at 12.0% over the 6-month episode of care. The average implant cost difference between the two cohorts was $1971.98 per case.
The literature comparing outcomes between generic and name-brand orthopaedic implants has been few and far between until the past decade. In a recent retrospective analysis of patients receiving fixation for peritrochanteric fractures, there was a significantly higher incidence of postoperative infections in patients who received name-brand CMNs (P = 0.045).6 A similar retrospective study analyzing fixation with generic implants for clavicle, proximal humerus, distal radius, proximal tibia, tibial pilon, and ankle fractures found no differences in infection rates between generic and name-brand implant fixation for any of the studied fracture locations.10 Our study found similar findings, with no statistically significant difference in postoperative infections between the two cohorts.
Overall cost-savings with the use of generic orthopaedic implants is reported to be anywhere from 30 to 80% depending on institutional prices and implant type.6,10–14 The total cost of name-brand CMNs is reported to be 38% greater than that of a generic implant.6 This study demonstrates an average difference of nearly $2,000 between name-brand and generic CMNs, which represents a 55.0% potential cost-savings with the implementation of generic CMN utilization while maintaining the same standard of care and excellent patient outcomes.
Cost of disposable items and devices used in surgery contribute to the great variability in total surgical costs. These items, such as guidewires, drill bits, and bone taps, can cost over $100 each, with several being one-use items.15 This study found notable difference in disposable item costs between generic and name-brand implant systems. The average per-case difference in disposable item costs between manufacturers was $807.64 (P < 0.001). When totaled with the implant cost difference between the systems, the overall cost difference reached an average of $2765.02. Utilization of generic implants and disposables instead of name-brand items can lead to a 61.6% cost reduction.
This study has many strengths and weaknesses. One strength of this study is the ability to pull implant cost data directly from the institutional chargemaster database for each case, allowing for accurate implant price representation. Another strength is that cohorts were matched by age, ASA, and CCI which present a unique opportunity for more accurate comparison between the two groups by accounting for several comorbidities. Weaknesses include the small cohort size, limited follow-up time, retrospective nature of the study, different BMI averages between the two cohorts, and limited generalizability of the study population to a broader orthopaedic population. Furthermore, power analyses for a two proportions z-test indicate a required minimum sample size of 64 (32 in each cohort) to yield a power of 0.8 with an alpha of 0.05 and a medium effect size, thus nonunion rate comparison between the two cohorts should be interpreted cautiously. The post hoc analysis comparing the observed nonunion rate in our study (4%) with the literature-reported rate (0.7%) did not reveal a statistically significant difference (P > 0.05).16 While our study demonstrated a higher proportion of nonunion cases, it is important to note that the analysis lacked the required statistical power (power = 0.466) to detect smaller differences. This emphasizes the need for larger sample sizes in further investigations within this domain. In addition, there was a notable difference in TAD between the two cohorts. Although there were no notable differences in outcomes, this begs the question of system ease of use. After discussion with the represented surgeon, they stated that they felt each system was equally user-friendly, though there was a bit of a learning curve with beginning use of a new system that they felt likely accounted for the difference in TAD. Future studies should aim to address long-term outcomes and perform randomized prospective analysis of generic CMN utilization and outcomes.
This retrospective matched cohort study compared 6-month outcomes and implant costs of intertrochanteric and subtrochanteric fracture fixation using CMNs from a single name-brand vendor to fixation using generic CMNs. We demonstrated equivalent 90-day and 6-month outcomes for patients that sustain IT and subtrochanteric femur fractures with generic and name-brand fixation while presenting an opportunity for cost savings on implants and disposable devices averaging over $2,000 per case.
References 1. Veronese N, Maggi S: Epidemiology and social costs of hip fracture. Injury 2018;49:1458-1460. 2. Tanner DA, Kloseck M, Crilly RG, Chesworth B, Gilliland J: Hip fracture types in men and women change differently with age. BMC Geriatr 2010;10:12-14. 3. Casnovsky L, Blaschke BL, Parikh HR, et al.: Does implant selection affect the inpatient cost of care for geriatric intertrochanteric femur fractures? Geriatr Orthop Surg Rehabil 2020;11:2151459320959005. 4. Porter ME: What is value in health care. N Engl J Med 2010;363:2477-2481. 5. Uzoigwe CE, Shoaib A: Patents and intellectual property in orthopaedics and arthroplasty. World J Orthop 2020;11:1-9. 6. Khoo KM, Kim GW, Lindvall EM, Martirosian AK: Outcomes and cost comparison between generic and conventional cephalomedullary nails in the treatment of peritrochanteric femur fractures. J Am Acad Orthop Surg 2022;30:119-124. 7. Lybrand KE, Althausen PL: The role of value-based implants in orthopedic trauma. Orthop Clin North America 2018;49:437-443. 8. Roffman C, Buchanan J, Allison G: Charlson comorbidities index. J Physiother 2016;62:171. 9. Charlson ME, Carrozzino D, Guidi J, Patierno C: Charlson comorbidity index: A critical review of clinimetric properties. Psychother Psychosom 2022;91:8-35. 10. McPhillamy A, Gurnea TP, Moody AE, Kurnik CG, Lu M: The clinical and economic impact of generic locking plate utilization at a level II trauma center. J Orthop Trauma 2016;30suppl 5:S32-S36. 11. Atrey A, Heylen S, Gosling O, Porteous M, Haddad F: The manufacture of generic replicas of implants for arthroplasty of the hip and knee: Is it regulated and will it save money? Bone Joint J 2016;98-B:892-900. 12. Egol KA, Capriccioso CE, Konda SR, et al.: Cost-effective trauma implant selection: AAOS exhibit selection. J Bone Joint Surg Am Vol 2014;96:e189. 13. Gurnea T, Swanson D, Bryan J, Shul C: The clinical and economic impact of high value external fixation utilization at a level II trauma center. J Orthop Exp Innov 2021 January 21. 14. Althausen PL, Kurnik CG, Shields T, et al.: Clinical and economic impact of using generic 7.3-mm cannulated screws at a level II trauma center. Am J Orthop 2014;43:405-410. 15. Wetzel RJ, Kempton LB, Lee ES, Zlowodzki M, McKinley TO, Virkus WW: Wide variation of surgical cost in the treatment of periarticular lower extremity injuries between 6 fellowship-trained trauma surgeons. J Orthop Trauma 2016;30:e377-e383. 16. Amer KM, Congiusta DV, Smith B, et al.: Cephalomedullary nailing has a higher reoperation rate compared to sliding hip screw fixation in the treatment of intertrochanteric femur fractures: A systematic literature review and meta-analysis. Arch Bone Joint Surg 2023;11:595-604.
留言 (0)