
記住我










A central venous catheter is a commonly performed procedure. The indications include hemodynamic monitoring, intravenous drug therapy, parenteral nutrition, hemodialysis, and rapid fluid resuscitation.[1] Central venous catheter insertion was traditionally performed with landmark techniques. The introduction of ultrasound guidance has greatly improved the safety of central venous catheters.[1] However, complications such as inadvertent arterial injury do occur occasionally even in experienced hands. We hereby report a case of inadvertent injury of the right subclavian artery during central venous catheter insertion with subsequent embolization of the right internal mammary artery and stenting of the right subclavian artery.
CASE REPORTA 40-year-old man with a past medical history of pulmonary tuberculous, hepatitis B, and hepatitis C was admitted to the hospital for sudden abdominal pain. CT of the abdomen revealed a large left hemoperitoneum secondary to rupture of a left renal artery pseudoaneurysm. The patient underwent left total nephrectomy after two failed left renal artery embolization procedures. The histological diagnosis was polyarteritis nodosa. The patient was transferred to the ICU for further management and a central venous catheter was inserted with the landmark technique for renal replacement therapy. During his stay, the patient was agitated and self-pulled out his central venous catheter. The clinical team tried to reinsert the central venous catheter with the landmark technique. The procedure was challenging as the patient was confused and uncooperative. An arterial injury was suspected as bright red blood was aspirated when the operator inserted the catheter. The central venous catheter was immediately removed for hemostasis by external compression. CT angiogram of the neck showed contrast extravasation at the junction between the right subclavian artery and internal mammary artery. The endovascular approach to repair the arterial injury was chosen due to difficult surgical access [Figure 1a-c].
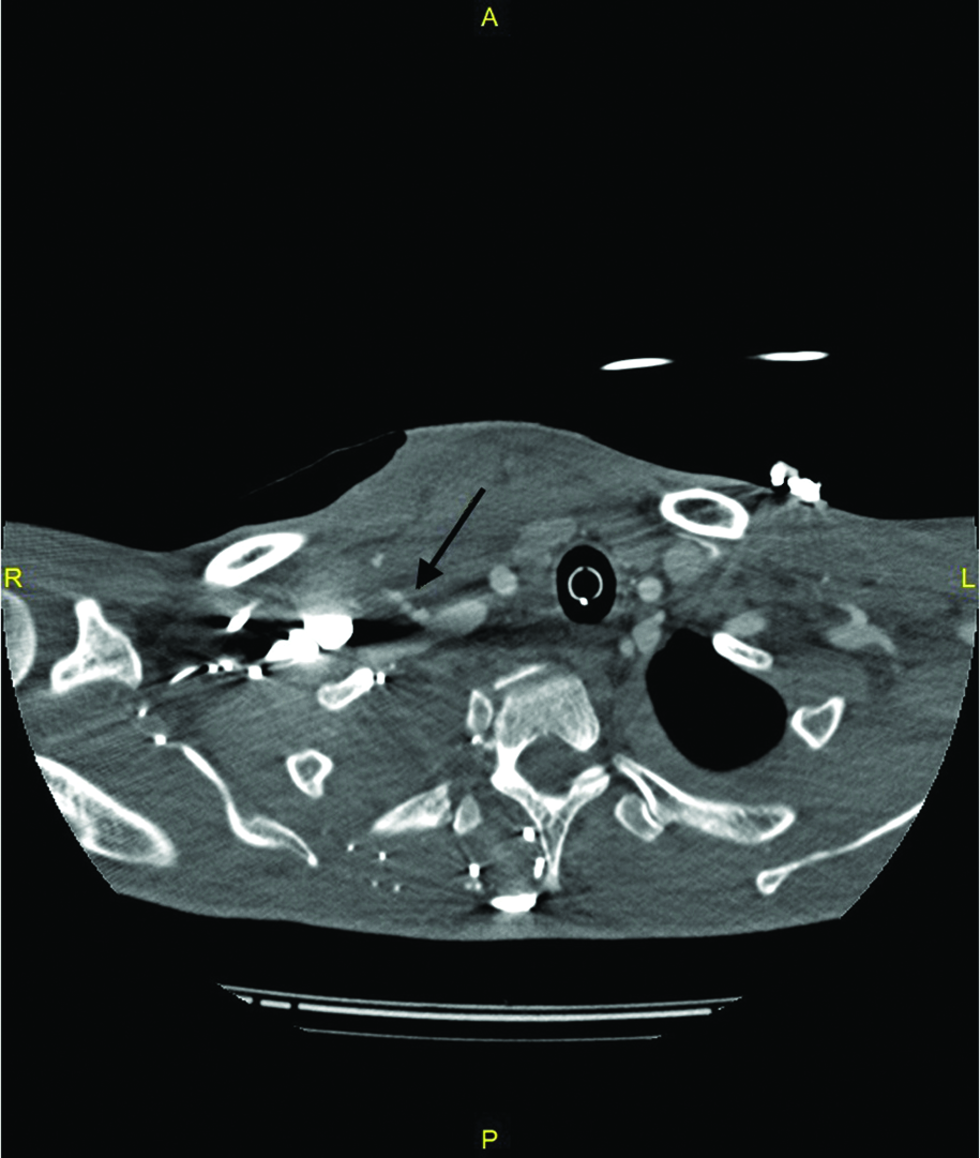
Figure 1a:: 40-year-old man with suspected arterial injury after central venous catheter insertion. (a) CT angiogram(axial) of the neck showed contrast extravasation(arrow) at the junction between the right subclavian artery and internal mammary artery.
Export to PPT
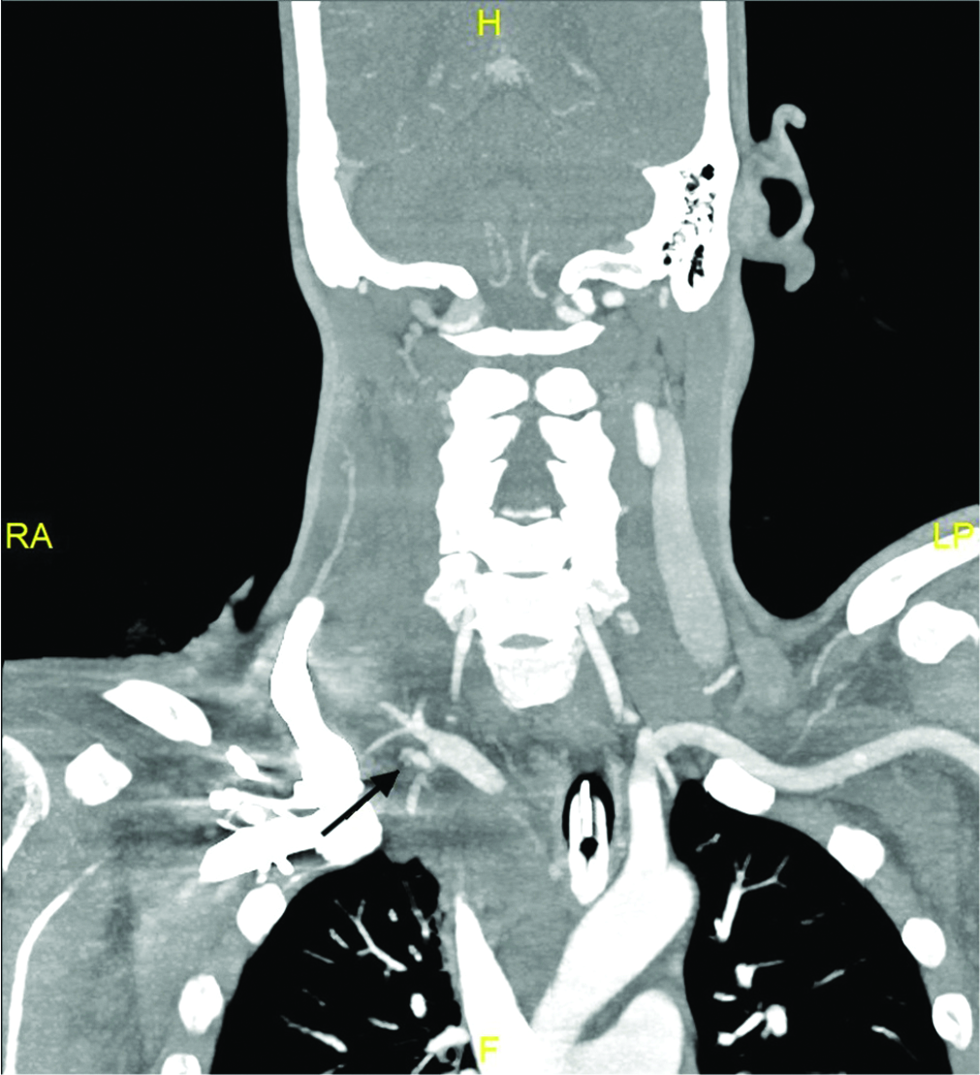
Figure 1b:: 40-year-old man with suspected arterial injury after central venous catheter insertion. (b) CT angiogram(coronal) of the neck showed contrast extravasation(arrow) at the junction between the right subclavian artery and internal mammary artery.
Export to PPT

Figure 1c:: 40-year-old man with suspected arterial injury after central venous catheter insertion. (c) CT angiogram(sagittal) of the neck showed contrast extravasation(arrow) at the junction between the right subclavian artery and internal mammary artery.
Export to PPT
Digital subtracted imaging (DSA) of the right subclavian artery was performed using the right brachial approach. After a 5Fr arterial sheath (Terumo, Tokyo, Japan) was inserted, the right subclavian artery was cannulated with a C1 catheter (Cook Medical, Bloomington, Indiana). DSA showed contrast extravasation at the junction between the right subclavian artery and the internal mammary artery [Figure 2a]. In view of the proximity between the internal mammary artery and the site of injury, the right internal mammary artery was embolized before placing a covered stent in the right subclavian artery. Coil embolization of the right internal mammary artery was performed using Nestor (Cook Medical, Bloomington, Indiana) and Interlock coils (Boston Scientific, Marlborough, Massachusetts) through a 2.5Fr Renegade microcatheter (Boston Scientific, Marlborough, Massachusetts).

Figure 2a:: Digital subtracted imaging (DSA) of the right subclavian artery. The right internal mammary artery was sacrificed with coil embolisation before right subclavian artery reconstruction. (a)DSA shows contrast extravasation(arrow) at the junction between the right subclavian artery and internal mammary artery
Export to PPT
Post embolization DSA of the right internal mammary artery showed no distal flow but persistent contrast extravasation from the proximal internal mammary artery [Figure 2b]. A stent graft was placed in the right subclavian artery to reconstruct the vessel. The origin of the right vertebral artery was included in the landing zone of the covered stent. However, in view of the right vertebral artery being non-dominant and it was a lifesaving procedure, the right vertebral artery was sacrificed. A Begraft (Bentley Innomed, Hechingen, Germany) peripheral stent (9 mm x 3.7 cm) was chosen. A 7Fr arterial sheath (Terumo, Tokyo, Japan) was exchanged at the right brachial artery. Deployment of the covered stent was then performed with the aid of a pressure inflator. The proximal end of the stent was deployed distal to the origin of the right subclavian artery while the distal end was deployed distal to the origin of the right thyrocervical trunk [Figure 3a]. Mild contrast extravasation was noted after the stent deployment and balloon angioplasty was performed using a 10 mm Mustang balloon (Boston Scientific, Marlborough, Massachusetts) [Figure 3b-c]. Post-procedure DSA showed no contrast extravasation at the right subclavian artery [Figure 3d].

Figure 2b:: Digital subtracted imaging (DSA) of the right subclavian artery. The right internal mammary artery was sacrificed with coil embolisation before right subclavian artery reconstruction. (b) DSA of the right internal mammary artery after embolisation shows no distal flow but contrast extravasation(arrow) from the proximal internal mammary artery.
Export to PPT

Figure 3a:: 40-year-old man with right subclavian artery injury after central venous catheter insertion. A peripheral stent graft is deplored in right subclavian artery after right internal mammary artery embolization. (a) A Begraft peripheral stent (arrow) was deplored in right subclavian artery.
Export to PPT

Figure 3b:: 40-year-old man with right subclavian artery injury after central venous catheter insertion. A peripheral stent graft is deplored in right subclavian artery after right internal mammary artery embolization. (b) DSA of right subclavian artery shows persistent contrast extravasation(arrow) after the stent deployment.
Export to PPT

Figure 3c:: 40-year-old man with right subclavian artery injury after central venous catheter insertion. A peripheral stent graft is deplored in right subclavian artery after right internal mammary artery embolization. (c) Balloon angioplasty was performed using a 10 mm Mustang balloon(arrow)
Export to PPT
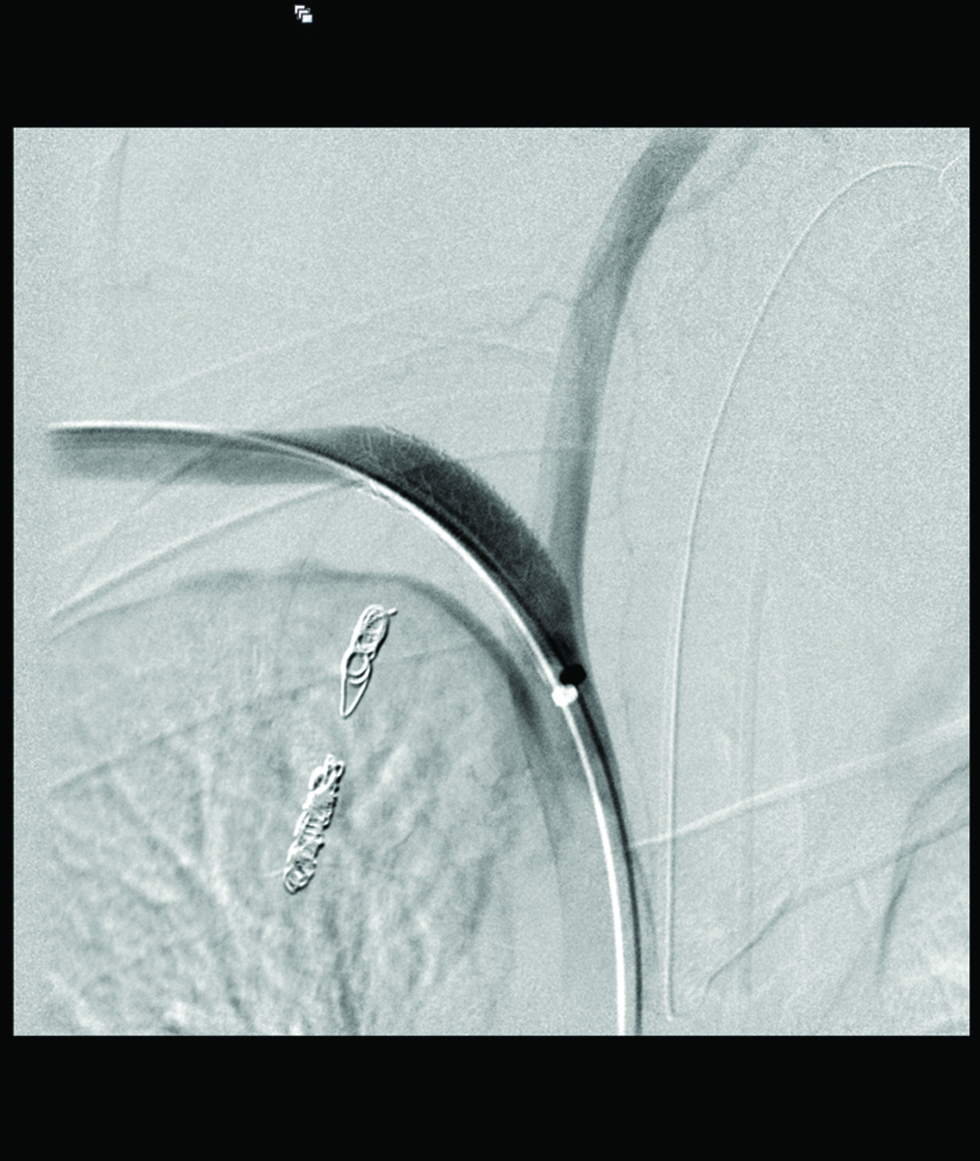
Figure 3d:: 40-year-old man with right subclavian artery injury after central venous catheter insertion. A peripheral stent graft is deplored in right subclavian artery after right internal mammary artery embolization. (d) Post balloon angioplasty DSA of right subclavian artery showed no further contrast extravasation.
Export to PPT
DISCUSSIONComplications of central venous catheter insertion include arterial puncture, malpositioning of the central venous catheter, pneumothorax, air emboli, great vessel perforation, infection, and venous thrombosis.[2] There are a few factors that increase the difficulty of central venous catheter insertion, including obesity, a short neck, and anxious patient. Inadvertent arterial puncture involving a small needle (22G or 25G) is often without significant consequences. It is probably underreported and more commonly seen than in literature. However, the result of an inadvertent arterial injury with a large-bore catheter can be devastating if it goes unrecognized. These complications include hematoma, airway compression, pseudoaneurysm, arteriovenous fistula, and stroke[1]
In order to minimize the risk of inadvertent arterial puncture, all central venous catheter insertions should be performed with real-time ultrasound guidance if the equipment and expertise are available. Saguel et al. suggested a six steps approach in ultrasound-guided central line placement. The suggested steps are 1. identify the anatomy of the insertion site and localization of the vein. 2. Confirm patency of the vein. 3. Use of real-time US guidance for puncture of the vein 4. Confirm needle position in the vein 5. Confirm guidewire position in the vein 6. Confirm catheter position in the vein.[3]
Optimal patient position is crucial to minimize inadvertent arterial puncture. The patient should be placed in the Trendelenburg position (10°-20° head down) with the neck rotate 30° away from the puncture site. According to the literature, rotating the neck more than 40° would increase overlapping between the internal jugular vein and the carotid artery and thus increase the chance of arterial puncture.[4]
Management of a serious cervicothoracic arterial injury during central venous catheter insertion depends on the several factors, including the site and extent of the injury, patient stability, catheter diameter, whether the catheter is still in place, and neurological status of the patient.[1] They can be broadly divided into 1. external compression 2. endovascular intervention and 3. direct surgical repair. The present data shows that arterial catheterization with a 7Fr or larger catheter is associated with high morbidity. Therefore, if the arterial injury involves a large-bore central venous catheter (7Fr or larger), the central venous catheter should be left in situ and seek endovascular or surgical repair depending on the site of injury. Endovascular techniques are ideal for arterial injury below or behind the clavicles as surgical exploration would be difficult in these cases.[1]
The endovascular techniques include the use of a percutaneous closure device and stent-graft placement. In general, a percutaneous closure device is favored if there is no vascular abnormalities (ie. thrombosis, AV fistula, arterial dissection).[5] The available closure devices fall into two major groups; those that use collage plugs at the arteriotomy site and those that deploy sutures at the arteriotomy site. They can produce hemostasis at the arteriotomy site regardless of the anticoagulation status.[6] It has a low complication rate and the complications include hematoma, arterial compromise (stenosis, occlusion, embolization), false aneurysm or arteriovenous fistula.[6] In our case, removal of the central venous catheter precluded the use of a percutaneous closure device.
We successfully treated the right subclavian artery injury with a stent-graft. In our case, we used a trans-brachial approach instead of the more traditional transfemoral approach in view of the shorter course to the injured arterial segment. The stent grafts can be a self-expanding type or a balloon-mounted type. The selection of a suitable stent-graft depends on the size of the vessel, length of the lesion, stent types, and location (whether the stent would cover any branches from the parent vessel).[7] The downside of covered stent placement is the need for long-term antiplatelet medication, and the higher rate of stroke compared with a percutaneous closure device.[5] Potential complications of stent-graft include stent graft infection, vessel occlusion, endoleak, stent extrusion, and cerebrovascular accident.[8]
CONCLUSIONThis case report highlights the role of endovascular therapy in managing arterial injuries associated with in central venous catheter insertion. If an arterial injury is suspected during venous catheterization, the catheter should be left in situ and obtain cross-sectional imaging. An endovascular or surgical approach to repair the injured artery is safer than pull and press techniques.
留言 (0)