
記住我



Two common causes of shoulder pain, pathology of the rotator cuff and the long head of the biceps tendon (LHBT), often present together in the same patient.1–4 The LHBT is susceptible to various pain-generating conditions, such as tendinopathy, tearing, and subluxation.5 There remains a lack of consensus regarding the best treatment option for addressing LHBT-related pain, especially in patients with concomitant rotator cuff pathology.6 Current treatment options for LHBT-related pain include nonsurgical management, tenotomy, or tenodesis.7 A comparison between tenotomy and tenodesis has shown mixed results, with similar outcomes reported for both procedures.8 Tenotomy has been associated with higher rates of cramping and cosmetic deformity, whereas biceps tenodesis (BT) has been found to have satisfactory outcomes through either an arthroscopic or open approach.9 Reported disadvantages of tenodesis include higher healthcare costs and a lack of consensus on the ideal surgical technique.10–13 In addition, although rare (<1%), complications specific to tenodesis have been reported including loss of fixation, infection, hematoma, and complex regional pain syndrome.13
The incidence of subsequent procedures after isolated rotator cuff repair (RCR) remains high. One study found that 14.3% required a distal clavicle resection and 8.1% of patients required a BT/tenotomy at a mean of 24 ± 27 months after isolated RCR.14 To decrease the burden of revision surgeries after RCR, there has been increasing interest in optimizing RCR procedures and addressing concomitant pathologies at the time of the index surgery.15 Nonetheless, previous research has shown mixed results. Some studies have shown higher revision surgery rates in patients undergoing RCR with BT compared with patients undergoing RCR without BT,6,15 whereas others have shown no difference in revision surgery rates at all.16 However, these studies were limited to a 1- to 2-year postoperative period. It has been demonstrated that 49% of patients who underwent RCR without concomitant BT demonstrate sonographic evidence of degenerative damage to the LHBT 1 year postoperatively.17 Therefore, concomitant BT may provide benefits in reducing revision surgery rates in the long term that are not apparent after 1 to 2 years.
There is a paucity of literature observing revision surgery rates beyond the 1-year postoperative window after RCR. Therefore, the purpose of this study was to use a national administrative database to compare 4-year ipsilateral revision surgery rates between patients undergoing primary RCR with BT and those without BT. We hypothesized that concomitant BT would be associated with lower 4-year revision surgery rates when compared with RCR without BT.
Methods Study DesignThe Mariner data set from the PearlDiver Database (10435 Marble Creek Circle Colorado Springs, CO 80908A) was used to conduct a retrospective cohort analysis. The data set consists of all-payer medical and prescription claims records for more than 150 million patients from 2010 to 2021. This data set uniquely tracks patients using distinct patient identifiers that are not influenced by changes in insurance providers, allowing for the analysis of long-term follow-up data. The methodology of this study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines for cohort studies. This study was reviewed by our institution's IRB and deemed to be exempt from IRB review (IRB #00387181) because no patient-identifying information was used.
Patient SelectionPatients who underwent primary open or arthroscopic RCR were identified using current procedural terminology (CPT) codes (Appendix A, https://links.lww.com/JG9/A329). To confirm the laterality of the index procedure, CPT codes for primary open or arthroscopic RCR were matched with laterality-specific International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes for rotator cuff tears on the day of the index surgery. Patients were only included in the analysis if they had a single, unilateral ICD-10 rotator cuff tear diagnosis on the day of surgery, thus confirming the laterality of the RCR performed. International Classification of Diseases, Ninth Revision (ICD-9) codes were not used as part of the inclusion criteria because they do not specify laterality. Those undergoing open (CPT-23430) or arthroscopic (CPT-29828) BT on the same day as the primary RCR were then identified.
Subjects who met any of the following criteria were excluded from this study: (1) 18 years or younger, (2) history of prior RCR, (3) bilateral surgery, (4) coexisting diagnosis of contralateral rotator cuff pathology, and (5) less than 4-year follow-up. To account for both 4-year minimum follow-up and the use of laterality-specific ICD-10 codes (which were implemented in the United States in 2015), our PearlDiver query was run from 2015 to 2017. Patients with bilateral rotator cuff tear ICD-10 codes were excluded to both ensure the laterality of the index procedure and ensure that any subsequent revision surgeries were done on the ipsilateral shoulder as the primary procedure. Patients were also stratified according to the approach and concomitant procedures performed during their index operation into four cohorts: open RCR with BT, open RCR without BT, arthroscopic RCR with BT, and arthroscopic RCR without BT. Shoulder revision surgeries were identified using CPT codes reported in Appendix A, https://links.lww.com/JG9/A329. To confirm the laterality of the revision surgery procedure, CPT codes for each respective revision surgery were again matched with laterality-specific ipsilateral ICD-10 diagnosis codes.
Demographic and Outcome VariablesDemographic variables included age and sex. Comorbidities were identified using ICD-10 codes relevant to the Elixhauser Comorbidity index. The primary study outcome was the incidence of 4-year revision surgery including revision RCR, BT, tenotomy/débridement, distal clavicle excision, arthroplasty, all-cause revision, and other scope procedures. Secondary outcomes included 90-day surgical site infection, nerve injury, wound complications, hematoma, and adhesive capsulitis.
Statistical AnalysisDemographics, comorbidities, and revision surgeries were initially analyzed with univariate analysis using X2 and Student t-tests where appropriate. A Number Needed to Treat (NNT) analysis was conducted for all univariate outcomes by dividing 1 by the absolute difference in incidence rates between the two cohorts being compared. Multivariable analysis was subsequently done using a logistic regression. Age, sex, and all comorbidities with a P-value <0.2 on univariate analysis were included as independent variables on multivariable analysis to control for confounders. Output from the logistic regression analysis was reported as odds ratios, 95% confidence interval (95% CI), and P-values. A P-value <0.05 was regarded as statistically significant. All statistical analysis was conducted using R software, Vienna, Austria, which is provided by the PearlDiver Database.
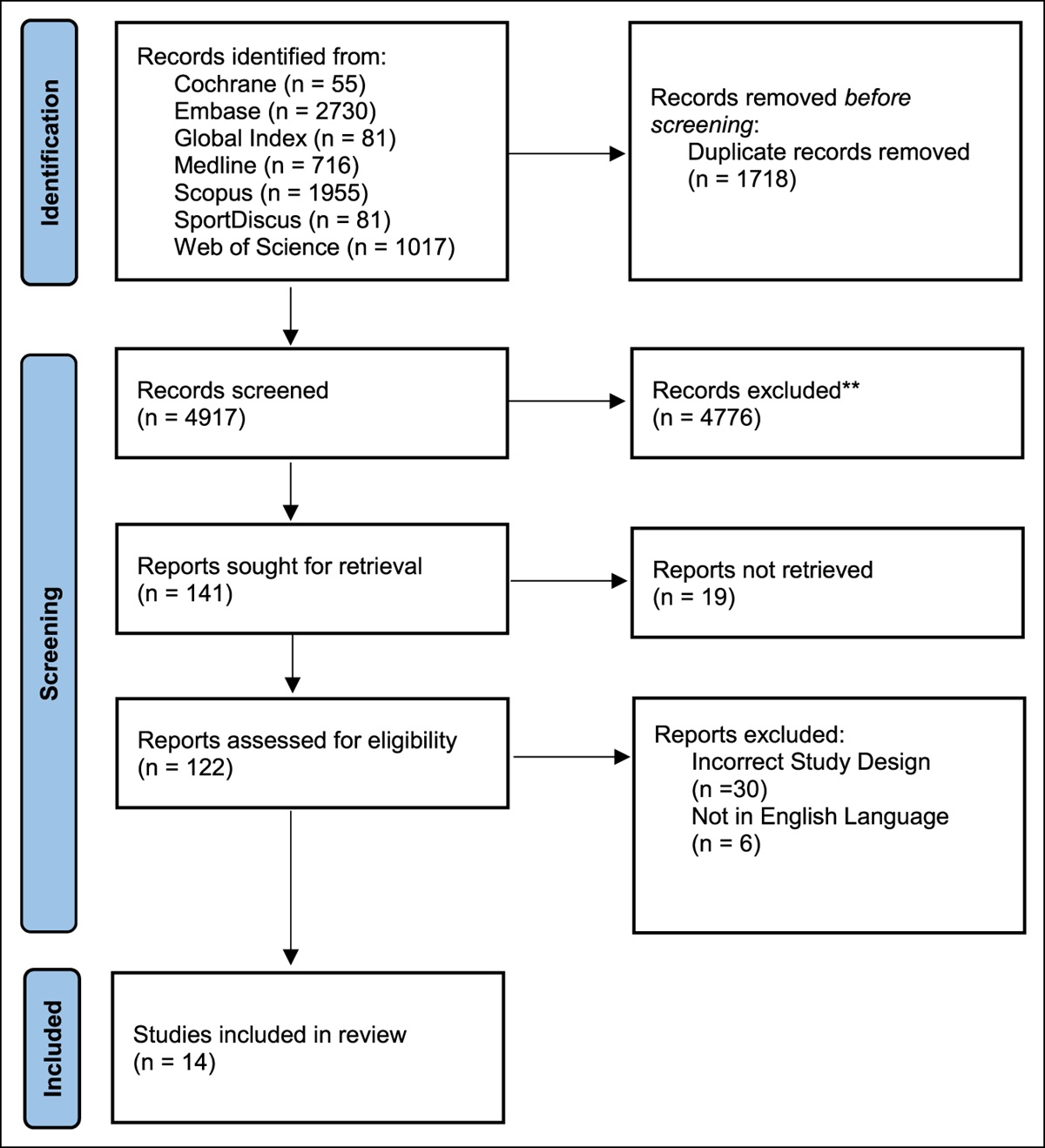
Results Patient PopulationIn total, 131,155 patients who underwent primary RCR met the inclusion criteria for our analysis. Of those, 24,487 (18.7%) underwent concomitant BT and 106,668 (81.3%) did not. Of those who received arthroscopic RCR, 20,302 (19.1%) received concomitant BT and 86,067 (80.9%) did not. Of those who received open RCR, 4185 (16.9%) received concomitant BT and 20,601 (83.1%) did not (Figure 1).
 Figure 1:
Figure 1: Study population flowchart
Demographics and ComorbiditiesPatients who underwent RCR with concomitant BT were significantly older (P < 0.001) and more likely to be male (P < 0.001). In addition, these patients were less likely to have congestive heart failure (P = 0.002), paralysis (P = 0.015), chronic pulmonary disease (P = 0.023), hypothyroidism (P = 0.003), peptic ulcer disease (P = 0.024), anemia (P = 0.004), depression (P = 0.012), and obesity (P = 0.003) when compared with those without concomitant BT (Table 1).
Table 1 - Demographics and Comorbidities RCR with BT n = 24,487 RCR without BT n = 106,668 P Demographics Average age, mean (SD) 60.38 9.3 60.02 9.9 <0.001 Sex Male 13,806 56.4% 54,243 50.6% <0.001 Female 10,681 43.6% 52,425 49.2% Comorbidities Congestive heart failure 340 1.4% 1783 1.7% 0.002 Arrhythmias 1436 5.9% 6510 6.1% 0.162 Valvular disease 771 3.2% 3517 3.3% 0.247 Pulm circ disorders 185 0.8% 929 0.9% 0.083 Peripheral vascular disease 776 3.2% 3454 3.2% 0.595 Hypertension 3015 12.3% 13,390 12.6% 0.310 Paralysis 61 0.3% 374 0.4% 0.015 Other neuro disorders 308 1.3% 1349 1.3% 0.956 Chronic pulmonary disease 1533 6.3% 7108 6.7% 0.023 Diabetes mellitus 1618 6.6% 7239 6.8% 0.321 Hypothyroidism 1171 4.8% 5597 5.3% 0.003 Chronic kidney disease 499 2.0% 2366 2.2% 0.086 Liver disease 798 3.3% 3570 3.4% 0.502 Peptic ulcer disease 84 0.3% 480 0.5% 0.024 Lymphoma 42 0.8% 175 0.2% 0.864 Metastatic cancer 70 0.3% 332 0.3% 0.559 Nonmetastatic cancer 578 2.4% 2474 2.3% 0.718 Rheumatoid arthritis and CVD 799 3.3% 3466 3.3% 0.930 Coagulopathy 197 0.8% 973 0.9% 0.115 Fluid and electrolyte disorders 1054 4.3% 4858 4.6% 0.092 Blood loss anemia 113 0.5% 539 0.5% 0.407 Deficiency anemia 545 2.2% 2715 2.6% 0.004 Alcohol abuse 57 0.2% 237 0.2% 0.809 Drug abuse 372 1.5% 1720 1.6% 0.306 Psychoses 118 0.5% 516 0.5% 1.000 Depression 1671 6.8% 7772 7.3% 0.012 Smoking 1007 4.1% 4562 4.3% 0.257 Obesity 1426 5.8% 6767 6.3% 0.003RCR = Rotator cuff repair, BT = biceps tenodesis, CVD = collagen vascular disease.
Values are n (%) unless otherwise noted; significance level = 0.05 (bolded); P values approaching statistical significance (P < 0.2) were included on multivariable analysis.
No difference was observed in the incidence of 90-day surgical site infection (P = 0.360), nerve injury (P = 0.842), wound complications (P = 0.211), hematoma (P = 0.814), and adhesive capsulitis (P = 1.000) in patients who underwent RCR with concomitant BT when compared with those without concomitant BT (Table 2).
Table 2 - Univariate Analysis of 90-day Complications and 2- and 4-year Revision Surgery Rate for Rotator Cuff Repair With or Without Biceps Tenodesis RCR With BT n = 24,487 RCR Without BT n = 106,668 e Number Needed to Treat P 90-day complications Surgical site infection 78 0.3% 300 0.3% N/A 0.360 Nerve injury 2 0.01% 13 0.01% N/A 0.842 Wound complication 12 0.05% 80 0.1% 2000 0.211 Hematoma 3 0.01% 18 0.02% 10,000 0.814 Capsulitis 0 0.0% 0 0.0% N/A 1.000 All-cause revision surgery 89 0.4% 384 0.4% N/A 0.982 2-year revision surgery Rotator cuff repair 589 2.4% 3174 3.0% 167 <0.001 Biceps tenodesis 156 0.6% 785 0.7% 1000 0.107 Tenotomy/débridement 419 1.7% 2416 2.3% 167 <0.001 Distal clavicle 148 0.6% 1069 1.0% 250 <0.001 Other scope 489 2.0% 2972 2.8% 125 <0.001 Arthroplasty 205 0.8% 1115 1.1% 333 0.004 All-cause revision surgery 1124 4.6% 6214 5.8% 83 <0.001 4-year revision surgery Rotator cuff repair 672 2.7% 4074 3.8% 91 <0.001 Biceps tenodesis 173 0.7% 1168 1.1% 250 <0.001 Tenotomy/débridement 526 2.2% 3169 3.0% 125 <0.001 Distal clavicle 216 0.9% 1571 1.5% 167 <0.001 Other scope 581 2.4% 3923 3.7% 77 <0.001 Arthroplasty 300 1.2% 1643 1.5% 333 <0.001 All-cause revision surgery 1420 5.8% 8033 7.5% 59 <0.001Values are n (%) unless otherwise noted. Only patients with at least 4-year follow-up were analyzed for 4-year revision surgery rate.
After controlling for possible confounders, the utilization of concomitant BT was not associated with a significant difference in the odds of surgical site infection (OR; 95% CI; P-value [1.08; 0.84 to 1.39; P = 0.534]), nerve injury (0.71; 0.16 to 3.18; P = 0.660), wound complications (0.64; 0.35 to 1.18; P = 0.156), hematoma (0.72; 0.21 to 2.44; P = 0.593), and capsulitis (1.00; 0.00-inf; P = 1.000) within 90 days of index surgery (Table 3).
Table 3 - Multivariable Analysis of Revision Surgery After Rotator Cuff Repair With or Without Biceps Tenodesis Odds Ratio 95% Confidence Interval P 90-day complications Surgical site infection 1.08 0.84-1.39 0.534 Nerve injury 0.71 0.16-3.18 0.660 Wound complication 0.64 0.35-1.18 0.156 Hematoma 0.72 0.21-2.44 0.593 Capsulitis 1 0.00-inf 1.000 All-cause revision surgery 0.97 0.77-1.23 0.823 2-year revision surgery Rotator cuff repair 0.82 0.75-0.89 <0.001 Biceps tenodesis 0.88 0.74-1.04 0.140 Tenotomy/débridement 0.77 0.69-0.85 <0.001 Distal clavicle 0.61 0.51-0.72 <0.001 Other scope 0.73 0.66-0.80 <0.001 Arthroplasty 0.82 0.70-0.95 0.008 All-cause revision surgery 0.79 0.74-0.84 <0.001 4-year revision surgery Rotator cuff repair 0.72 0.66-0.78 <0.001 Biceps tenodesis 0.65 0.55-0.76 <0.001 Tenotomy/débridement 0.73 0.67-0.80 <0.001 Distal clavicle 0.61 0.52-0.70 <0.001 Other scope 0.65 0.60-0.71 <0.001 Arthroplasty 0.81 0.71-0.91 0.001 All-cause revision surgery 0.77 0.72-0.81 <0.001Only patients with at least 4-year follow-up were analyzed for the 4-year revision surgery rate.
Within 2 years, there was no difference in the incidence of revision BT in patients who underwent RCR with concomitant BT at their index surgery compared with patients who did not have a concomitant BT performed (P = 0.107). The incidence of any revision surgery within 2 years was significantly lower in patients who underwent RCR with concomitant BT (4.59%) when compared with those without concomitant BT (5.83%; P < 0.001). At 2 years postoperatively, the NNT for concomitant BT to prevent a single all-cause revision surgery was 83 (Table 2).
Within 4 years, the incidence of any revision surgery was significantly lower in patients who underwent RCR with concomitant BT (5.80%) when compared with those without concomitant BT (7.53%; P < 0.001). Regarding etiology, the incidence rates of revision surgery within 4 years for RCR (P < 0.001), BT (P < 0.001), tenotomy/débridement (P < 0.001), distal claviculectomy (P < 0.001), other shoulder scope procedures (P < 0.001), and shoulder arthroplasty (P < 0.001) were significantly lower for patients with concomitant BT when compared with those without concomitant BT. At 4 years postoperatively, the NNT for concomitant BT to prevent a single all-cause revision surgery was 59 (Table 2).
When stratifying for both arthroscopic and open approaches, the incidence rates of any revision surgery examined at 2 years (open: 4.37% versus 5.95%; P < 0.001; scope: 4.64% versus 5.78%; P < 0.001) and 4 years (open: 6.00% versus 8.13%; P < 0.001; scope: 5.76% versus 7.37%; P < 0.001) were significantly lower in those who underwent concomitant BT when compared with those without concomitant BT. Among those who had a concomitant BT, there was no significant difference in 2-year (P = 0.645) and 4-year (0.675) revision BT in those undergoing arthroscopic surgery when compared with open (Table 4).
Table 4 - Univariate Analysis of 2-year Revision Surgery Rate for (A) Open Rotator Cuff Repair With or Without Open Biceps Tenodesis, (B) Arthroscopic Rotator Cuff Repair With or Without Arthroscopic Biceps Tenodesis, and (C) Open Rotator Cuff Repair With Open Biceps Tenodesis Versus Arthroscopic Rotator Cuff Repair With Arthroscopic Biceps Tenodesis Open RCR With open BT n = 4185 Open RCR Without open BT n = 20,601 Number Needed to Treat P 2-year revision surgery Rotator cuff repair 91 2.2% 643 3.1% 111 <0.001 Biceps tenodesis 24 0.6% 135 0.7% 1000 0.618 Tenotomy/débridement 64 1.5% 458 2.2% 143 0.005 Distal clavicle 18 0.4% 224 1.1% 143 <0.001 Other scope 57 1.4% 384 1.9% 200 0.030 Arthroplasty 37 0.9% 255 1.2% 333 0.064 All-cause revision surgery 183 4.4% 1225 6.0% 63 <0.001 4-year revision surgery Rotator cuff repair 107 2.6% 896 4.5% 53 <0.001 Biceps tenodesis 27 0.7% 228 1.1% 250 0.009 Tenotomy/débridement 82 2.0% 643 3.1% 91 <0.001 Distal clavicle 29 0.7% 364 1.8% 91 <0.001 Other scope 88 2.1% 603 2.9% 125
留言 (0)