
記住我



Resident physicians have been subject to an 80-hour work week and required time off between clinical activities since 2003.1 This restriction was placed to ensure patient safety with the assumption that fatigue will lead to medical errors. Studies evaluating the efficacy of work hour limits on residents have failed to demonstrate improvements in patient outcomes, and in surgical subspecialties including orthopaedics,2 there is a trend in the opposite direction. Because of resident work hour rules, patients may believe that their surgeon should be subject to duty hour restrictions.3 We were interested in evaluating the association of being on call or operating on call with objective and validated measures of surgical success for attending physicians who operated the next day for a common procedure.
Attending fatigue has not demonstrated a negative effect on outcomes in general surgical,4,5 neurosurgical,6 or cardiothoracic7,8 patients. However, this assessment is subject to variable methodologies and the inherent ambiguity of defining fatigue. In the orthopaedic literature, one retrospective review used surgical start time during the day to equate case load with fatigue9 and found increased surgical duration and a trend toward intraoperative complications in surgeries with a later start time. Other authors evaluated nighttime surgery that might be negatively affected by fatigue and10 reported increased surgical time and a trend toward increased mortality in patients who were operated on at night. Work hour restrictions for residents focus on requiring substantial time from the end of one day to the beginning of the next with the idea that a lack of a full night's sleep may affect performance. While less sleep may slow instantaneous reaction time, such as that needed for a fighter pilot, we found no data that less sleep would yield any differences in results of a non–time-dependent activity such as surgery. There is limited reporting of the influence of an attending surgeon being on call the night before surgery on surgical outcomes, and no study has yet evaluated a validated objective primary outcome.11,12
We sought to evaluate a clinically meaningful objective radiographic measure of surgical performance in the same set of attending surgeons when operating post-call vs. when not on call the night before. We used reduction and fixation of pertrochanteric hip fractures for this assessment because it is a common procedure with clearly defined objective radiographic markers of quality. This condition was chosen because, to our knowledge, there is no other reproducible, validated, objective radiographic measure for any other orthopaedic procedure that is common enough to provide power in such an assessment.
MethodsThis is a multicenter retrospective comparative cohort study. Nine sites participated, and all sites received approval from their local institutional review boards. At each site, a report of current procedural terminology codes for intertrochanteric, pertrochanteric, and subtrochanteric hip fractures (27244, 27245) was generated. From this list, patients were selected for inclusion if they were older than 18 years and were treated with either a sliding hip screw or cephalomedullary nail for a pertrochanteric hip fracture. Subtrochanteric fractures and those treated nonsurgically or with any other fixation construct were excluded. We did not exclude cases based on resident or fellow involvement because we wanted to reflect current practice, but rather recorded this information to conduct subgroup analysis. Patients were excluded if postoperative radiographs were unavailable or unacceptable in quality to evaluate. Using date of surgery, this list was then cross-referenced with available historic call schedules at each site to determine group designation: patients for whom the attending surgeon was post-call versus a control group in which attending surgeon was not post-call. In the post-call group, attending case log from their on-call period was reviewed to determine whether they operated overnight while on call, defined as 10pm to first start the following day. This allowed for a subgroup analysis of post-call surgeons who operated while on call, given that on-call status represents a spectrum of clinical demands, but having operated after 10pm the night before reliably results in decreased sleep that would be unacceptable for a resident. The study period varied from site to site based on EMR and on-call records and spanned from June 2005 to October 2019.
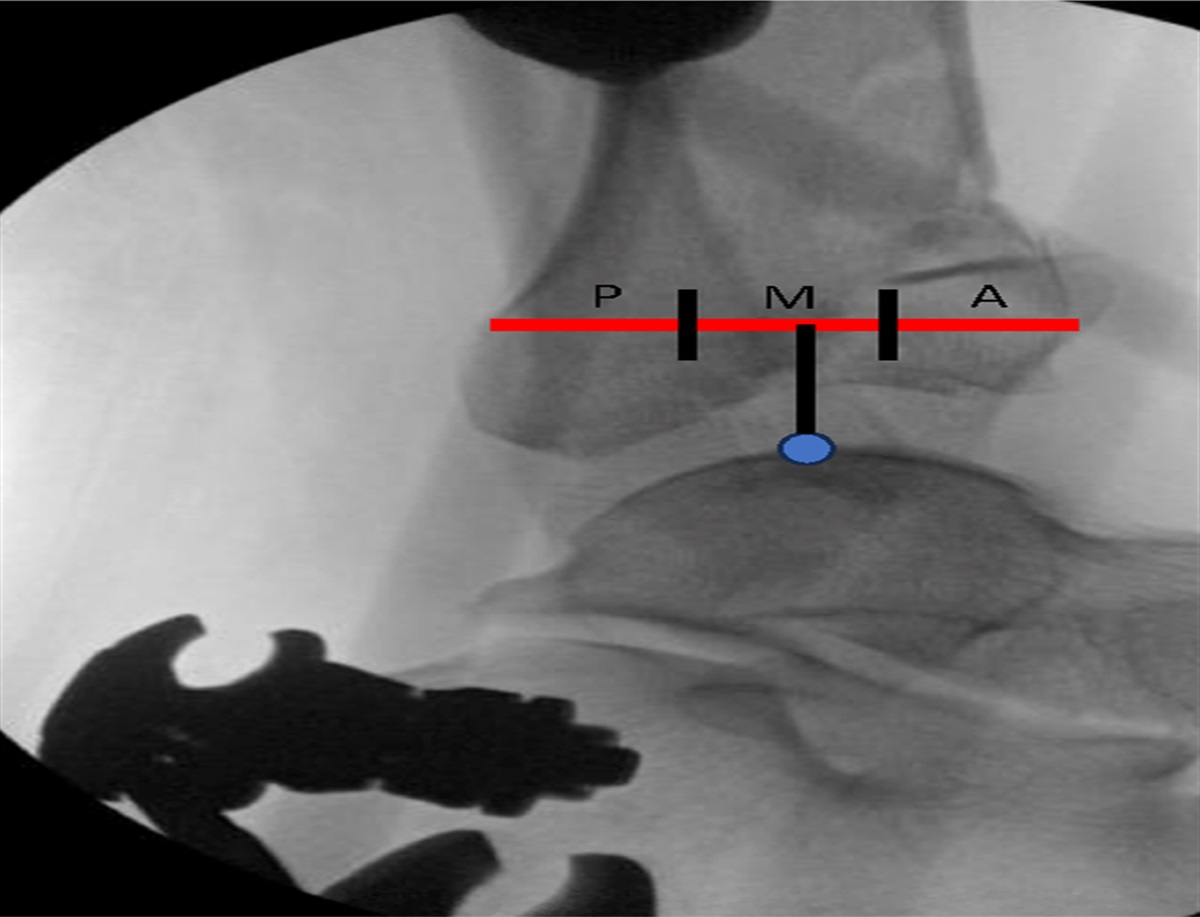
Outcomes MeasuredWe chose a common orthopaedic condition, hip fracture, and evaluated two clinically important, well-defined, validated, and reproducible radiographic outcomes. The primary outcome was corrected tip-apex distance (cTAD) because this measure has a validated threshold over which worse outcomes can be expected.13–15 A standard equation is used to correct the TAD to account for magnification of the XR, using the known implant specifications as a reference.13 The secondary outcome was Garden indices, which relate to reduction quality and are predictive of implant failure.16,17 Finally, fracture outcome and immediate perioperative complications were collected and compared.
Data CollectedPatient records were reviewed for demographic data including age, sex, BMI, and ASA classification. Fractures were classified using the Orthopedic Trauma Association classification for trochanteric region fracture, 31A.18 Side of injury was recorded, and resident involvement in each case was documented. Type of implant was designated as cephalomedullary nail with single or double screw into the neck or sliding hip screw two holes versus ≥ 4 holes, with or without trochanteric side plate. On immediate postoperative hip radiographs, corrected tip-apex distance and Garden indices were determined using the previously described methods.13,17
Site principal investigators (orthopaedic trauma surgeons) were responsible for ensuring accuracy of these measurements when evaluators were resident-level surgeons or research assistants. All evaluators were blinded to whether the surgical surgeon was on call or not. Fracture outcome was recorded when available, defined as union, malunion, nonunion, osteonecrosis, or construct failure, and secondary surgeries were documented. Perioperative complications included neurovascular injury, hematoma, superficial infection, deep infection, wound dehiscence, deep vein thrombosis, pulmonary embolism, pneumonia, respiratory failure requiring intubation, stroke, myocardial infarction, cardiac arrhythmia, urinary tract infection, decubitus ulcer, and immediate perioperative mortality during index hospitalization.
Statistical AnalysisThe R statistical software package was used to conduct statistical analysis. Descriptive statistics including median, range, and standard deviation are provided for demographic data, and chi square testing was used to compare groups. Wilcox rank-sum testing was conducted for continuous outcome variables. Categorical variables including fracture outcome and complications were compared using chi square testing. Statistical significance was set at P < 0.05, and power analysis indicated that 98 patients in each group would detect a 2-mm difference in cTAD between groups. We compared the outcomes in patients treated by physicians who were on call the night before vs. those who were treated by physicians not on call the night before. Subgroup analyses were conducted as follows: patients treated by surgeons who had operated the night before vs. those treated by surgeons not on call and cTAD between post-call and not post-call groups with and without resident involvement.
ResultsWe evaluated 1,714 patients (1,113 female, 601 male), averaging age 77 years (19 to 103) with 894 left and 820 right-sided hip fractures. There were 891 patients in the control group and 823 in the post-call group. In 66 cases, the surgeon had operated past 10 PM the night before. Average age (77 years), BMI (24.9), and ASA (III+) did not differ between post-call and control groups (P = 0.88; P = 0.22; P = 0.49 respectively). Fractures were classified as Orthopedic Trauma Association 31A1 in 1,003 patients, 31A2 in 509 patients, and 31A3 in 202 patients. Cephalomedullary nail was used in 1,364 patients and sliding hip screw in 347 (Table 1). The choice of implant did vary between sites (P < 0.001), but was similar between study groups (P = 0.11). Resident involvement varied across sites and groups (P < 0.001).
Table 1 - Patient Demographics Post-call (n = 823) Not post-call (n = 891) Sex Male 298 303 Female 525 588 Age, years 77 76.9 Side Left 450 444 Right 373 447 BMI 24 24 ASA grade I-II 159 184 III+ 664 707 OTA classification 31A1 460 541 31A2 258 251 31A3 103 99 Implant used CMN long 386 396 CMN short 288 294 SHS ≥ 4 holes 76 112 SHS 2 holes 71 88 Resident involvementa Primary 295 249 Assistant 426 513 None 71 116 Unknown 31 13CMN = cephalomedullary nail, OTA = Orthopedic Trauma Association, SHS = sliding hip screw
aStatistically significant.
Corrected TAD was 18 mm (IQR 14, 22) in the control group, 18 mm (IQR 14,21.5) in the post-call group (P = 0.59; power 90.5%), and 17 mm (IQR 14, 20.4, P = 0.25, Table 2) for patients whose surgeon operated the night before. Corrected TAD was ≥ 25 in 12.9% of patients (n = 221), 117 (13.1%) in the control group vs. 104 (12.6%) in the post-call group (P = 0.76). The rate of TAD ≥ 25 mm in the group whose surgeon had operated the night before was 6% (n = 4, P = 0.1). Garden index measurement on the AP radiograph was 160° in both the control (IQR 158, 165) and post-call (IQR 158, 164) groups. No statistical significance was found on rank-sum analysis. The Garden index on the lateral radiograph was 179° in both groups (P = 0.363). Similarly, Garden indices were not statistically different for patients whose surgeon had operated the night before (AP 161°, P = 0.84; lateral 178°, P = 0.55). When resident involvement was controlled for, we found no difference in cTAD between post-call (18 mm) and not post-call (18.8 mm) surgeries (P = 0.10).
Table 2 - Main Outcome Measure Post-call Not post-call P Operated on call P (Versus Not post-call) cTAD (mm) 18 (14, 21.5) 18 (14,22) 0.594 17 (14,20.4) 0.25 % ≥25 mm 12.6 13.1 0.76 6 0.1 Garden Index AP (Degrees) 160 (158, 164) 160 (158, 165) 0.079 161 (159, 164) 0.844 Garden Index Lateral (Degrees) 179 (175, 180) 179 (174, 180) 0.363 178 (175, 179) 0.545cTAD = corrected tip-apex distance
Fracture outcomes were available in 82.5% of patients (n = 1414). The control group experienced 10 malunions, 17 nonunions, one osteonecrosis, and four construct failures. The post-call group experienced 14 malunions, seven nonunions, two osteonecrosis, and six construct failures. The overall rate of complications was 20.6%, with 175 in the control group and 179 in the post-call group (P = 0.309, Table 3). Where fracture outcome data were available, the incidence of construct failure was 0.6% when TAD was <25 mm and 1.6% when TAD was ≥ 25 (P = 0.13).
Table 3 - Fracture Outcome Post-call n = 645 (78.4%) Operated while on call n = 54 (81.8%) Not post-call n = 781 (87.8%) Union 611 (95.5) 50 (92.6) 742 (95.9) Nonunion 7 (1.1) 1 (1.9) 17 (2.2) Malunion 14 (2.2) 2 (3.7) 10 (1.3) Osteonecrosis 2 (0.3) 0 (0) 1 (0.1) Construct failure 6 (0.9) 1 (1.9) 4 (0.5)We evaluated radiographic outcomes in a large sample of hip fracture patients treated surgically at multiple institutions to objectively evaluate the radiographic quality and complications between attending surgeons who were not on call versus those who were and those who operated past 10pm on call. We also evaluated resident involvement because, at teaching institutions, surgeon’s role may be more supervisory than technical during a standard operation such as hip fracture repair. We used the reproducible and validated measure of tip-apex distance as our primary indicator of surgical quality along with the Garden indices as a representation of reduction quality. The overall rate of unacceptable corrected TAD was high enough (13%) to allow for statistical comparison between these groups (powered to show a 3% difference). Baumgartner13 initially published that TAD >25 mm had a markedly increased risk of cutout in 198 hip fractures treated with a sliding hip screw (1995). No constructs with TAD ≤ 25 mm experienced cutout, but 16 cutout events occurred when TAD was >25 mm. Subsequently, this measure was applied to cephalomedullary devices with similar findings. In a case-control analysis, Lobo-Escolar et al.14 found a mean TAD of 32.2 mm in their cutout group versus 23.8 mm in the control group. On retrospective review, Gellar et al.15 found a 44% rate of cutout when the TAD exceeded 25 mm, which was markedly higher than the overall rate of failure of 8.5% in their population.
In our study population, there was no statistical difference in cTAD between the post-call and control groups (P = 0.59), and this remained true when subgroup analysis was conducted on patients whose surgeon had operated the night before while on call (P = 0.25) and patients whose surgeon did not have a resident assistant (P = 0.1). We also found no difference in Garden indices, which have also been correlated with fracture outcome,16 for post-call surgeons or post-call surgeons who operated when on call. In addition, the percentage of hip fractures that went on to union does not differ between groups (95.5% post-call, 95.9% control, P = 0.23). For those whose fracture outcome was available, our rate of revision surgery (2.7%) was consistent with prior reports in the literature.13,15,19,20 Finally, there was no difference seen in summed complications for patients treated by surgeons who were not on call, post-call, or post-call having operated past 10pm.
This is the first study to evaluate surgical quality using validated, objective, and clinically important outcome measures for surgeons who were on call or operated on call the night before a commonly performed procedure such as hip fracture repair. A more frequently studied outcome is incidence of complications, albeit with different definitions of surgeon fatigue and different patient populations. Peskun et al.9 used primary arthroplasty case start time, split into daily quartiles, to look at patient outcomes, assuming that a later start time corresponds to a more fatigued surgeon. They found no statistical difference in any variables among the TKA cohort, and in the THA group, the only statistically significant findings were an increase in surgical time of 7 minutes and a trend toward a higher incidence of periprosthetic femur fracture between the first and fourth quartiles.
In our study, the most common complications were UTI (n = 108), cardiac arrhythmia (n = 69), and pneumonia (n = 64) (Figure 1). The summed complication rate was 20.6% and was not different between groups (P = 0.309). These complication rates are similar to prior reports in the literature.21 Two fatigue-related studies have been published, which include subsets of orthopaedic surgeons in their analyses, including one by Govindarajan et al.,11 which found no increased odds ratio for death, complications, or readmission in elective hip and knee arthroplasty patients or hip fracture repair patients when their physician had performed clinical duties the night before surgery. A separate report from Rothschild et al.,12 which included a small number of orthopaedic attendings in its analysis, also failed to find a notable increase in the odds ratio for having a complication after a post-nighttime procedure. The authors did, however, find that when a surgeon's “sleep opportunity” was numbered 6 hours or less, the odds ratio became notable. This is at odds with our finding of no perioperative mortalities when the surgeon was known to have operated the night before. It was in this cohort that the surgeon “sleep opportunity” was known to have been decreased.
 Figure 1:
Figure 1: Graph showing postoperative complications. Overall incidence 20.6%, P = 0.28. Statistical significance found for UTI, perioperative mortality, and respiratory failure requiring reintubation. No significance found on subgroup analysis for surgeons who operated while on call. UTI = urinary tract infection; SSI = surgical site infection; DVT = deep vein thrombosis; PE = pulmonary embolism; NV = neurovascular
While this study is retrospective, the nature of the data is robust. Call schedules were able to be confirmed, and the radiographic outcomes were evaluated specifically for this study without knowledge of the status of the surgeon who had done the case. Complications were based on chart review and are limited because all are retrospective studies. We also noted that across sites, there were heterogeneous implant choices and a wide array of resident involvement. This variability makes our results generalizable to standard practice. A main limitation of the study involves the procedure investigated. While surgical repair of an intertrochanteric fracture is a routinely performed procedure across practice settings, it does not, in all cases, require advanced technical skill. Care should be taken when extrapolating the results of this study to cases with a high level of complexity that may be more susceptible to surgeon fatigue.
In addition, it is worth noting that fatigue remains an ambiguous and subjective descriptor, and future investigations should seek to validate an objective measure thereof. For example, modern activity trackers worn by surgeons would provide discrete data beyond “sleep opportunity”. The subgroup analysis including surgeons operating on call, as previously mentioned, was used in this study to identify surgeons who may have been operating in a fatigued state. Having operated at any point within those noncivilian hours would result in a decreased “sleep opportunity” if one makes the logical assumption that sleep opportunity does not begin with procedure end time and end at the time of incision the next morning. One must account for postoperative charting, commute, personal care and home tasks, and morning routine and commute, for example.
As a separate but related issue, there is no empirically derived answer to the question posed of whether a call night with limited calls results in the same rest as a non-call night; however, published results of a survey by the ACS correlated increased number of nights on call per week with higher burnout, worse emotional health, more conflicts at home, and worse career satisfaction.22 Given the inherent variability in burden of a night on call, this suggests there is a baseline stress response that accompanies being on call, likely affecting the restfulness independent of call burden. This would certainly vary by practice setting and volume. The authors were also interested, however, in the ability of the post-call surgeon, in general, to perform the procedure, without necessarily an obligation (outside of the operated on call subgroup) to be fatigued in the post-call state. This makes the results more generalizable to the reality of taking call.
ConclusionIn this multicenter review, objective surgical quality based on validated radiographic outcomes and clinical outcomes for a common procedure were not negatively affected when the attending orthopaedic surgeon had been on call or had operated on call the night before surgery.
References 1. Burchiel KJ, Zetterman RK, Ludmerer KM, et al.: The 2017 ACGME common work hour standards: Promoting physician learning and professional development in a safe, humane environment. J Graduate Med Educ 2017;9:692-696. 2. Baldwin K, Namdari S, Donegan D, Kamath AF, Mehta S: Early effects of resident work-hour restrictions on patient safety: A systematic review and plea for improved studies. The J Bone Jt Surg Am Vol 2011;93:e5. 3. Berg DB, Engel AM, Saba A, Hatton EK: Differences in public belief and reality in the care of operative patients in a teaching hospital. J Surg Educ 2011;68:10-18. 4. Sharpe JP, Weinberg JA, Magnotti LJ, et al.: Outcomes of operations performed by attending surgeons after overnight trauma shifts. J Am Coll Surg 2013;216:791-799. 5. Zafar SN, Libuit L, Hashmi ZG, et al.: The sleepy surgeon: Does night-time surgery for trauma affect mortality outcomes? Am J Surg 2015;209:633-639. 6. Bekelis K, Missios S, Mackenzie TA: Outcomes of elective cerebral aneurysm treatment performed by attending neurosurgeons after night work. Neurosurgery 2018;82:329-334. 7. Chu MWA, Stitt LW, Fox SA, et al.: Prospective evaluation of consultant surgeon sleep deprivation and outcomes in more than 4000 consecutive cardiac surgical procedures. Arch Surg 2011;146:1080-1085. 8. Ellman PI, Law MG, Tache-Leon C, et al.: Sleep deprivation does not affect operative results in cardiac surgery. Ann Thorac Surg 2004;78:906-911. 9. Peskun C, Walmsley D, Waddell J, Schemitsch E: Effect of surgeon fatigue on hip and knee arthroplasty. Can J Surg J canadien de chirurgie 2012;55:81-86. 10. Chacko AT, Ramirez MA, Ramappa AJ, Richardson LC, Appleton PT, Rodriguez EK: Does late night hip surgery affect outcome? J Trauma 2011;71:447-453. 11. Govindarajan A, Urbach DR, Kumar M, et al.: Outcomes of Daytime procedures performed by attending surgeons after night work. New Engl J Med 2015;373:845-853. 12. Rothschild JM, Keohane CA, Rogers S, et al.: Risks of complications by attending physicians after performing nighttime procedures. J Am Med Assoc 2009;302:1565-1572. 13. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM: The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am Vol 1995;77:1058-1064. 14. Lobo-Escolar A, Joven E, Iglesias D, Herrera A: Predictive factors for cutting-out in femoral intramedullary nailing. Injury 2010;41:1312-1316. 15. Geller JA, Saifi C, Morrison TA, Macaulay W: Tip-apex distance of intramedullary devices as a predictor of cut-out failure in the treatment of peritrochanteric elderly hip fractures. Int Orthopaedics 2010;34:719-722. 16. Pervez H, Parker MJ, Vowler S: Prediction of fixation failure after sliding hip screw fixation. Injury 2004;35:994-998. 17. Garden RS: Low-angle fixation in fractures of the femoral neck. The J Bone Joint Surg Br Vol 1961;43-B:647-663. 18. Meinberg E, Agel J, Roberts C, Karam MD, Kellam JF: Fracture and Dislocation classification compendium-2018. J Orthop Trauma 2018;32Suppl 1:S1-S170. 19. Andruszkow H, Frink M, Fromke C, et al.: Tip apex distance, hip screw placement, and neck shaft angle as potential risk factors for cut-out failure of hip screws after surgical treatment of intertrochanteric fractures. Int Orthop 2012;36:2347-2354. 20. Matre K, Havelin LI, Gjertsen JE, Espehaug B, Fevang JM: Intramedullary nails result in more reoperations than sliding hip screws in two-part intertrochanteric fractures. Clin Orthop Relat Res 2013;471:1379-1386. 21. Lawrence VA, Hilsenbeck SG, Noveck H, Poses RM, Carson JL: Medical complications and outcomes after hip fracture repair. Arch Intern Med 2002;162:2053-2057. 22. Shanafelt TD, Balch CM, Bechamps GJ, et al.: Burnout and career satisfaction among American surgeons. Ann Surg 2009;250:463-471.
留言 (0)