
記住我

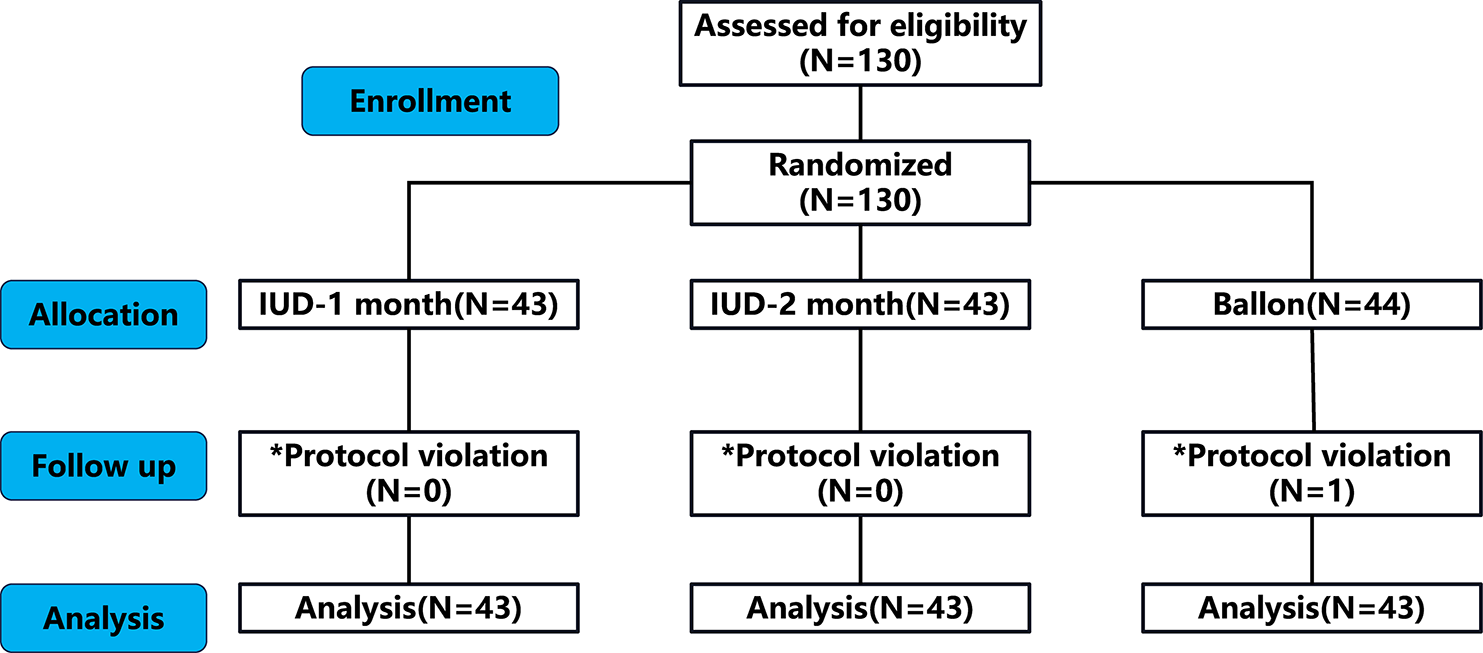
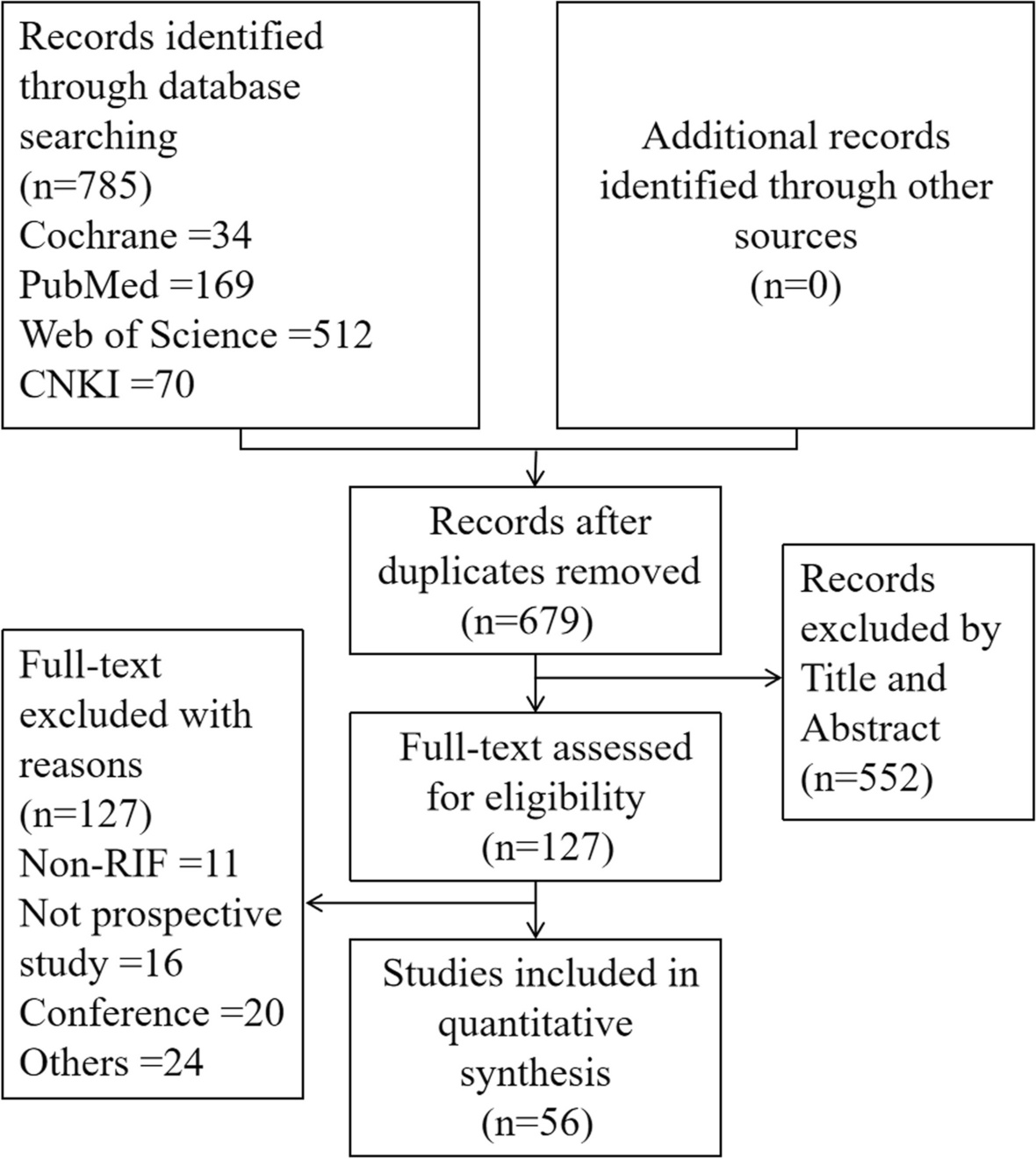
The search identified 4149 citations after removing duplicates, among which 27 RCTs [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47] with 4608 participants met the eligibility criteria and were included in the meta-analysis (Fig. 1). The sample size of the included studies ranged from 25 to 750, and the publication years were 2001 to 2021. The mean age of all participants was 27.67 years, and the mean infertility duration was 2.45 years. The mean BMI of subjects in these RCTs ranged from 20.8 to 38.4 (Supplementary Table 2).
Fig. 1
PRISMA flow diagram of screening literatures
In addition to placebo, a total of 11 types of pharmacological treatments were included in these studies: CC, LZ, MET, PIO, exenatide (EXE), tamoxifen, dual therapy with CC + MET, LZ + MET, CC + ROS, CC + EXE, and triple therapy with CC + MET + PIO. Two placebo-controlled RCTs and 25 head-to-head RCTs were included in our review. CC monotherapy was the most frequently investigated treatment in 18 studies. Dual therapy with CC + MET was involved in 13 studies. LZ and MET were also commonly used: 8 studies used LZ, and 11 studies used MET monotherapy. Five studies used TZDs (PIO or ROS) as monotherapy [39, 43] or in combination with CC [36, 41] or CC + MET [25]. Two studies used EXE as monotherapy or in combination with CC [34, 45]. Only one trial compared tamoxifen (TAM), a synthetic antiestrogen drug, with CC and LZ [38]. The network of all comparisons for the primary and secondary outcomes for efficacy are presented in Fig. 2.
Fig. 2
Network plot for the included trials comparing different pharmacological treatments for PCOS women. MET, metformin; CC, clomiphene citrate; PIO, pioglitazone; LZ, letrozole; ROS, rosiglitazone; EXE, exenatide; TAM, tamoxifen
Effects of first-line pharmacological treatments in clinical pregnancyAll 27 trials compared each intervention or placebo clinical pregnancy in women with PCOS. Network meta‐analysis showed that most pharmacological treatments (LZ, MET, PIO, EXE, CC + MET, LZ + MET, CC + EXE and CC + MET + PIO) resulted in a significantly elevated clinical pregnancy in infertile women with PCOS compared with placebo (Fig. 3A). The pioglitazone (log OR 3.14, 95% CI 1.56 ~ 4.70; NNT 0.38; moderate confidence), CC + EXE (log OR 2.96, 95% CI 1.07 ~ 4.82, NNT 0.46, moderate confidence) and CC + MET + PIO (log OR 2.82, 95% CI 0.99 ~ 4.60, NNT 0.53, moderate confidence) groups obtained a superior clinical pregnancy than the other interventions. However, there was no statistically significant impact of CC alone (log OR 1.20, 95% CI -0.02 ~ 2.35, very low confidence), CC + ROS (log OR 1.62, 95% CI -0.02 ~ 3.24, very low confidence), or TAM alone (log OR 1.65, 95% CI -0.12 ~ 3.34, very low confidence) on clinical pregnancy (Fig. 3A, Supplementary Table 5A).
Fig. 3
Forest plot for outcomes of different pharmacological treatments compared with placebo. OR, odds ratio; CI, credibility interval; NNT, number needed to treat; NNH, number treated to harm; NA, not applicable
The league table demonstrated that CC alone tended to be less effective than the other monotherapies or combination treatments, especially CC + EXE, LZ, CC + MET, CC + MET + PIO, LZ + MET, and PIO. However, there was no significant difference in most pairwise comparisons of these pharmacological interventions (Supplementary Table 3A). In addition, the possibility rank suggests that among the 11 pharmacological interventions, pioglitazone, CC + EXE, CC + MET + PIO and EXE might increase the clinical pregnancy most effectively for infertile PCOS women (Fig. 4A).
Fig. 4
The ranking probability histogram for the outcomes. The color of the bar indicates the possibility rank of outcomes and the larger the proportion of dark colors, the higher the ranking
Effects of first-line pharmacological treatments on live birth rateThirteen studies evaluated the effect of eight pharmacological treatments, including CC, LZ, MET, PIO, CC + MET, LZ + MET, CC + ROS and CC + MET + PIO, on the live birth rate. A trend toward an improved live birth rate in patients who had received pharmacological therapy was noted, but it was not found to be statistically significant (Fig. 3B). It is noted that CC + MET + PIO (log OR 1.62, 95% CI -0.25 ~ 6.06, very low confidence) could increase the live birth rate most when compared to placebo (Supplementary Table 2B, 5B), and the probability rank also suggested that CC + MET + PIO was superior for improving the live birth rate (Fig. 4B). The league table showed that all pairwise comparisons were not statistically significant (Supplementary Table 3B).
Effects of first-line pharmacological treatments on miscarriage rate, ectopic pregnancy and multiple pregnancyThe miscarriage rate of 8 interventions, which was identical to the live birth rate, was compared in 15 trials. Most of these pharmacological treatments played relatively minor roles in miscarriage when compared with the placebo group (Fig. 3C). However, PCOS patients who received PIO showed a tendency to have an increased miscarriage rate (log OR 0.15, 95% CI -3.64 ~ 4.36, very low confidence), which requires more direct evidence (Fig. 4C, Supplementary Table 3C, 5C).
Only 8 studies provided the outcome of ectopic pregnancy involving five interventions: CC, LZ, MET, CC + MET, and LZ + MET. None of the five interventions increased ectopic pregnancy for PCOS women compared to placebo. Among these, MET (log OR -11.25 95% CI -33.7 ~ 0.57, low confidence) and LZ + MET (log OR -10.44 95% CI -59.56 ~ 42.11, very low confidence) seemed to be beneficial in decreasing ectopic pregnancy (Fig. 3D).
For multiple pregnancy, six interventions, including CC, LZ, CC + MET, CC + MET + PIO, MET, and CC + ROS, were assessed. All of them except MET alone (log OR 0.07 95% CI -4.26 ~ 4.34, low confidence) significantly increased the multiple pregnancy rate (Fig. 3E). However, it made no sense to estimate the effect of ectopic pregnancy and multiple pregnancy in this network meta-analysis because the occurrence of the two adverse events was extremely low in these studies.
Heterogeneity, inconsistency, and sensitivity assessmentThe inconsistency test showed that the clinical pregnancy and live birth rate results were consistent in the direct, indirect and network analyses except for the comparison of CC + MET and MET (Supplementary Fig. 1), and the sensitivity analysis, which used frequentist methods to perform the network meta-analysis, showed similar results, even though the 95% CI was narrower than the results from the Bayes method (Supplementary Fig. 2).
However, significantly high heterogeneity existed in the comparison of CC and MET and MET and CC + MET in the primary outcome. Clinical pregnancy also had high heterogeneity in the comparison between MET and placebo. The heterogeneity in the comparison of CC with CC + MET was moderate, and the other comparisons had low heterogeneity in the analysis (Supplementary Fig. 3A&B). Nevertheless, the heterogeneity was decreased to some extent after subgroup analysis (Supplementary Fig. 3F&G).
For the secondary outcome, heterogeneity was low to moderate for most trials (Supplementary Fig. 3C-E). Unfortunately, sensitivity assessment and subgroup analysis were not accomplished due to the lack of data for the second outcome.
Meta-regression and subgroup analysisThe results of the meta-regression showed that baseline demographic characteristics, including age, BMI, region, duration of infertility and length of treatment, had no effect on clinical pregnancy and live birth (Supplementary Table 3). However, the potential effect of the variables could not be fully excluded based on negative results because meta-regression may underestimate some small associations. Thus, we performed subgroup analysis with different BMI cut-off points for pregnancy outcome.
The results showed that only one East Asian study included a population with normal BMI, while one East Asian and eight non-East Asian trials included obese populations. In addition, one East Asian study and twelve non-East Asian studies included overweight patients. To obtain sufficient data for the network meta-analysis, we finally divided these studies into obese and nonobese subgroups. In the obese group, no significant difference was found among these medications, including CC, EXE, LZ, MET, CC + MET, PIO, and CC + ROS, when compared with placebo (Supplementary Fig. 4A), whereas in the nonobese group, these medications showed an effect of increasing the clinical pregnancy in women with PCOS except for CC and TAM (Supplementary Fig. 4B).
Quality assessment and the risk of biasOnly seven studies were at a low risk of bias for all components and seven studies were at a high risk of bias. The main biases were caused by failure of blinding of the participants and personnel and incomplete outcome data. For blinding of the outcome assessment, due to the particularity of pregnancy, we considered all studies to have a low risk of bias in this aspect (Supplementary Fig. 5).
The funnel plot and test were visually symmetrical, which indicated that there was no publication bias in the primary outcome (Supplementary Fig. 6). The CINeMA confidence of results showed moderate to very low confidence grades, mainly due to concerns about within-study bias, heterogeneity and imprecision owing to low numbers of trials for some comparisons (Supplementary Table 5).
留言 (0)